Embed Size (px)
DESCRIPTION
Citation preview

CASE DISCUSSIONS IN POLYPOSIS.
D O U G L A S R I E G E RT J O H N S O N
M AYO C L I N I C F LO R I D A


CASE1
A 45 year-old man presented for medical genetics evaluation. Between the ages of 20 and 30 years, the patient had nasal polyps and several large stalked colon polyps removed. At 43 years-old, he was diagnosed with jejunal adenocarcinoma (T1N0). Upper endoscopy following surgery showed several stomach and small bowel polyps. A genetic test for familial adenomatosis polyposis (APC gene) was negative. There was no family history of cancer.
What is the diagnosis?


NASAL POLYPOSIS
Originally published in Dutch as: Peutz J. Very remarkable case of familial polyposis of mucous membrane of intestinal tract and nasopharynx accompanied by peculiar pigmentations of skin and mucous membrane. Nederl Maandschr Geneesk. 1921; 10:134-146.

RRIR
Smooth muscle arborizing through PJS polyp

CASE2
4 years old. Alive and well.
28 years oldAlive and well
48 years oldThyroid disease
50 years oldAlive and well
25 yo dx with transverse CRC, 25 tubular adenomas in left colon (right colon not seen due to obstruction).A few stomach polyps. At 22 yo dx left temporal lobe glioblastoma.“Freckles in Eye”.


CASE2
4 years old. Alive and well.
28 years oldAlive and well
48 years oldThyroid disease
50 years oldAlive and well
25 yo dx with transverse CRC, 25 tubular adenomas in left colon (right colon not seen due to obstruction)A few stomach polyps. At 22 yo dx left temporal lobe glioblastoma.“Freckles in Eye”.DX: ? FAP NEW MUTATION TURCOT

TERM “TURCOT SYNDROME” AS CURRENTLY USED
FAP + brain tumor (usually meduloblastoma) = Turcot syndrome
LS + brain tumor (usually glioblastoma) = Turcot syndrome

TURCOT SYNDROME
Described in 1959 by Jacques Turcot in Diseases of the Colon and Rectum
Hôtel Dieu de Quebec hospital (1640) and the Laval University
2 teenage siblings with numerous colorectal polyps. The brother (15 years old) with meduloblastoma of the spinal cord and adenocarcinomas of the sigmoid colon and rectum. The sister (13 years old) with cerebral glioblastoma and pituitary adenoma.
Mckusick and Osler communicated that parents were third cousins.
Crail Syndrome case report (1949) Adenomatous polyposis, mebullastoma of the brain stem,
and papillary thyroid cancer.
New England Journal Medicine article describing molecular phenotype.Turcot original report 1959. 13839882.

CASE2
4 years old. Alive and well.
28 years oldAlive and well
48 years oldThyroid disease
50 years oldAlive and well
25 yo dx with transverse CRC, 25 tubular adenomas in left colon (right colon not seen due to obstruction)A few stomach polyps. At 22 yo dx left temporal lobe glioblastoma.“Freckles in Eye”.
Test Diagnosis Result
APC
MUTYH
MLH1/MSH2
Mismatch repair gene IHC
DNA Microsatellite Instability
DX: ? FAP NEW MUTATION TURCOT

CASE2
4 years old. Alive and well.
28 years oldAlive and well
48 years oldThyroid disease
50 years oldAlive and well
25 yo dx with transverse CRC, 25 tubular adenomas in left colon (right colon not seen due to obstruction)A few stomach polyps. At 22 yo dx left temporal lobe glioblastoma.“Freckles in Eye”.
Test Diagnosis Result
APC FAP
MUTYH MAP
MLH1/MSH2 Lynch syndrome 2 genes
Mismatch repair gene IHC Lynch syndrome 5 genes
DNA Microsatellite Instability
Lynch syndrome 5 genes
DX: ? FAP NEW MUTATION TURCOT

CASE2
4 years old. Alive and well.
28 years oldAlive and well
48 years oldThyroid disease
50 years oldAlive and well
25 yo dx with transverse CRC, 25 tubular adenomas in left colon (right colon not seen due to obstruction)A few stomach polyps. At 22 yo dx left temporal lobe glioblastoma.“Freckles in Eye”.
Test Diagnosis Result
APC FAP Normal
MUTYH MAP Normal
MLH1/MSH2 Lynch syndrome 2 genes
Normal
Mismatch repair gene IHC
Lynch syndrome 5 genes
Abnormal
DNA Microsatellite Instability
Lynch syndrome 5 genes
Not done : Probably normal
DX: ? FAP NEW MUTATION TURCOT

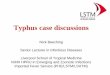
Normal Staining of PMS2 in tumor.Both copies of PMS2 present.
Lynch syndrome. No staining in tumor. (Both copies of PMS2 inactivated, one inherited, one acquired in tumor) Staining
in tumor lymphocytes and normal tissue.
Patient Results: Constitutional mismatch repair deficiency. No staining in tumor and normal tissue.
(Both copies of PMS2 inactivated in tumor and normal by inherited mutations.)

CONSTITUTIONAL MISMATCH REPAIR DEFICIENCYFirst described in 1999 in two simultaneously published
reports (Ricciardone et al. 1999; Wang et al. 1999)
Synonyms.Childhood cancer syndrome (CCS) Lynch III syndrome ‘‘CoLoN’’, Colon tumours or/and Leukaemia/Lymphoma
Constitutional mismatch repair-deficiency syndrome:have we so far seen only the tip of an iceberg?

MICRO SATELLITE INSTABILITY UNRELIABLE IN CMMRDDNA measurements of microsatellite instability
based on comparing normal and tumor tissue MS. In LS, the tumor MS change, so a difference can be seen. (I think) in CMMRD normal and tumor both change so no difference can be seen.
Only one out of the 14 brain tumours exhibited an MSI-high genotype.
Genetic and clinical determinants of constitutional mismatch repair deficiency syndrome: Report from the constitutional mismatch repair deficiency consortium. 24440087.

CMMR OVERLAPS WITH NF1: CASE 2 WITH 50 CALM.
All CMMRD patients with available clinical data (n = 18) had café-au-lait spots (>6 spots) and three patients had hypopigmentation. Three individuals had axillary freckles, and one had a plexiform neurofibroma; meeting the criteria for NF-1, but lacked germline NF-1 mutations.
Genetic and clinical determinants of constitutional mismatch repair deficiency syndrome: Report from the constitutional mismatch repair deficiency consortium.. 24440087.

TUMOR SPECTRUM OF CMMRD IN 92 PATIENTS
Cancer Number Median age (range) of diagnosis
Hematological 30 6 (0.4-17)
Brain tumor 44 8 (2-35)
Colorectal cancer
37 16 (8-35)
Small bowel 9 26 (11-42)
2010 CMMRD Review of 92 patients.

DIFFERENCES IN TUMOR SPECTRUM BASED ON GENOTYPE IN CMMRD
PMS2/MSH6>
MLH1/MSH2
n 65 24
Median age of dx 9 years 4 years
Hematological (#1 Non Hodgkins Lymphoma Tcell)
29% 46%
Brain 35% 8%
Lynch syndrome cancer(colon, endometrial)
68% 29%

CMMRD MUTATION SPECTRUM
PMS2 dominates, followed by MSH6 and MLH1.“MSH2 mutations which are most commonly found in
Lynch syndrome are less common to absent in CMMRD, while PMS2 and MSH6 are more commonly observed in the syndrome. A possible explanation for this phenomenon is low penetrance of heterozygous mutations in MSH6 and PMS2 found in CMMRD and the deleterious functional consequence of homozygous mutations. Highly penetrant mutations in MSH2, may be embryonically lethal when homozygous leading to the lower prevalence observed in CMMRD.”

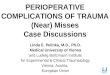
LABORATORY FINDINGS OF CMMRD: IGG CLASS SWITCH
Human PMS2 deficiency is associated with impaired immunoglobulin class switch recombination . 18824584.

Surveillance protocol for patient with for Biallelic MMR mutations.Cancer Surveillance strategy
Children
Colon Colonoscopy annuallya
Upper GI tract and small bowel
EGD annuallya, video capsule endoscopy annuallya
Brainb Ultrasound at birth then MRI brain every 6 months
Leukemiab, Lymphomab Complete blood count, erythrocyte sedimentation rate, lactate dehydrogenase every 4 months
Adults
Colon Colonoscopy annuallya
Upper GI tract and small bowel
EGD annuallya, video capsule endoscopy annuallya
Brainb Ultrasound at birth then MRI brain every 6 months
Leukemiab, Lymphomab Complete blood count, erythrocyte sedimentation rate, lactate dehydrogenase every 4 months
Uterus Ultrasound annually
Upper urinary tract Ultrasound and urine cytology annually
EGD-esophagogastroduodenoscopy. a To start at 3 years of age or at diagnosis;
b Brain, leukemia/lymphoma screening should commence at birth if diagnosed prenatally.
Genetic and clinical determinants of constitutional mismatch repair deficiency syndrome: Report from the constitutional mismatch repair deficiency consortium. 24440087.

EU CMMRD PARIS - JUNE 2013
“In 1968, criteria were proposed by WHO that should be met prior to the implementation of screening programmes. These criteria were used to assess surveillance in CMMR-D. The evaluation showed that surveillance for CRC is the only part of the programme that largely complies with the WHO criteria.”
Guidelines for surveillance of individuals with constitutional mismatch repair-deficiency proposed by the European Consortium "Care for CMMR-D" (C4CMMR-D). J Med Genet. Vasen HF and others behalf of the EU-Consortium Care for CMMR-D (C4CMMR-D).


CASE 2 GENETIC TEST RESULTS
4 years old. Alive and well.
28 years oldAlive and well
48 years oldThyroid disease
50 years oldAlive and well
PMS2 gene mutation (Pro246Cysfsx3)
PMS2 gene mutation (Ile611Asnfsx3)
25 yo dx with
transverse CRC.
PMS2 gene wildtype (normal)
CONSTITUTIONAL MISMATCH REPAIR DEFICIENCY = 1 LS MUTATION FROM FATHER, AND 1 FROM MOTHER, (BIALLELIC)

CASE 2 GENETIC TEST RESULTS
4 years old. Alive and well.
28 years oldAlive and well
48 years oldThyroid disease
50 years oldAlive and well
PMS2 gene mutation (Pro246Cysfsx3)
PMS2 gene mutation (Ile611Asnfsx3)
PMS2 gene wildtype(normal)
25 yo dx with
transverse CRC.
or

ECCLESIASTES 1:9
The thing that hath been, it is that which shall be; and that which is done is that which shall be done: and there is no new thing under the sun.

Described in 1959 by Jacques Turcot in Diseases of the Colon and Rectum
Hôtel Dieu de Quebec hospital (1640) and the Laval University2 teenage siblings with numerous colorectal polyps. The brother (15 years old) with meduloblastoma of the spinal cord and adenocarcinomas of the sigmoid colon and rectum. The sister (13 years old) with cerebral glioblastoma and pituitary adenoma.Mckusick and Osler communicated that parents were third cousins.
“Every case of familial polyposis should be followed and explored, not only looking for new occurrences of polyps in the colon and rectum, when they are not removed by also for the appearance of other tissue tumors elsewhere in the body.”


FEATURES OF TURCOT BY ITOH AND OTHERS (1) In Turcot's syndrome the manifestations of brain tumour and colonic
polyposis are significantly associated and are not merely coincidental, although the association of brain tumour is only incidental in the few cases of familial polyposis coli.
(2) Moreover, an autosomal recessive mode of transmission is most likely in this syndrome.
(3) The number of colonic polyps in Turcot's syndrome was frequently less than 100, in contrast with the study of Bussey (1975) who noted that the average number of polyps in familial polyposis coli was about 1000 and rarely less than 200. The analysis of macroscopic findings of colonic polyps showed that they were fewer in number and larger in size in Turcot's syndrome compared with familial polyposis coli.
(4)Therefore, we present the hypothesis that Turcot's syndrome is genetically distinct from familial polyposis coli.
Turcot syndrome and its characteristic colonic manifestations.Itoh H, Ohsato K. Dis Colon Rectum. 1985 Jun;28(6):399-402.

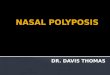
There were several cafr-au-lait spots on the
skin of the chest, back, abdomen, and extremities,
but there were no nodules on the body surface.
H Itoh and others, Gut 1979. Kyushu University Faculty of Medicine, Fukuoka, Japan.“There were several cafe-au-lait spots on theskin of the chest, back, abdomen, and extremities, but there were no nodules on the body surface.”

Proband. 13 yo from Brazil. Youngest in a family of 7 children.
No gastric or extracolonic features
of FAP.

END

SUPPLE
MENTAL
SLIDES

Compared with familial polyposis coli, colonic polyps in Turcot’s syndrome are fewer in number and larger in size.