Embed Size (px)
Citation preview
CLINICAL DIAGNOSIS

FIRST VISIT
• Overall Appraisal of the Patient • Medical History • Dental History • Intraoral Radiographic Survey • Casts • Clinical Photographs • Review of the Initial Examination
SECOND VISIT
• Oral Examination • Examination of the Teeth and Implants • Examination of the Periodontium
A Periodontal Diagnosis should determine :
1. Presence of disease 2. Identify the type 3. Extent 4. Distribution 5. Severity 6. Understanding of cause
Gingival Diseases• Chronic marginal gingivitis • Acute necrotizing ulcerative gingivitis • Acute herpetic gingivostomatitis • Allergic gingivitis • Gingivitis associated with skin diseases • Gingivitis associated with endocrine-metabolic disturbances • Gingivitis associated with hematologic-immunologic
disturbances • Gingival enlargement associated with medications • Gingival tumors
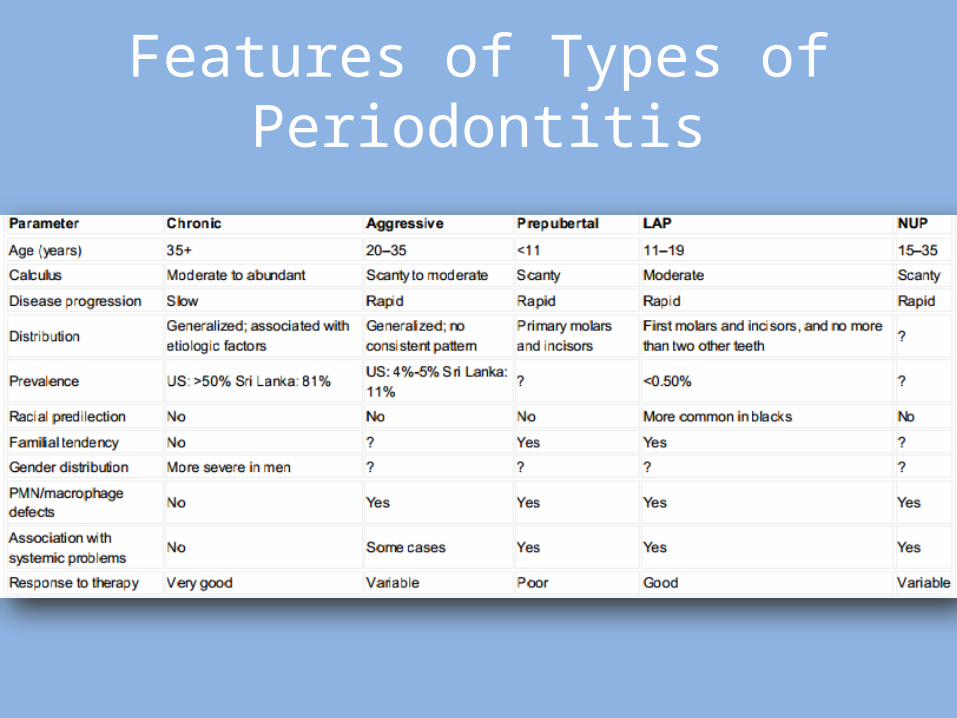
Features of Types of Periodontitis

FIRST VISIT
• Overall Appraisal of the Patient
1. Mental and emotional status2. Temperament3. Attitude4. Physiologic age
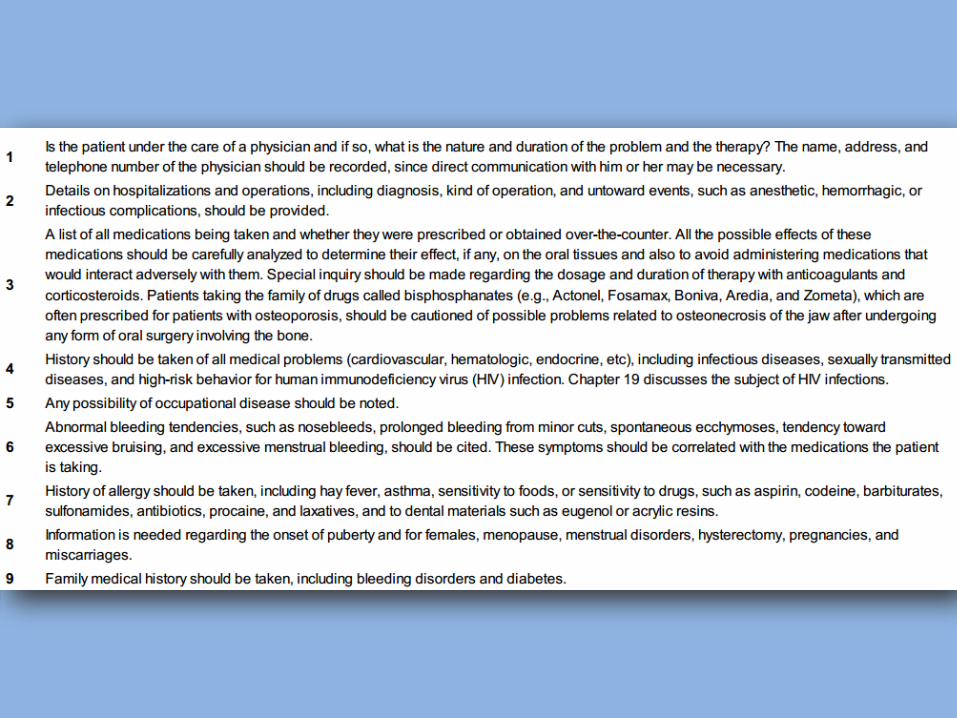
Medical History
• The possible role of some systemic disease, conditions and behavioral factors.
• Presence of condition may require caution.
• The possibility that oral infections may have a powerful influence on the occurrence and severity of a variety of systemic diseases and conditions.
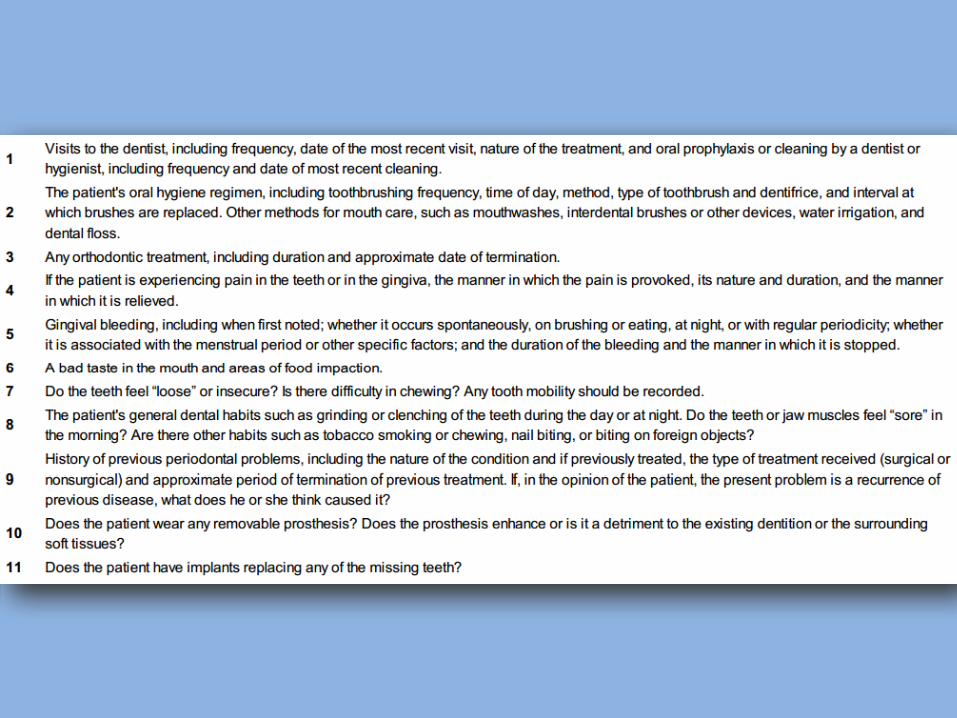
Dental History
• Current illness 1. May be unaware of any problem2. Bleeding gums3. Loose teeth4. Foul taste5. Itchy gums6. Pain (Variable)7. Sensitivity (Hot, Cold, Chewing, Air inhale, Burning)
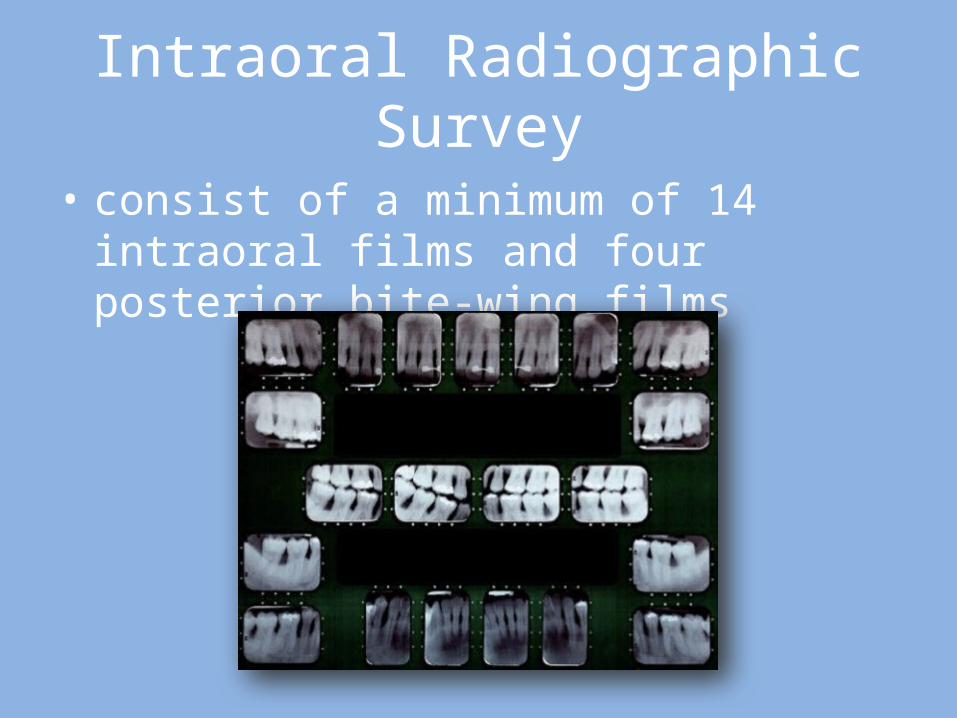
Intraoral Radiographic Survey
• consist of a minimum of 14 intraoral films and four posterior bite-wing films
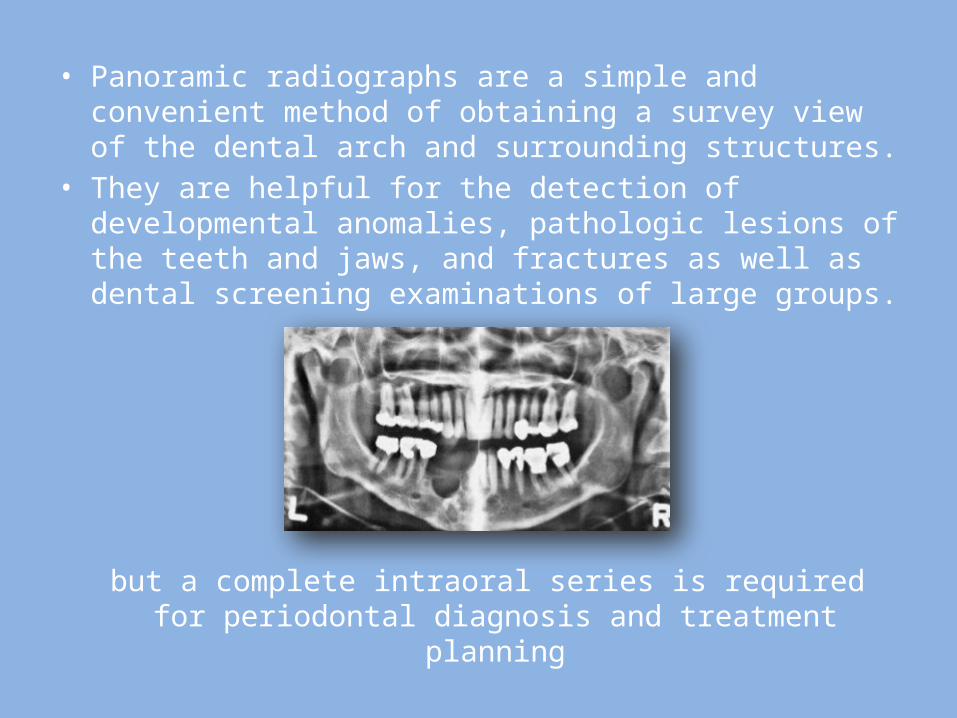
• Panoramic radiographs are a simple and convenient method of obtaining a survey view of the dental arch and surrounding structures.
• They are helpful for the detection of developmental anomalies, pathologic lesions of the teeth and jaws, and fractures as well as dental screening examinations of large groups.
but a complete intraoral series is required for periodontal diagnosis and treatment planning
CASTS
1. Position of gingival margins2. Position and inclination of the teeth3. Proximal contact relationship4. Food impaction areas5. View of lingual-cuspal relationship6. Visual aid in discussion and comparison 7. Position of implant placement (If required)
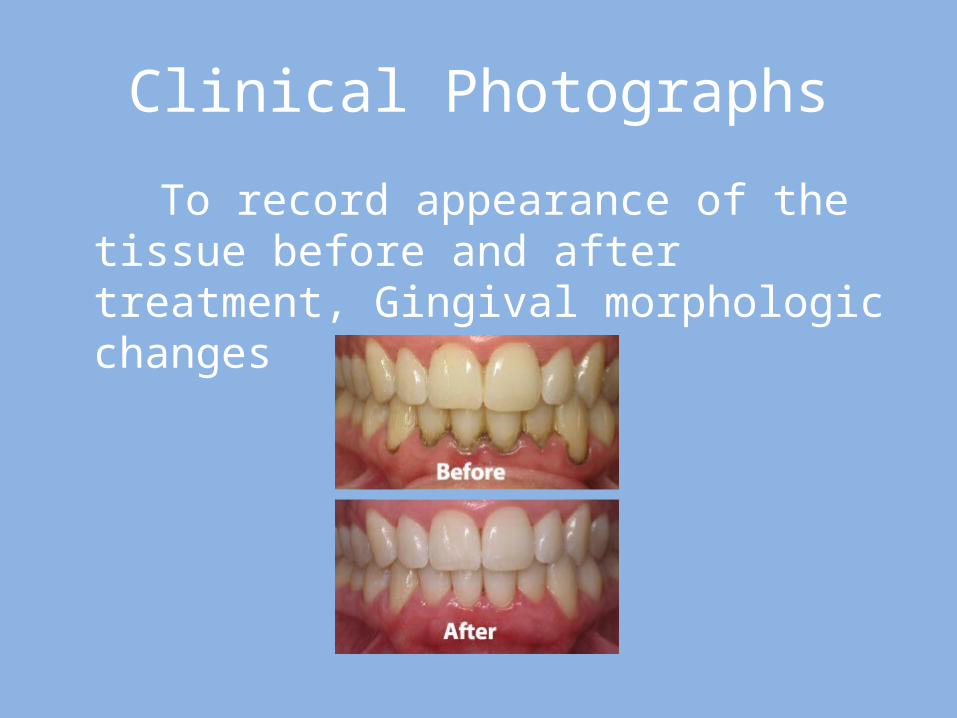
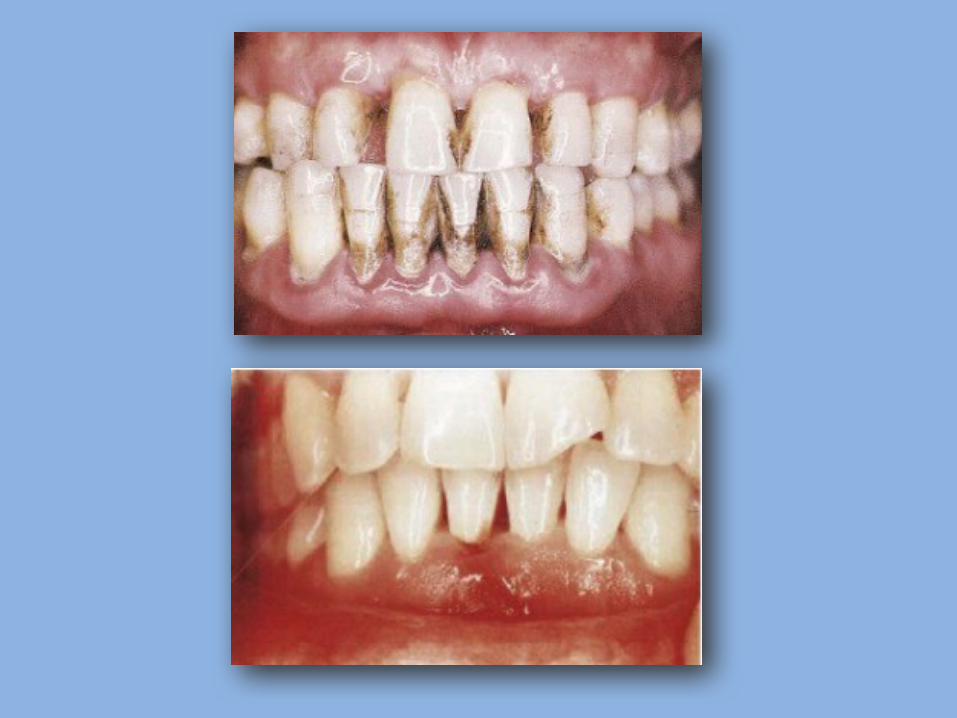
Clinical Photographs
To record appearance of the tissue before and after treatment, Gingival morphologic changes
Review of the Initial Examination
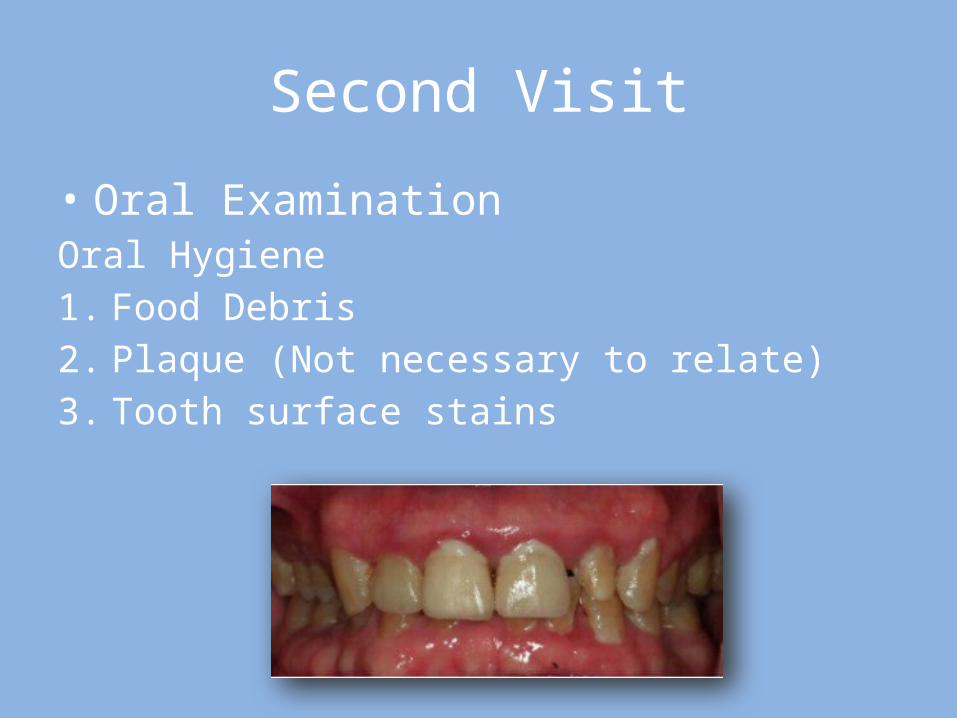
Second Visit
• Oral ExaminationOral Hygiene1. Food Debris2. Plaque (Not necessary to relate)3. Tooth surface stains
• Oral Malodor (Halitosis) May be either oral or extra-oral
• Examination of the Oral Cavity1. Lips2. Floor of the mouth3. Palate4. Tongue5. Oropharyngeal region6. Quality and Quantity of saliva
Examination of Lymph Nodes• Lymph nodes can become enlarged and hard as a result of
infectious episode, malignant metastases and residual fibrotic changes.
• Inflammatory nodes become:1. Enlarged, Palpable, tender and fairly immobile2. Red and warm overlying skin
• Primary herpetic gingivostomatitis, necrotizing ulcerative gingivitis (NUG), and acute periodontal abscesses may produce lymph node enlargement
Examination of the Teeth and Implants
1. Caries2. Poor restorations3. Developmental defects4. Anomalies of the tooth form5. Wasting (Erosion, Attrition, Abrasion)6. Hypersensitivity7. Proximal contact relationship
The stability, position, and number of implants and their relationship to the adjacent natural dentition is also
examined.
• Dental Stains Examined carefully to determine the origin
• Hypersensitivity Root surface exposed by gingival recession
• Proximal Contact Relations Open contact allow food impaction
Tooth Mobility
• Night<Morning (with slight extrusion)• Single rooted>Multi-rooted (incisors having
the most)
Stages of tooth mobility:Initial = 100lb order of 0.05mm to 0.10mm Secondary = 500g 1-2mm(incisors) 0.5-0.9mm(canines)0.08-0.1mm(premolars) 0.4-0.8mm(molars)
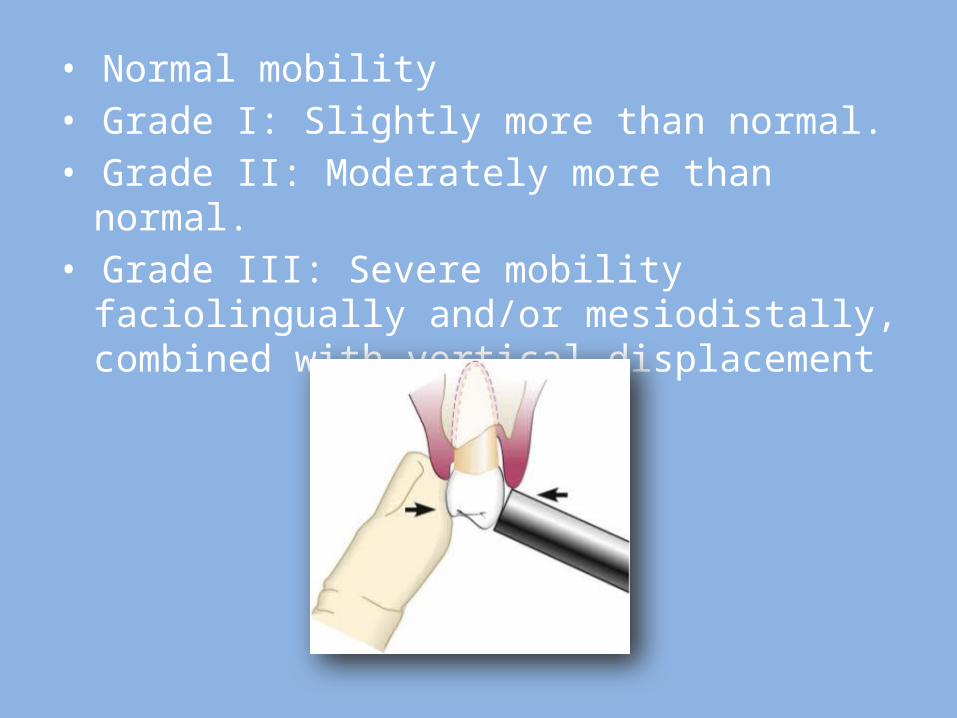
• Normal mobility • Grade I: Slightly more than normal. • Grade II: Moderately more than normal. • Grade III: Severe mobility faciolingually and/or
mesiodistally, combined with vertical displacement
Increased mobility is caused by one or more of the following factors
1. Loss of tooth support(Bone loss)2. Trauma from occlusion3. Extension of inflammation4. Periodontal surgery5. Pregnancy6. Pathologic processes of the jaw(osteomyelitis
and tumors of the jaw(
Trauma from occlusion
1. Excessive tooth mobility2. Widened periodontal space(radiograph)3. Vertical or angular bone destruction4. Infra-bony pockets5. Pathologic migration (especially in anterior
teeth)
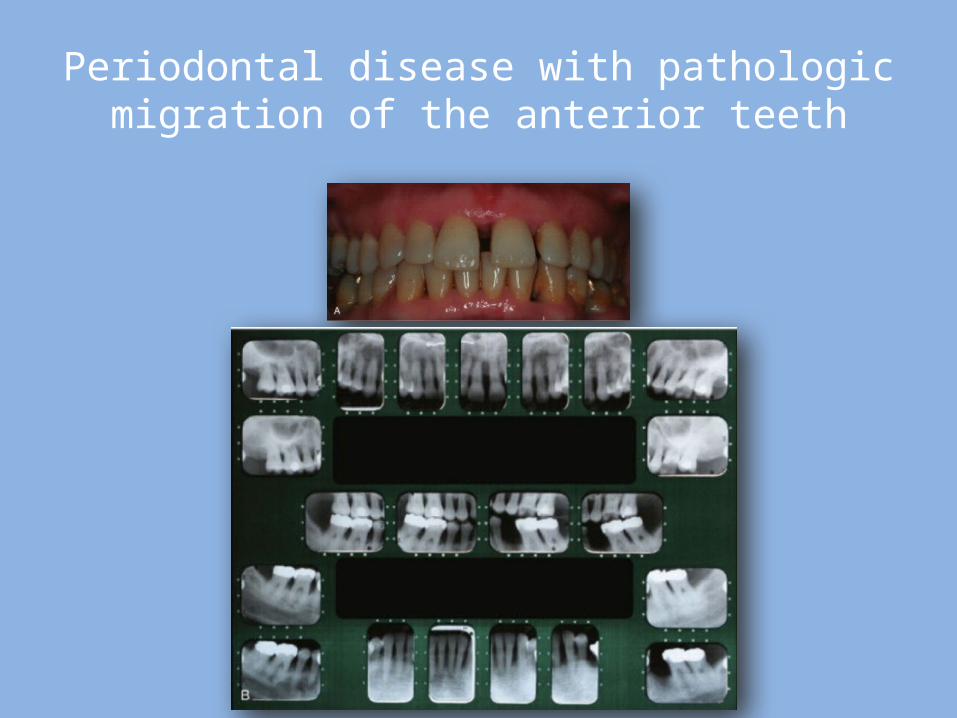
Periodontal disease with pathologic migration of the anterior teeth
• Sensitivity to Percussion Feature of acute inflammation of periodontal
ligament.
• Dentition with the Jaws Closed1. Irregularly aligned teeth2. Extruded teeth3. Improper proximal contacts4. Areas of food impaction
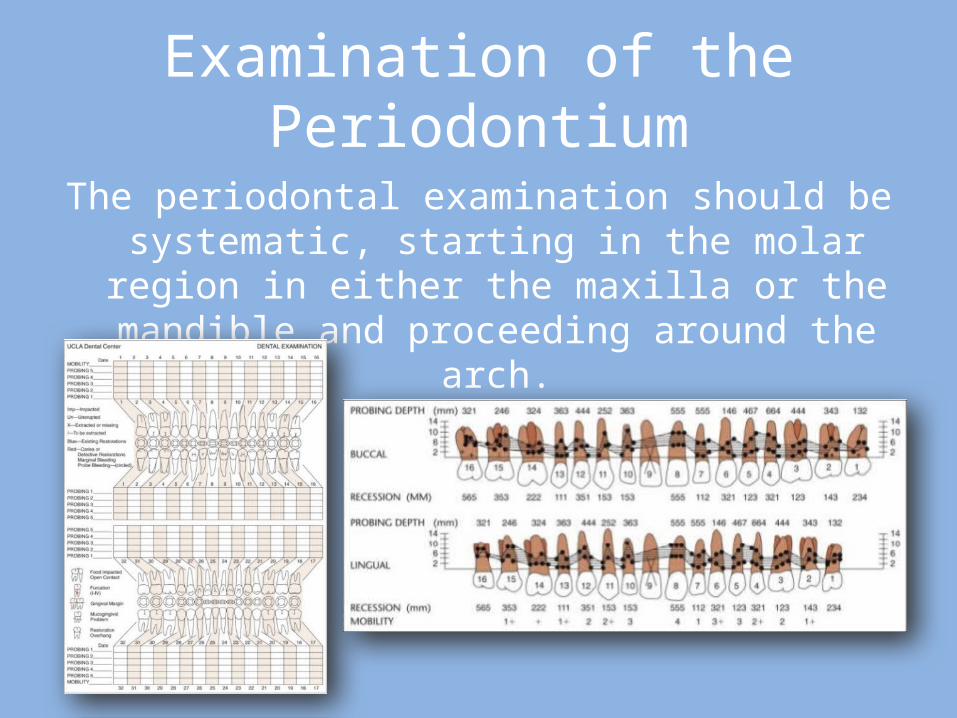
Examination of the Periodontium
The periodontal examination should be systematic, starting in the molar region in either the maxilla or
the mandible and proceeding around the arch.
Plaque and Calculus
• The presence of supragingival plaque and calculus can be directly observed and the amount measured with a calibrated probe.
• For the detection of subgingival calculus, each tooth surface is carefully checked to the level of the gingival attachment with a no. 17 or no. 3A explorer.
Gingiva
• Gingiva must be dried before accurate observation can be made.
1. Observation2. Exploration with instruments3. Firm but gentle Palpation
Features to consider:1. Color2. Size3. Contour4. Consistency 5. Surface texture6. Position7. Ease of bleeding8. Pain
• Clinically gingival inflammation can produce two basic types of tissue response :
1. Edematous (smooth, glossy, red gingiva)
2. Fibrous (firm, stippled, opaque, thicker, round margins)
Periodontal Pockets
• Must include their presence and distribution on each tooth surface
• Pocket depth• Level of attachment on the root• Type of pocket(supra-bony, infra-bony)
Signs and symptoms
• Although probing is the only reliable method of detecting pockets, clinical signs, such as :
1. Color changes(bluish red margin, Bluish red vertical zone)2. “Rolled” edge margins3. Enlarged edematous gingiva4. Bleeding5. Suppuration6. Loose, extruded teeth

1. Generally painless2. But localized pain and sometimes radiating
pain3. Sensation of pressure after eating4. A foul taste in localized areas5. Sensitivity to hot and cold6. Toothache in absence of caries
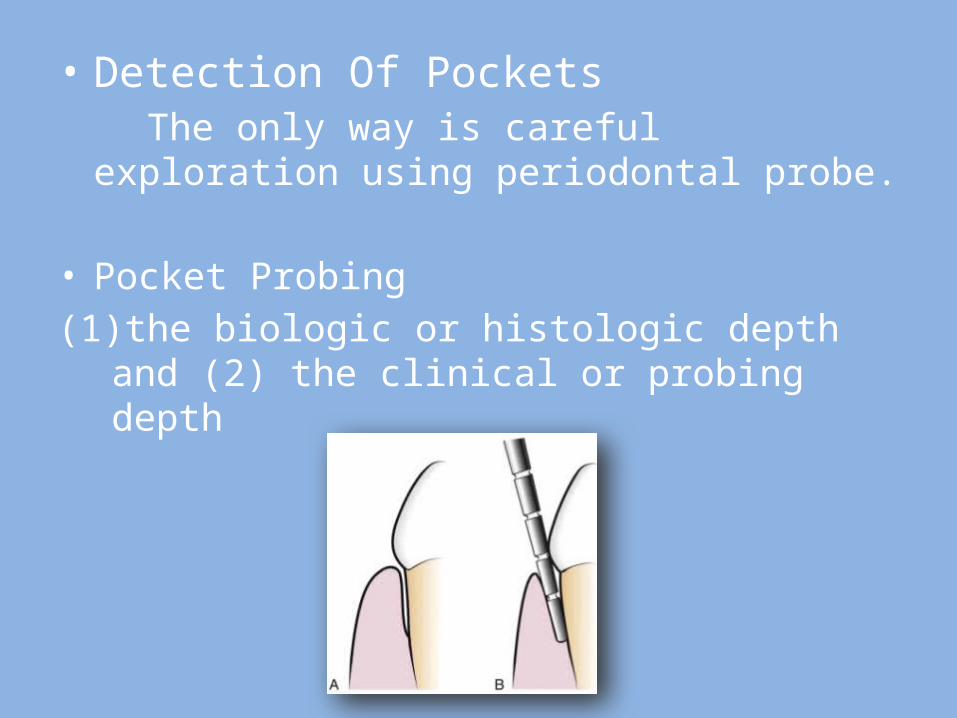
• Detection Of Pockets The only way is careful exploration using periodontal
probe.
• Pocket Probing (1) the biologic or histologic depth and (2) the clinical
or probing depth
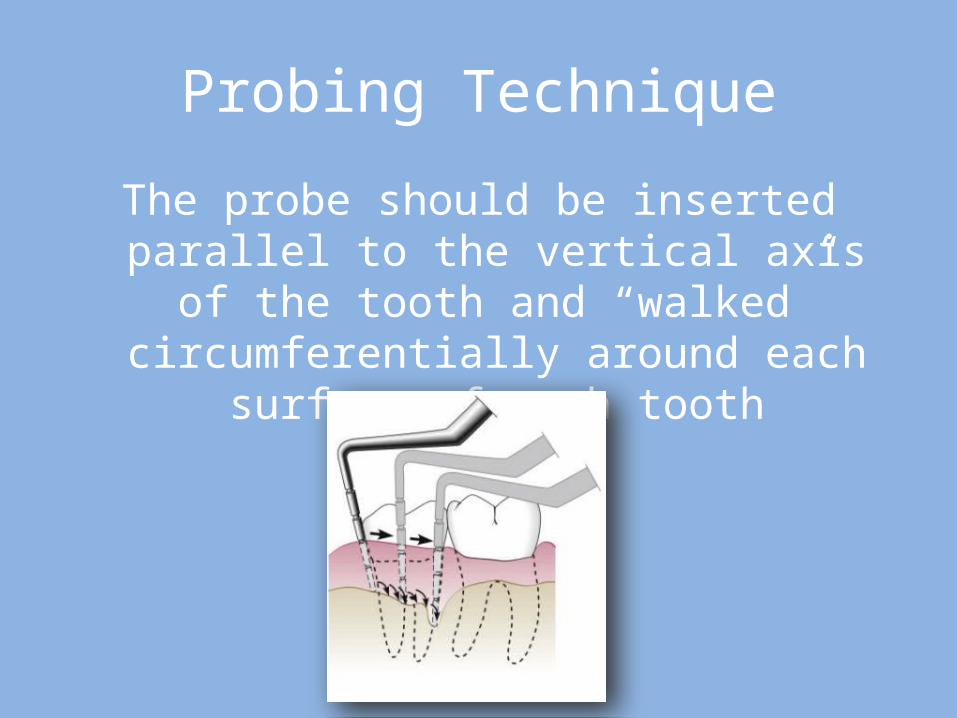
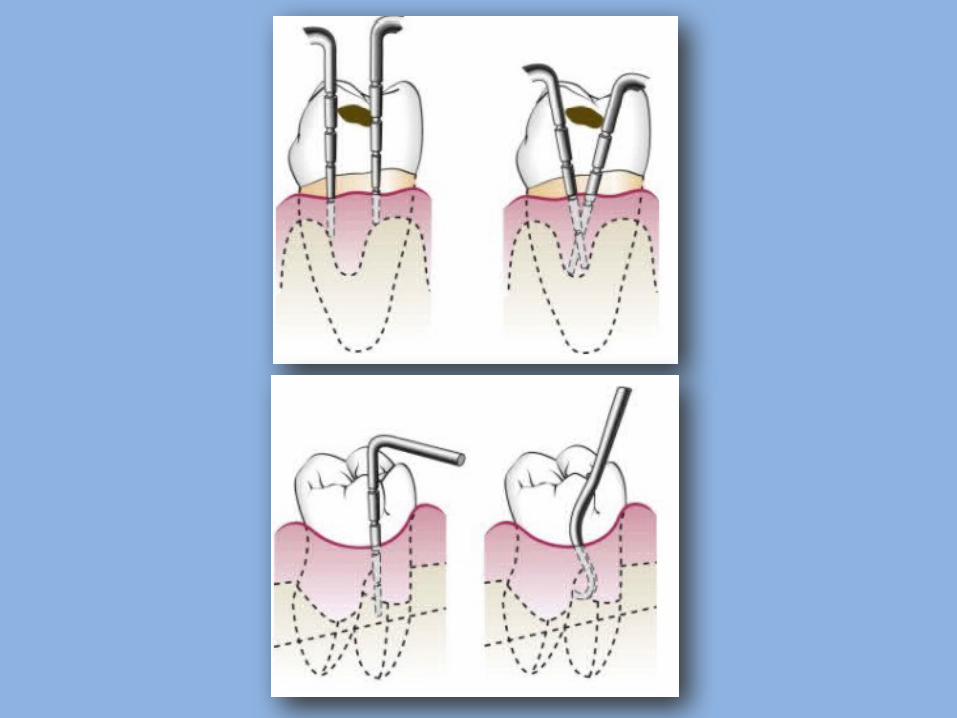
Probing Technique
The probe should be inserted parallel to the vertical axis of the tooth and “walked”
circumferentially around each surface of each tooth
Level of Attachment Versus Pocket Depth
• Pocket depth is the distance between the base of the pocket and the gingival margin
• The level of attachment, on the other hand, is the distance between the base of the pocket and a fixed point on the crown such as the cementoenamel junction (CEJ)
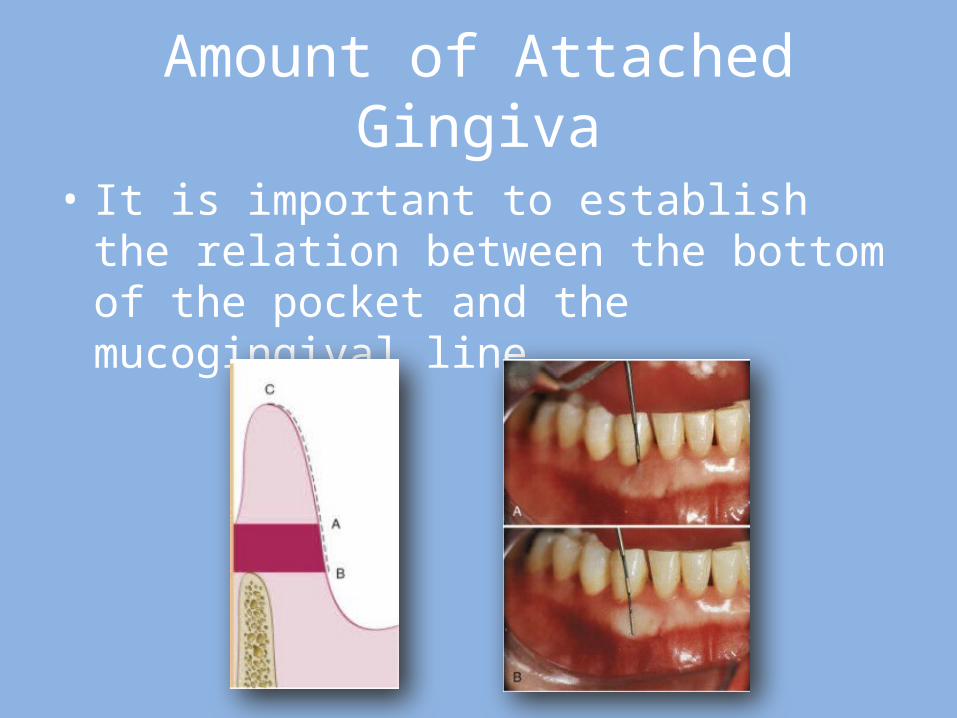
Amount of Attached Gingiva
• It is important to establish the relation between the bottom of the pocket and the mucogingival line
• Degree of Gingival Recession This measurement is taken with a periodontal probe
from the CEJ to the gingival crest, and it is drawn on the patient's chart.
• Alveolar Bone Loss Alveolar bone levels are evaluated by clinical and
radiographic examination.
• Palpation Palpating the oral mucosa in the lateral and apical
areas of the tooth may help locate the origin of radiating pain that the patient cannot localize.
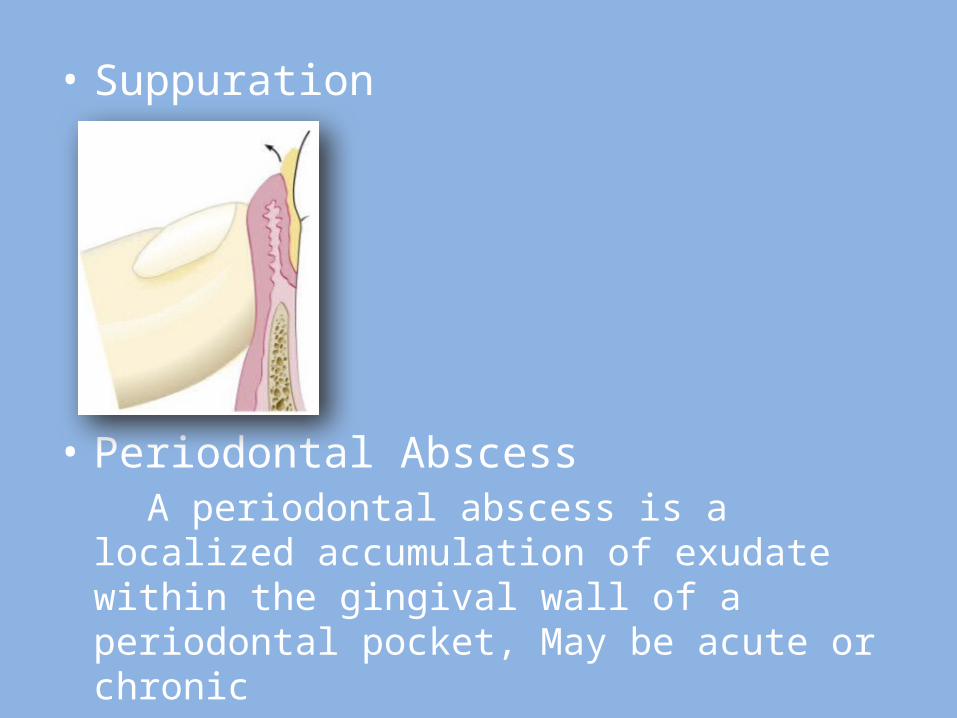
• Suppuration
• Periodontal Abscess A periodontal abscess is a localized accumulation of
exudate within the gingival wall of a periodontal pocket, May be acute or chronic
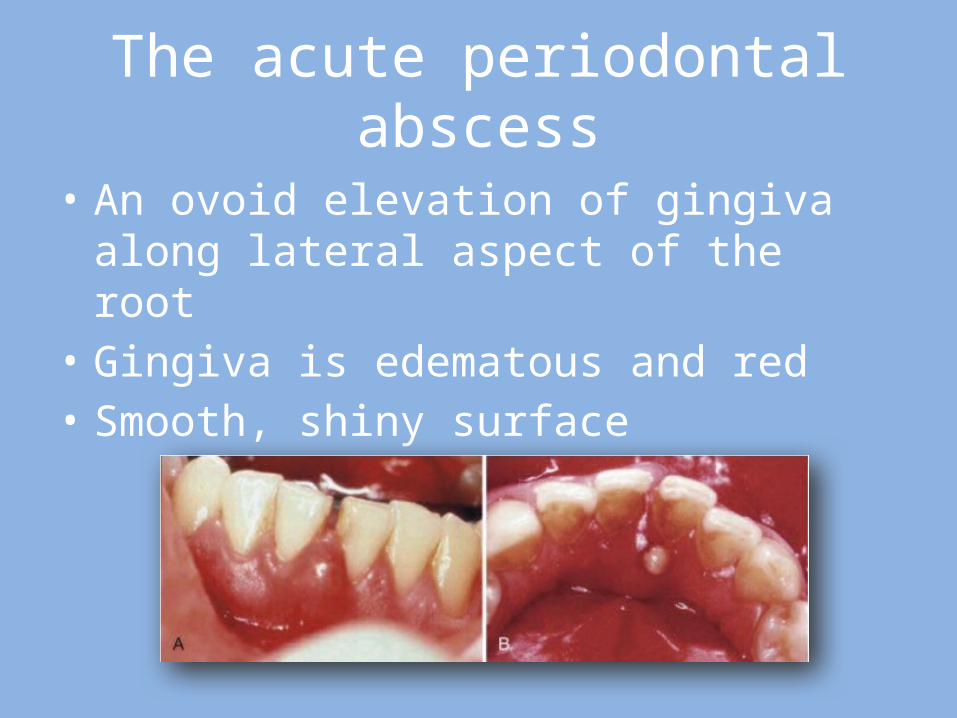
The acute periodontal abscess
• An ovoid elevation of gingiva along lateral aspect of the root
• Gingiva is edematous and red• Smooth, shiny surface
The acute periodontal abscess
• Throbbing• Tenderness of gingiva to palpation• Radiating pain• Pain of the tooth to palpation• Tooth mobility
The chronic periodontal abscess
• Presents a sinus that opens into the gingival mucosa
• There might be a history of intermittent exudation
• Orifice of the sinus is hard to detect• The sinus may be covered by a small, pink,
beadlike mass of granulation tissue• Usually asymptomatic
Periodontal Abscess and Gingival Abscess
• The principal differences between the periodontal abscess and the gingival abscess are location and history
• The gingival abscess is confined to the marginal gingiva, and it often occurs in previously disease-free areas
• It is usually an acute inflammatory response to forcing of foreign material into the gingiva
• The periodontal abscess involves the supporting periodontal structures and generally occurs in the course of chronic destructive periodontitis.

Periodontal Abscess and Periapical Abscess
• If the tooth is nonvital, the lesion is most likely periapical. However, a previously nonvital tooth can have a deep periodontal pocket that can abscess.
• Moreover, a deep periodontal pocket can extend to the apex and cause pulpal involvement and necrosis
• An apical abscess may spread along the lateral aspect of the root to the gingival margin
• However, when the apex and lateral surface of a root are involved by a single lesion that can be probed directly from the gingival margin, the lesion is more likely to have originated as a periodontal abscess
• A draining sinus on the lateral aspect of the root suggests periodontal rather than apical involvement
Laboratory Aids to Clinical Diagnosis
After consulting the patient’s physician about presence of any systemic disease.
• Analyses of blood smears• Blood cell counts• White blood cell differential counts• erythrocyte sedimentation rates