Embed Size (px)
Citation preview

Cellular Allograft in the Treatment Cellular Allograft in the Treatment of a Severe Periodontalof a Severe Periodontal
Intrabony Defect: Intrabony Defect: A Case ReportA Case Report
Samuel Koo,* Abdulmonem Alshihri,† Nadeem Y. Karimbux,* Mohamed Maksoud*
REPORTER: Janine RumbaoaREPORTER: Janine Rumbaoa

Radiograph of the periodontal distal defect of tooth #9 showingthe extent of the bone loss close to the apex of the tooth
INTRODUCTION
• This report describes the use of allograft cellular bone matrix containing mesenchymal stem cells in the treatment of a severe periodontal defect.

CASE PRESENTATIONgeneralized severe
periodontitis
severe radiographic defect on the distal aspect of tooth #9 extending
to the apex of the tooth.
the tooth was vital
After thorough debridement, the defect was grafted with cellular
allograft and covered with resorbable membrane.
Nine months after grafting, the periapical radiograph
demonstrated bone fill of the defect.
The postoperative clinical examination revealed
gain in the clinical attachment level and reduction in the probing
depth. In addition, the tooth maintained its vitality
TERMINOLOGY
• ALLOGRAFTALLOGRAFTA graft of tissue obtained from a donor
genetically different from, though of the
same species as the recipient.
Also called allogenenic graft,
allogeneic homograft,
homograft, homologous graft, homoplastic graft.

CLINICAL PRESENTATION
• A healthy 39-year-old male• Extensive periodontal and implant treatment.• The patient reported a past dental history of
orthodontic treatment to correct a Class III malocclusion.
• periodontal examination revealed generalized severe periodontitis with mobility of several teeth, recession, and severe gingival inflammation together with heavy supragingival and subgingival calculus accumulation.
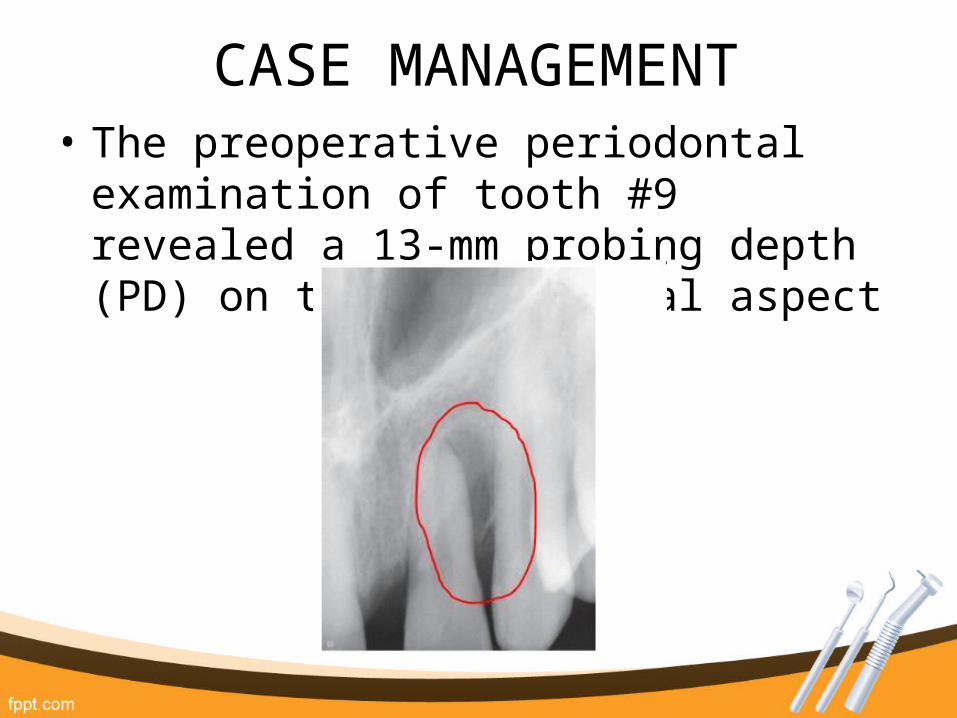
CASE MANAGEMENT• The preoperative periodontal examination
of tooth #9 revealed a 13-mm probing depth (PD) on the distopalatal aspect

• Local anesthesia was administered, and full-thickness mucoperiosteal flaps were reflected without vertical releasing incisions
• The periodontal defectwas thoroughly debrided.
The defect after the flap elevation and debridement.
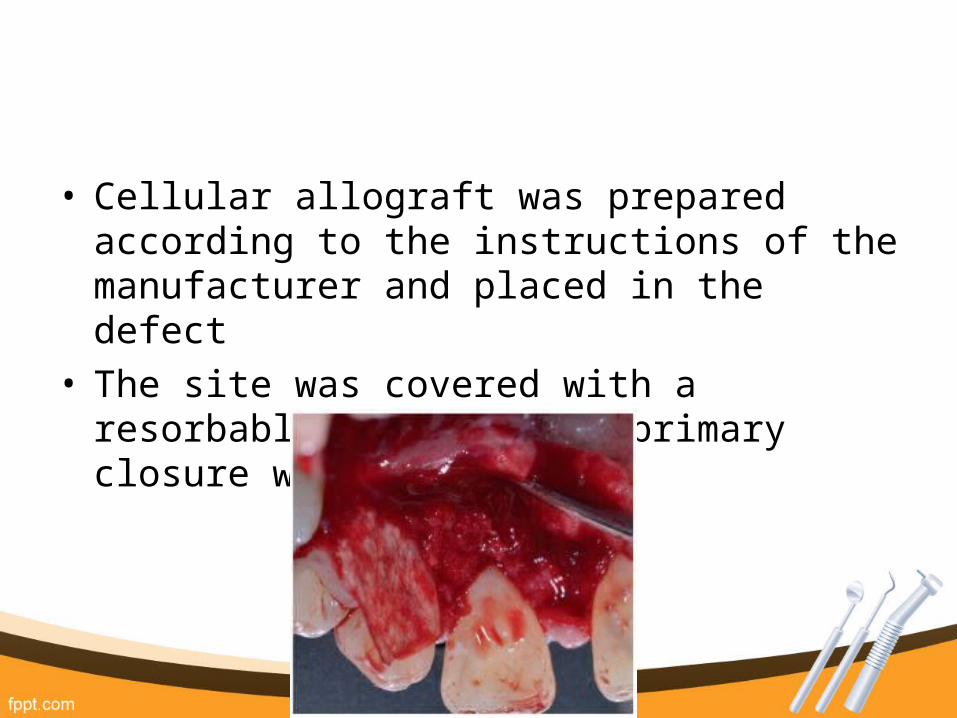
• Cellular allograft was prepared according to the instructions of the manufacturer and placed in the defect
• The site was covered with a resorbable membrane and primary closure was obtained

CLINICAL OUTCOMES
• Nine months after the grafting, there was a significant improvement in the periodontal parameters except for the reverse architecture between teeth #9 and #11

• There was a significant reduction of the PD and a gain of clinical attachment levels, and the tooth remained vital without mobility.

• The radiographic examination showed defect fill when compared to preoperative images
• In the case presented here, the source of implanted osteogenic cells was a commercially available cellular allograft.
• The cellular allograft material consists of cell-rich cancellous bone combined with demineralized cortical bone from the same donor.
• The potential benefits of this material are the ability to provide large amounts of autograft-like concentrations of cells, without the risks of harvest-site morbidity, or patient variability associated with either autograft harvest bone or BMA.
DISCUSSION

• Keys to successful management of this case:
1.Thorough debridement of root surface
2.Primary closure
3.Patient compliance





























