Embed Size (px)
Citation preview

Kristina Cesa, MPH
ORISE fellow, Division of HIV/AIDS Prevention
Office of the Director
CDC’s Expanded HIV Testing Program: Successes, Best Practices and Lessons
Learned
1
National HIV Prevention Conference
Atlanta, GA
August 14-17th, 2011
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
Division of HIV/AIDS Prevention

Advancing HIV Prevention: New Strategies for a Changing Epidemic, 2003
� Strategy 1
• Make HIV testing a routine part of medical care
� Strategy 2
• Implement new models for diagnosing HIV infections outside medical settings
� Strategy 3
2
� Strategy 3
• Prevent new infections by working with persons diagnosed with HIV and their partners
� Strategy 4
• Further decrease perinatal HIV transmission
MMWR 2003;52:329-32

Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in
Health-Care Settings
� HIV screening in all health-care settings for adults ages 13-64 years
• Opt-out testing strategy
� Persons at high risk for HIV infection should be screened annually
3
annually
� General consent for medical care should encompass consent for HIV testing
� Prevention counseling should not be required with HIV diagnostic testing or as part of HIV screening programs in health-care settings
� HIV screening should be included in the routine panel of prenatal screening tests for all pregnant women
MMWR 2006;55 (No.RR-14)

PS07-768: Expanded and Integrated Human
Immunodeficiency Virus (HIV) Testing for Populations
Disproportionately Affected by HIV, Primarily African
Americans
� Purpose:
1. Increase testing opportunities for populations disproportionately affected by HIV, primarily African Americans
4
affected by HIV, primarily African Americans
2. Increase the proportion of HIV-infected persons in these populations who are aware of their infection and are linked to medical care

PS07-768: Expanded HIV Testing Program
� Annual Goals:
1. Test 1.5 million persons
2. Identify 20,000 previously undiagnosed HIV infections
� Project length: 3 years (Oct 2007 – Sept 2010)
5
� Total Funding: $111,211,614
� Venues: Clinical settings (at least 80%)Non-clinical settings (no more than 20%)

MA
NYC
NJ
ChicagoWA
OR
ID
MT
WY
ND
SD
MN
WINY
ME
MI
NH
VT
PA
RI
CT
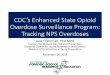
PS07-768: Funded Jurisdictions¹
Eligibility: At least 140 AIDS cases (estimated) among African Americans in 2005
6
Washington, D.C.
1Represents 95% of AIDS cases among African Americans in the United States in 2005
Los Angeles County CA
NV
WY
UT
AZNM
CO
NE
KS
OK
TX
IA
MO
AR
LA
MS AL GA
FL
ILIN
KY
TNSC
NC
VAWV
PADE
MD
Houston
CT
OH
Funded in Years 1-3
Funded in Years 2-3
Philadelphia.

Number of HIV Tests, Positive Tests, and Positive Test Rates
October 2007 – September 2010
Total Clinical Settings Non-Clinical Settings
Tests Done 2,786,739 2,519,917 (90%) 266,822 (10%)
7
Confirmed HIV+ 29,503 23,546 (80%) 5,957 (20%)
New HIV+ 18,432 15,478 (84%) 2,954 (16%)
Previous HIV+ 11,071 8,068 (73%) 3,003 (27%)
New HIV+ Rate 0.7 0.6 1.1
Data Source: APR Year 1–3

Number of HIV Tests, New Positive Tests and New Positive Rate in Years 1 – 3
Year 1 Year 2 Year 3
HIV Tests 458,014 1,021,181 1,307,544
8
New Positive Tests 4,029 6,821 7,582
New Positive Rate 0.9% 0.7% 0.6%
Data Source: APR Year 1–3

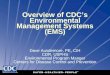
Proportion of HIV Tests and New HIV Positives by Race/Ethnicity
October 2007 – September 2010
60%
70%
60%
80% HIV TestsNew HIV PositivesNew Positive Rate, %
9
18% 16%
5%
14% 12%
5%
0%
20%
40%
Black/AA White Hispanic Other/Unknown*
Race/Ethnicity
Perc
en
t
0.8 0.5 0.5
* Includes American Indian/ Alaskan Native, Asian, Native Hawaiian/ Pacific Islanders, multiple race and unknown

Proportion of HIV Tests and New HIV Positives by Gender
October 2007 – September 2010
55%
45%
72%
60%
80%
HIV TestsNew HIV PositivesNew Positive Rate, %
10
45%
<1%
27%
1%0%
20%
40%
Male Female Other*
Perc
en
t
Gender
New Positive Rate, %
0.9 0.4
* Includes transgender and unknown categories

Venues Funded Under PS07-768Year 3 (October 2009 – September 2010)*
20%
30%
281
183
270
315
11
* (n=1,331)
0%
10%
Emergency Departments
STD Clinics Correctional Health
Facilities
Substance Abuse
Treatment Centers
Community Health
Centers
Community Based
Organizations
Other**
108
7698
** Includes Inpatient Medical Units, Urgent Care Clinics, Substance Abuse Treatment Centers, TB Clinics, and miscellaneous

Distribution of HIV Tests and New Positive Testsby Venue Type
October 2007 – September 2010*
30%
20%
32%
30%
40%HIV TestsHIV PositivesNew Positive Rate, %
12
* (n=2,562,124)
20%
17%15%
6%
11%
20%
12%14%
11% 11%
0%
10%
20%
Emergency Departments
STD Clinics Community Health Centers
Correctional Health Facilities
Community Based Organizations
Other **
0.7 0.6 0.5 0.6 0.6
** Includes Inpatient Medical Units, Urgent Care Clinics, Substance Abuse Treatment Centers, TB Clinics, and miscellaneous
1.2

New HIV-Positives by Selected OutcomeOctober 2007 – September 2010
Total Clinical Settings
Non-Clinical Settings
New HIV-Positives 18,432 15,478 2,954
13
New HIV+ Receiving Test Results
91% 93% 84%
New HIV+ Linked to Medical Care
75% 78% 63%
New HIV+ Referred to Partner Services
83% 83% 82%
Data Source: APR Year 1–3

CDC Cost per Test and New HIV DiagnosisOctober 2007 – September 2010
Year 1 Year 2 Year 3
Tests 458,014 1,021,181 1,307,544
Cost/Test $58 $36 $30
14
Data Source: APR and grantee financial status reports year 1 – 3
New Positives 4,029 6,821 7,582
Cost/New Positive
$6,634 $5,346 $5,163

PS07-768: Barriers & Challenges
� Start-up delays
� New partnerships
� Provider resistance
� Laws and policies
Operational issues
15
� Operational issues
� Technical assistance/training
� Data management
� Reimbursement

PS07-768: Lessons Learned
� Testing Strategy: Opt-out vs. Opt-in
� Difficult to identify a profile to capture all those at risk/unaware of infection
� Opt-out screening reaches clients who otherwise would not have been tested
16
tested
� Opt-out HIV screening in high prevalence areas maximizes case finding value

PS07-768: Lessons Learned
� Test Technology: Rapid vs. Conventional
� Rapid Testing Models:
• Increase receipt of preliminary results
• Decrease the number of clients lost to follow up
• More feasible in settings with dedicated testing staff
17
� Conventional Testing:
• Reduces disruptions to clinic flow associated with point-of-care testing
• Feasible in clinical settings where routine blood tests are ordered as a standard of care
• Reduces the overall costs of testing
• Using multi-platform analyzers increases the volume of tests and decreases the turn around time for results

PS07-768: Lessons Learned
� Staffing Model: Integrated vs. Parallel
� Parallel Models:
• Minimum effect on the clinic flow
• Better acceptance from staff
• More expensive and require additional space
18
� Integrated Models:
• More difficult to initiate due to:
o Perceived burden on clinic flow
o Extensive training requirements
• Requires getting buy-in from staff
• More cost effective and increase sustainability

PS07-768: Lessons Learned
� Sustainability
� Identifying and maximizing all possible sources of funding
� Building community support and cultivating program champions
� Implementing innovative strategies
• Cost effective staffing models
• Low cost testing models
19
• Low cost testing models
� Develop a “business case” for routine testing

PS 07-768: Lessons Learned
� Bottom Line:
Routine HIV screening in healthcare settings
20
Routine HIV screening in healthcare settings WORKS!

PS10-10138/ PS12-1201: Expanded HIV Testing for Disproportionately Affected Populations
� Purpose:
� To sustain progress made under announcement PS07-768
� To expand routine testing services to new clinical venues to reach a broader array of at-risk populations.
� Target Population:
21
� Target Population:
� African American and Hispanic men and women
� MSM and IDUs, regardless of race or ethnicity
� Grantees: � Expanded to 30 state, territorial and local health departments
under PS10-10138
� Eligibility further extended to 36 jurisdictions under PS12-1201

PS10-10138/ PS12-1201: Expanded HIV Testing for Disproportionately Affected Populations
� Objectives: (when fully implemented)
1. Conduct ≥ 1.3 million tests
2. Identify ≥ 6,500 undiagnosed HIV infections
3. Receipt of test results (≥ 85% of positives)
4. Linkage to medical care (≥ 80% of positives)
22
4. Linkage to medical care (≥ 80% of positives)
5. Linkage to partner services (≥ 80% of positives)
6. Receipt of prevention counseling and/or referral to prevention services (≥ 80% of positives)
7. Sustainability
8. Service Integration

Acknowledgments:
Co-authors:
� Christopher Brown
� Sam Dooley
� Erica Dunbar
Benny Ferro
Additional Acknowledgments:
Nadia Duffy
Abigail Viall
PS 07-768 Grantees
23
� Benny Ferro
� Priya Jakhmola
� Marlene McNeese-Ward
� Kimberly Thomas
� Cathy Yanda

Kristina Cesa404-639-6418
24
For more information please contact Centers for Disease Control and Prevention
1600 Clifton Road NE, Atlanta, GA 30333Telephone, 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348E-mail: [email protected] Web: www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
National Center for HIV/AIDS, Viral Hepatitis, STD & TB Prevention