Embed Size (px)
Citation preview
Jeffrey Turner SPT, CSCS
Junsik Yoon SPT
5th most common condition
~25% adults report LBP w/in past 3 months
Prevalence of 70% over the course of one’s life
>85% cannot be reliably attributed to a specific disease or abnormality
Classified into 3 broad categories:
1. Nonspecific LBP
2. Nerve Root Syndrome (CES, etc.)
3. Serious Spinal Pathology
Images Courtesy of www.ericcressey.com
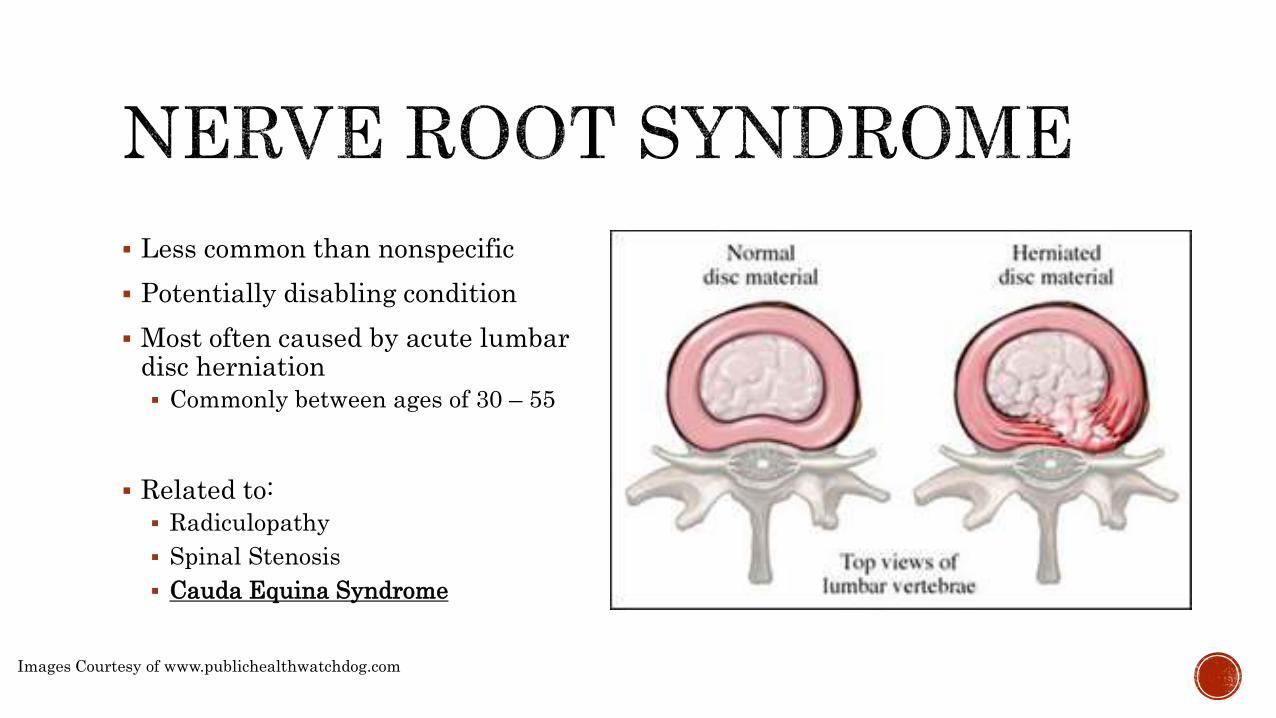
Less common than nonspecific
Potentially disabling condition
Most often caused by acute lumbar disc herniation
Commonly between ages of 30 – 55
Related to:
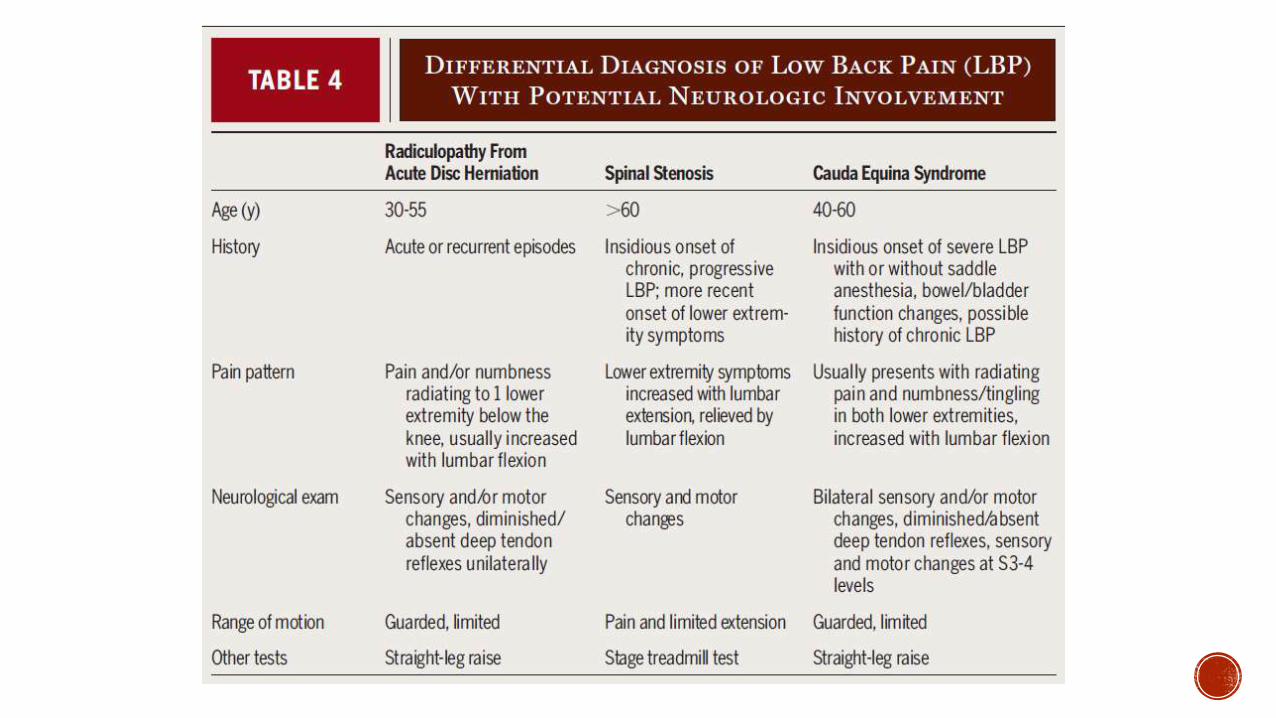
Radiculopathy
Spinal Stenosis
Cauda Equina Syndrome
Images Courtesy of www.publichealthwatchdog.com
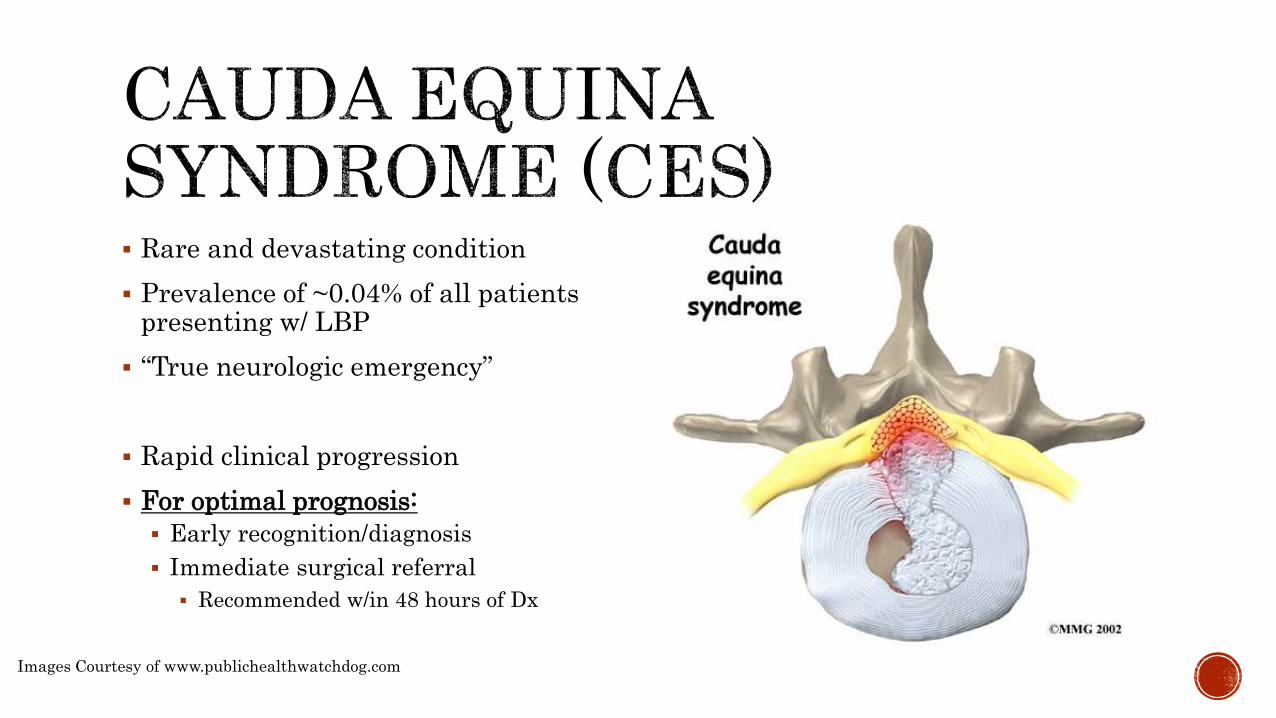
Rare and devastating condition
Prevalence of ~0.04% of all patients presenting w/ LBP
“True neurologic emergency”
Rapid clinical progression
For optimal prognosis:
Early recognition/diagnosis
Immediate surgical referral
Recommended w/in 48 hours of Dx
Images Courtesy of www.publichealthwatchdog.com

32 year old male presented to a PT at a medical aid station in Iraq.
Convoy machine gunner
Prolonged periods of standing >8 hrs
Wearing equipment up to ~80 lbs
4 week history of insidious onset and recent worsening of:
Low back pain
Left buttock pain
Posterior left thigh pain
Goal: Decrease pain during work
Images Courtesy of www.defense.gov
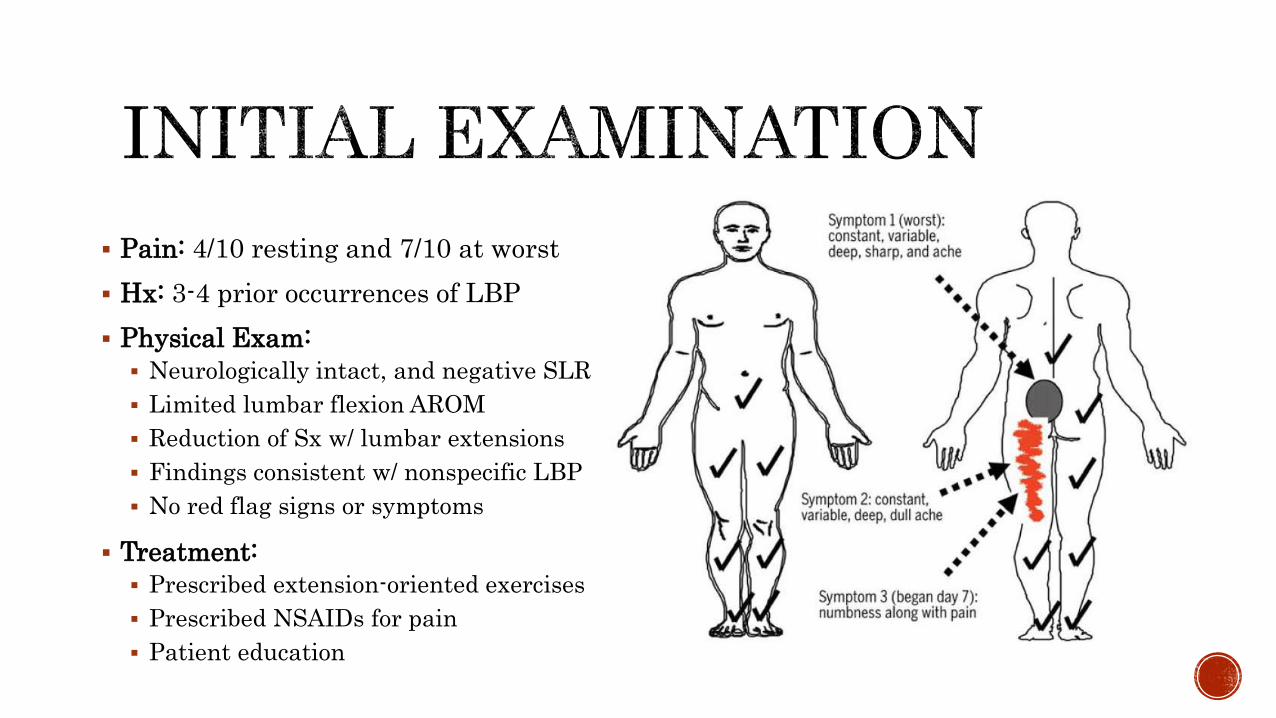
Pain: 4/10 resting and 7/10 at worst
Hx: 3-4 prior occurrences of LBP
Physical Exam:
Neurologically intact, and negative SLR
Limited lumbar flexion AROM
Reduction of Sx w/ lumbar extensions
Findings consistent w/ nonspecific LBP
No red flag signs or symptoms
Treatment:
Prescribed extension-oriented exercises
Prescribed NSAIDs for pain
Patient education
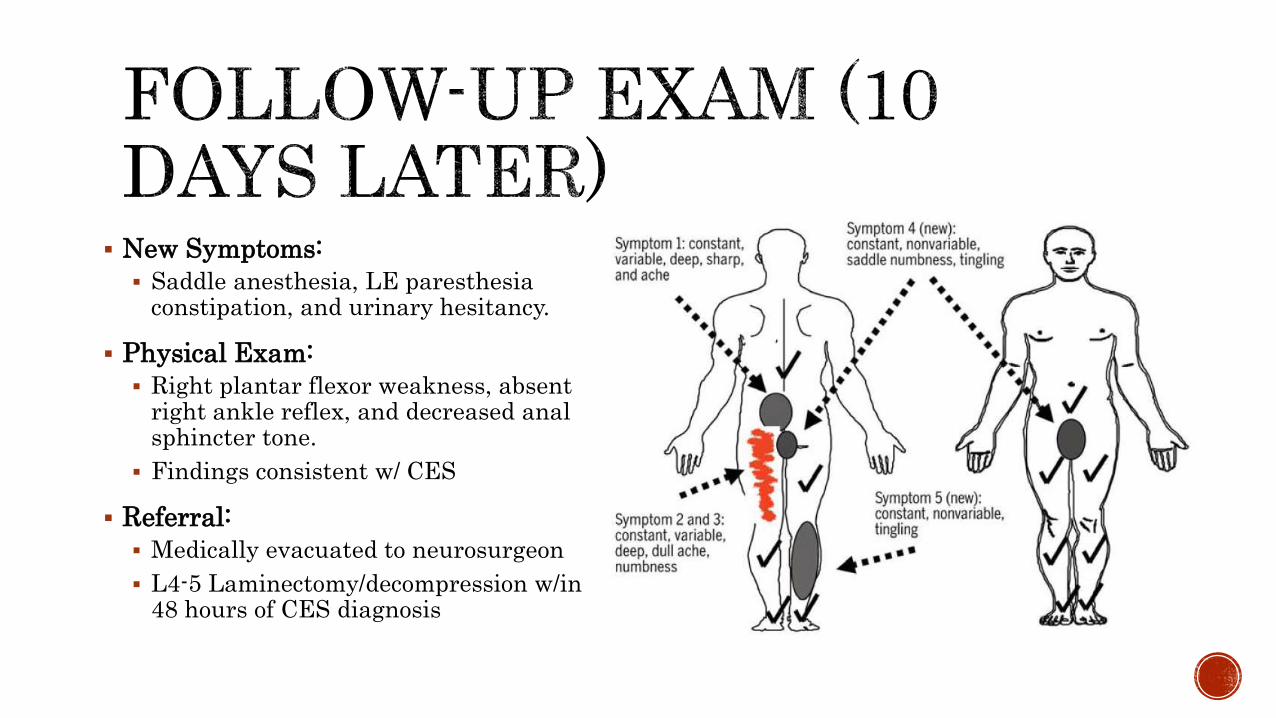
New Symptoms:
Saddle anesthesia, LE paresthesia constipation, and urinary hesitancy.
Physical Exam:
Right plantar flexor weakness, absent right ankle reflex, and decreased anal sphincter tone.
Findings consistent w/ CES
Referral:
Medically evacuated to neurosurgeon
L4-5 Laminectomy/decompression w/in 48 hours of CES diagnosis

Returned to full military duty 18 weeks after surgery without back or lower extremity symptoms or neurological deficits.
Demonstrates the importance of medical screening.
Demonstrates the importance of immediate referral to surgical specialties when CES is suspected.
Rapid intervention offers the best prognosis.
Images Courtesy of www.englishrussia.com
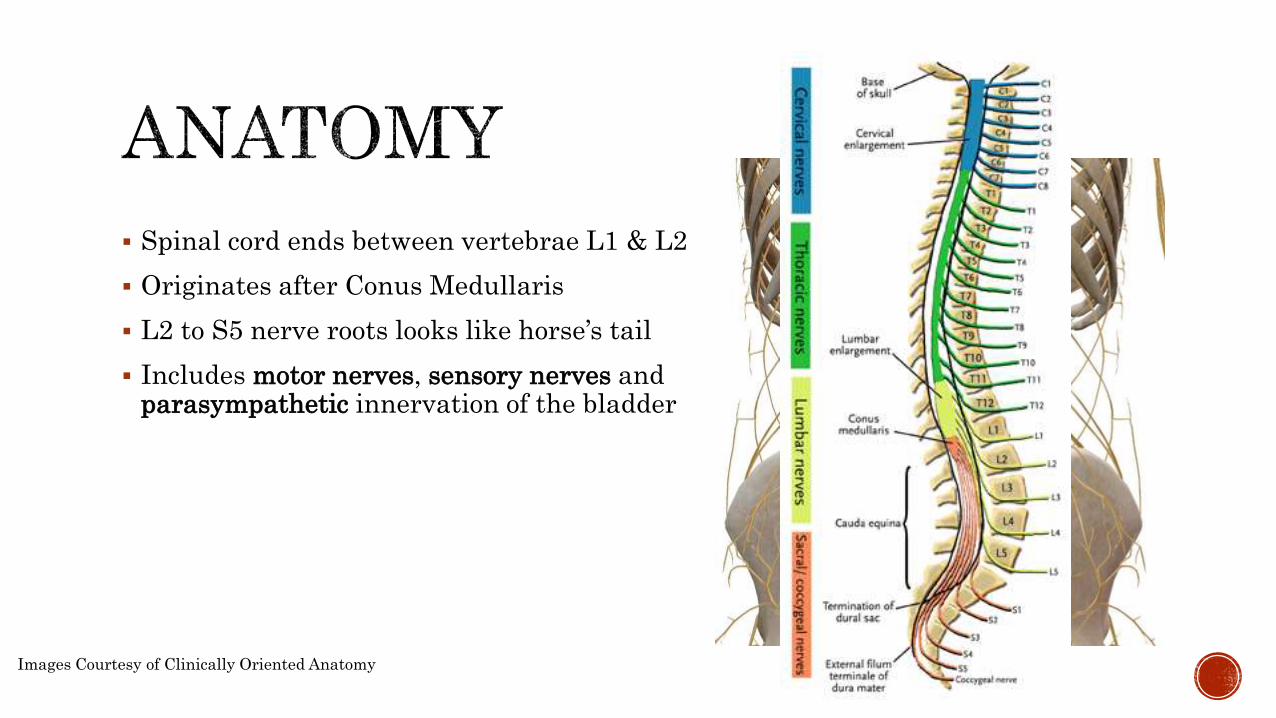
Spinal cord ends between vertebrae L1 & L2
Originates after Conus Medullaris
L2 to S5 nerve roots looks like horse’s tail
Includes motor nerves, sensory nerves and parasympathetic innervation of the bladder
Images Courtesy of Clinically Oriented Anatomy
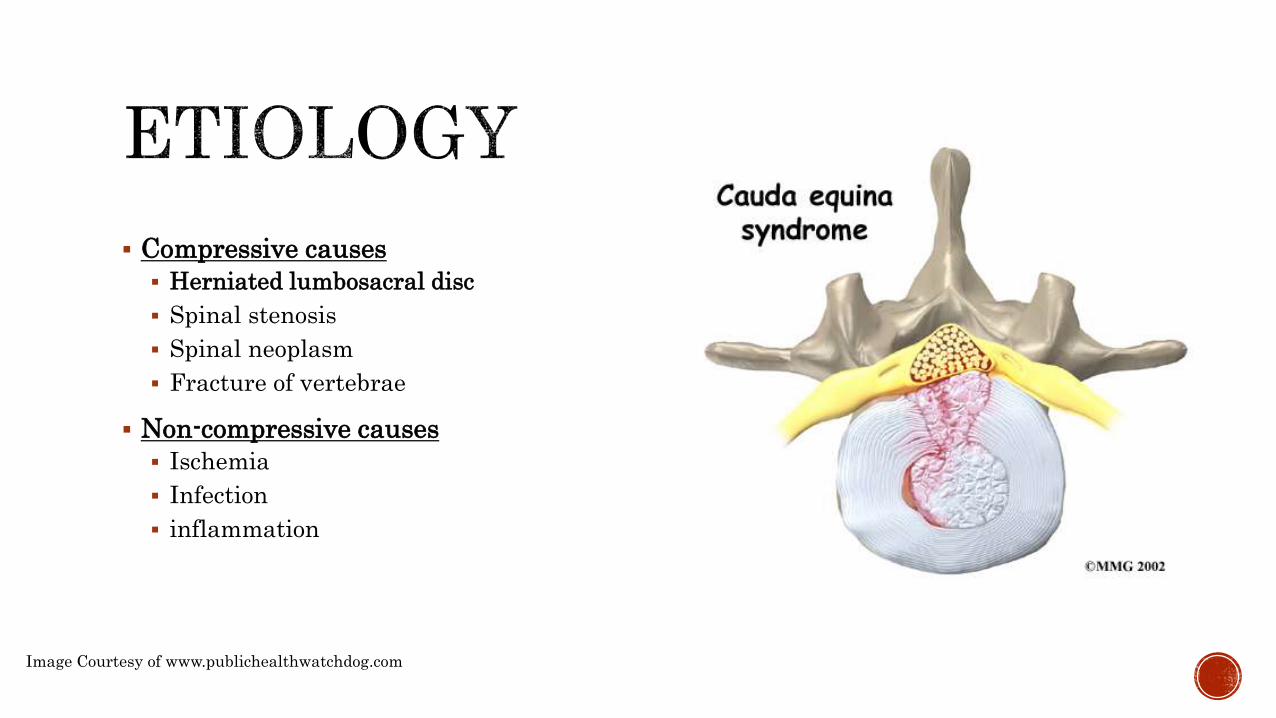
Compressive causes
Herniated lumbosacral disc
Spinal stenosis
Spinal neoplasm
Fracture of vertebrae
Non-compressive causes
Ischemia
Infection
inflammation
Image Courtesy of www.publichealthwatchdog.com
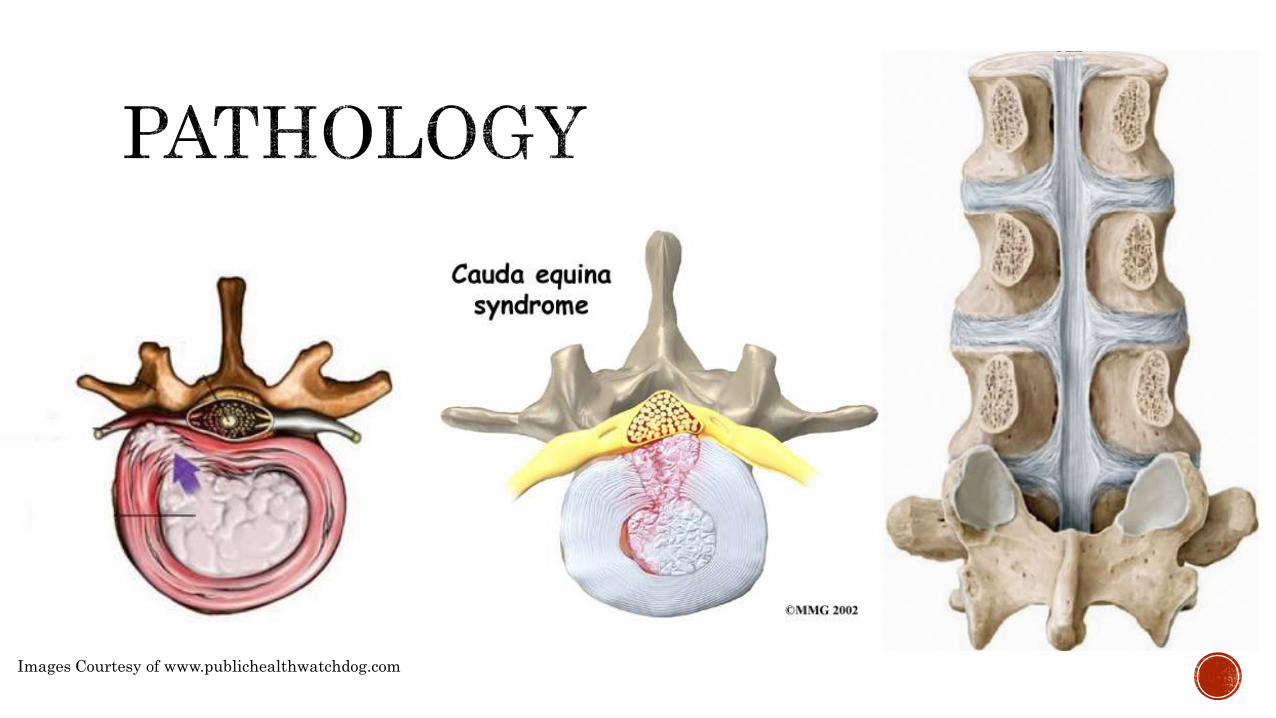
Images Courtesy of www.publichealthwatchdog.com
Making a thorough evaluation
Continually monitoring patient’s status throughout the patient management
Acting appropriately when conditions emerge that requires immediate referral
Image Courtesy of www.bu.edu

Crowell MS, Gill NW. Medical Screening and Evacuation: Cauda Equina Syndrome in a Combat Zone. J Orthop Sports Phys Ther. 2009; 39(7):541-549.
Moore KL, Dalley AF, Agur AMR, et al. Clinically Oriented Anatomy 7th Edition. Lippincott Williams & Wilkins; 2013.