Embed Size (px)
Citation preview
Cardiovascular Physiology
Dr. Hussein Farouk Sakr
Contractility
• The ability of the cardiac muscle to convert electrical and chemical energies into mechanical energy.• The ability of the cardiac muscle to pump blood.• The pumping action of the heart generates the blood pressure that force
the blood to circulate in the vascular tree
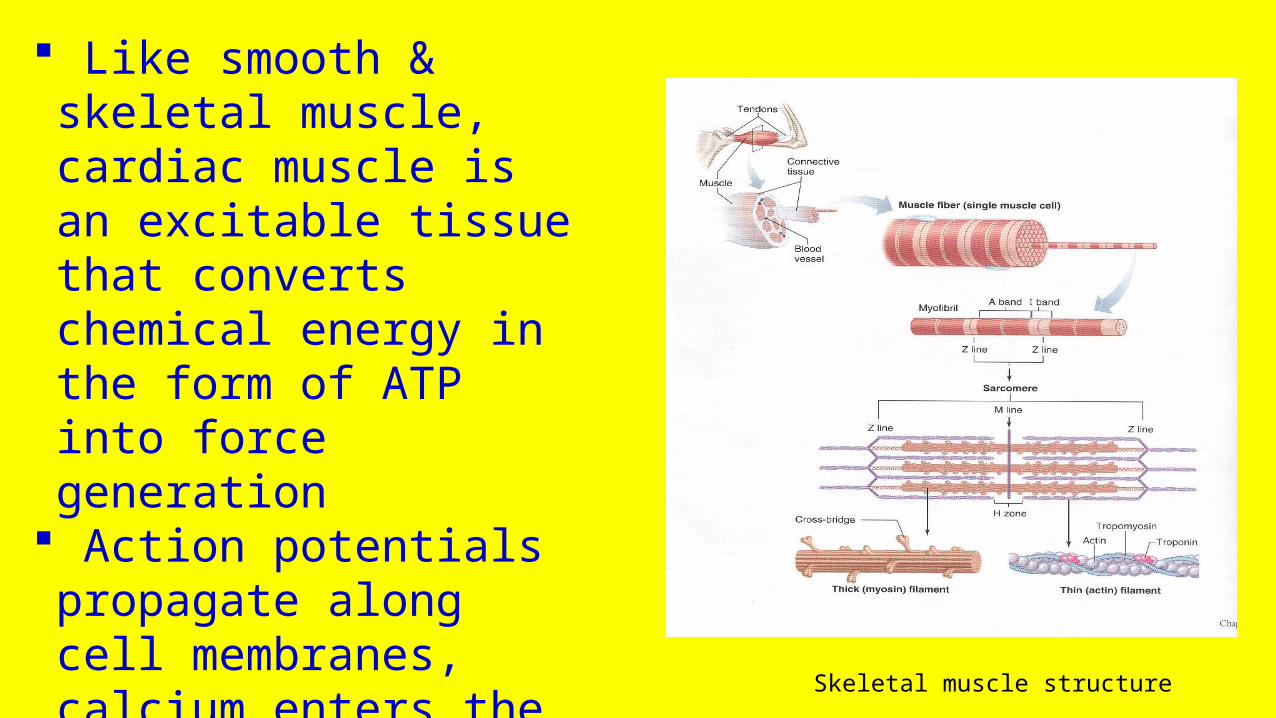
Like skeletal muscle, cardiac muscle has striated appearance, which results from the arrangement of numerous thick and thin filaments
The thick and thin filaments in each myofibril are arranged in a repeating pattern along the length of the myofibril. One unit of this repeating pattern is known as a sarcomere
The thick filaments are composed almost entirely of the protein myosin
The thin filaments are principally composed of the protein actin, as well as two other proteins – troponin and tropomyosin
Contractile and regulatory proteins
Contractile proteins: actin and myosin
Regulatory proteins: troponin and tropomyosin
Like smooth & skeletal muscle, cardiac muscle is an excitable tissue that converts chemical energy in the form of ATP into force generation
Action potentials propagate along cell membranes, calcium enters the cytosol, and the cycling of force-generating cross-bridges is activated
Skeletal muscle structure
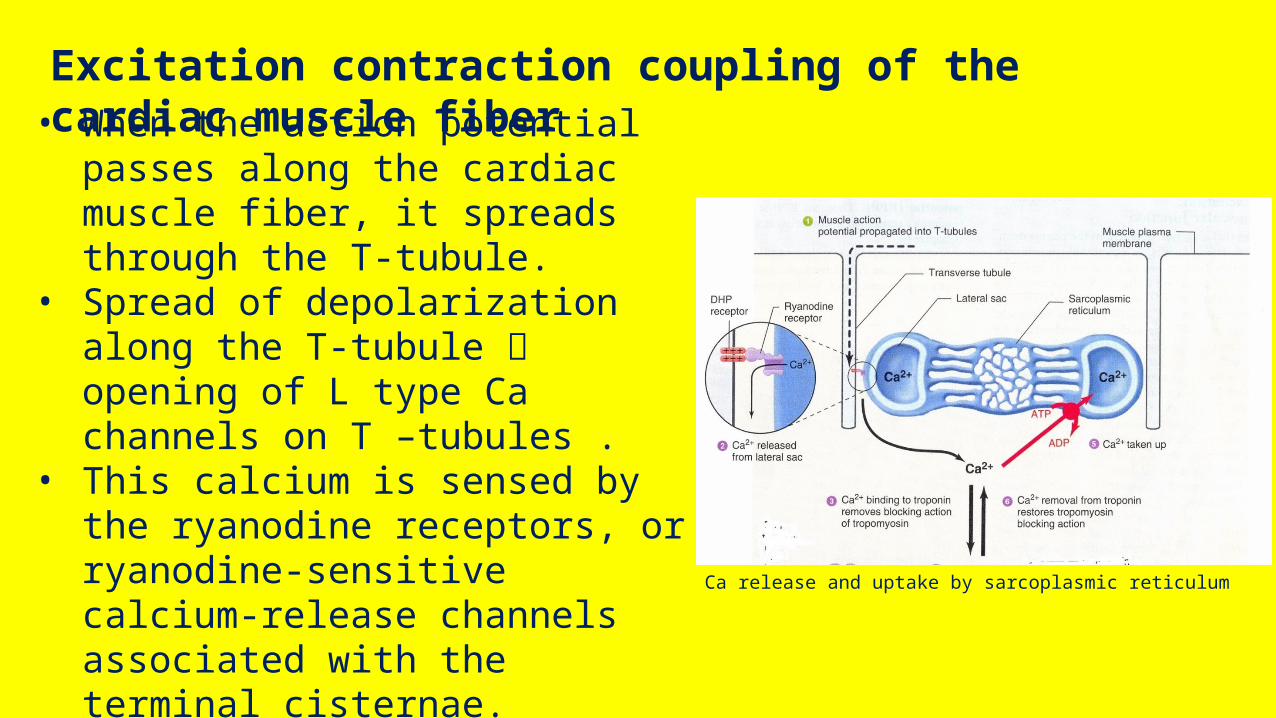
Excitation contraction coupling of the cardiac muscle fiber• When the action potential passes along
the cardiac muscle fiber, it spreads through the T-tubule.
• Spread of depolarization along the T-tubule opening of L type Ca channels on T –tubules .
• This calcium is sensed by the ryanodine receptors, or ryanodine-sensitive calcium-release channels associated with the terminal cisternae.
• This triggers the subsequent release of large quantities of calcium stored in the terminal cisternae through the calcium-release channels.
Ca release and uptake by sarcoplasmic reticulum
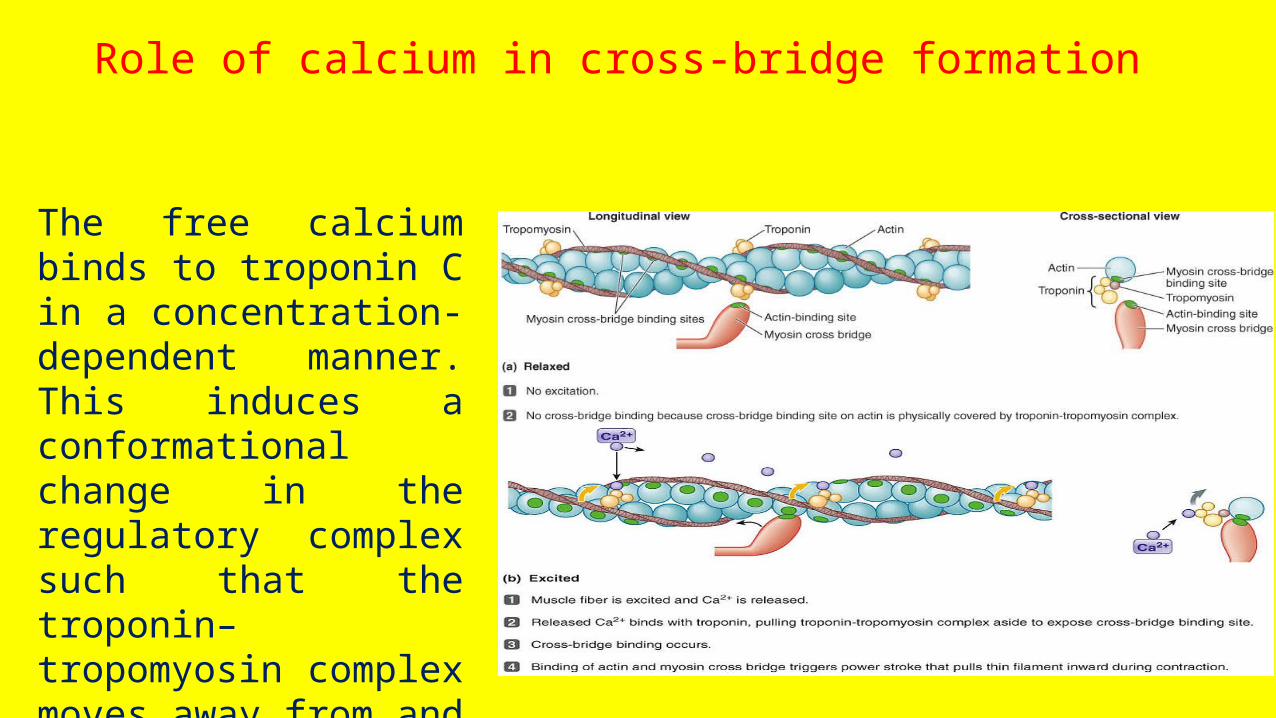
The free calcium binds to troponin C in a concentration- dependent manner. This induces a conformational change in the regulatory complex such that the troponin–tropomyosin complex moves away from and exposes a myosin binding site on the actin molecule.
Role of calcium in cross-bridge formation
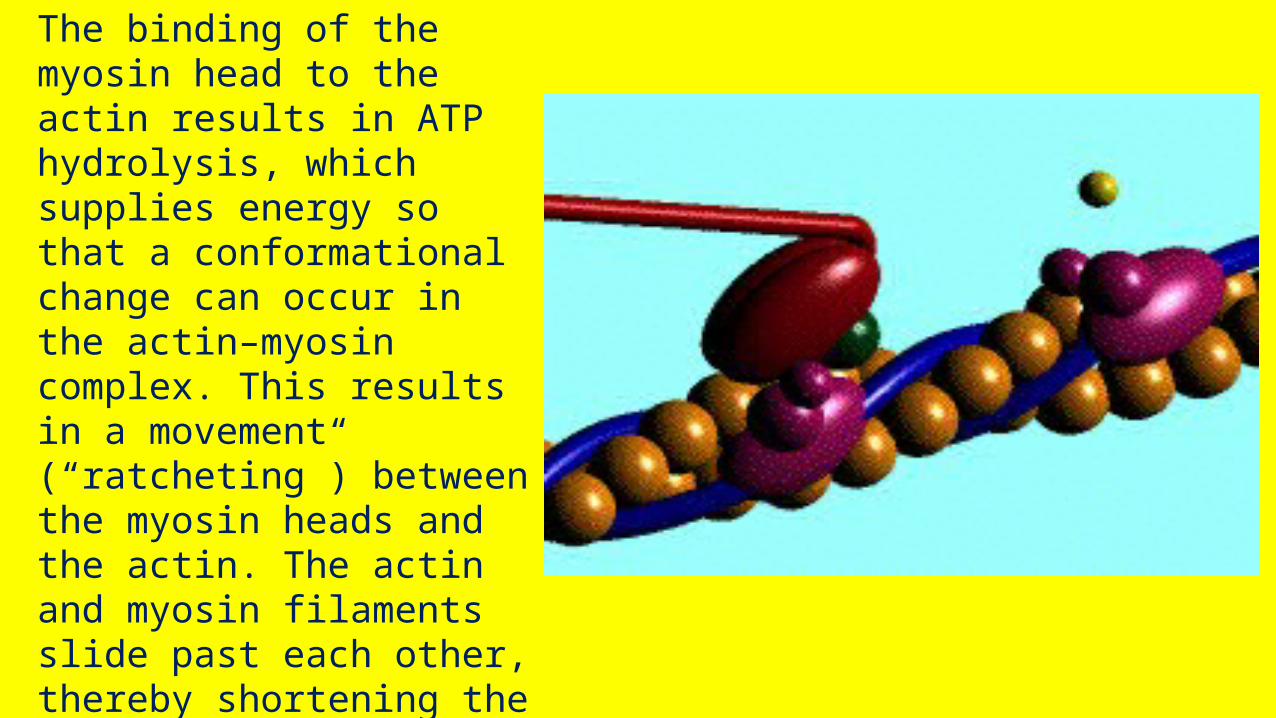
The binding of the myosin head to the actin results in ATP hydrolysis, which supplies energy so that a conformational change can occur in the actin–myosin complex. This results in a movement (“ratcheting”) between the myosin heads and the actin. The actin and myosin filaments slide past each other, thereby shortening the sarcomere length (this is referred to as the sliding filament theory of muscle contraction)
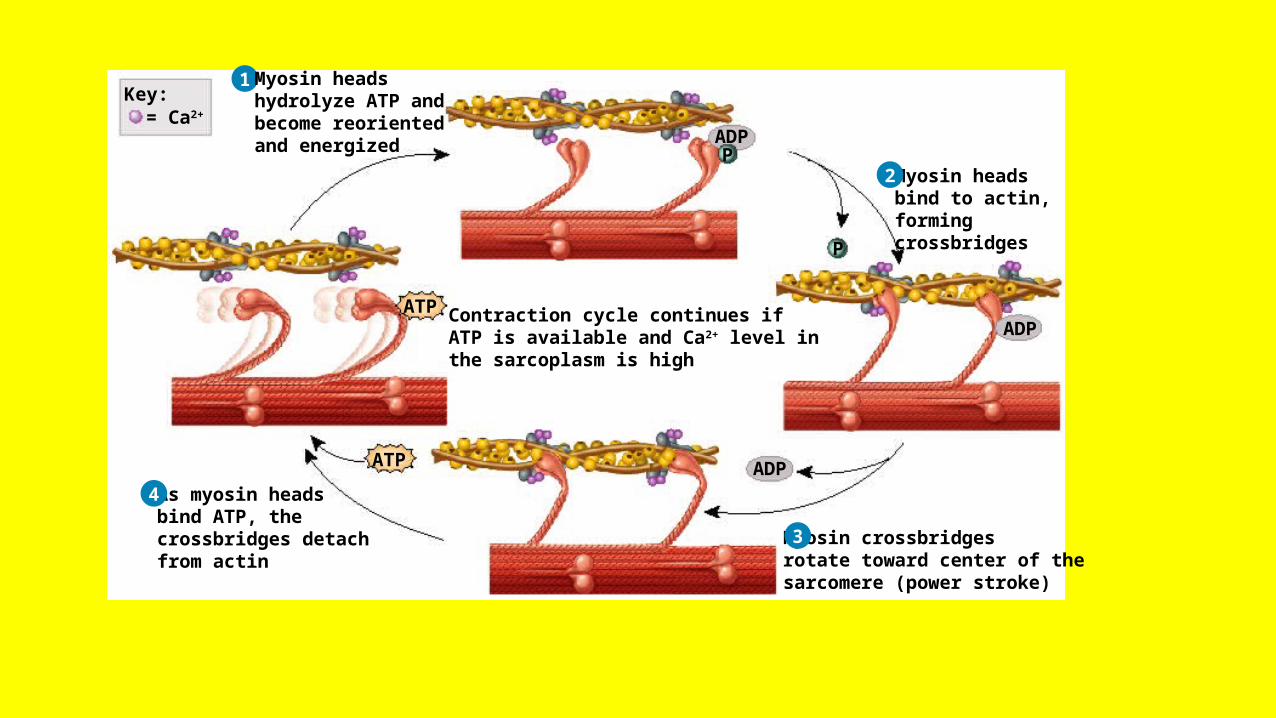
1 Myosin headshydrolyze ATP andbecome reorientedand energized
Myosin headsbind to actin,formingcrossbridges
Myosin crossbridgesrotate toward center of thesarcomere (power stroke)
As myosin headsbind ATP, thecrossbridges detachfrom actin
Contraction cycle continues ifATP is available and Ca2+ level inthe sarcoplasm is high
ADP
ADP
ADP
ATP
P
P
= Ca2+Key:
ATP
2
3
4

• Toward the end of the myocyte action potential, calcium entry into the cell diminishes and the sarcoplasmic reticulum sequesters calcium by an ATP-dependent calcium pump, sarcoplasmic reticulum calcium ATPase.
• As intracellular calcium concentration declines, calcium dissociates from troponin C, which causes a conformational change in the troponin– tropomyosin complex; this again leads to troponin– tropomyosin inhibition of the actin binding site.
• At the end of the cycle, a new ATP binds to the myosin head, displacing the adenosine diphosphate (ADP), and the initial sarcomere length is restored. Thus, ATP is required both for providing the energy of contraction and for relaxation.
Mechanism of relaxation
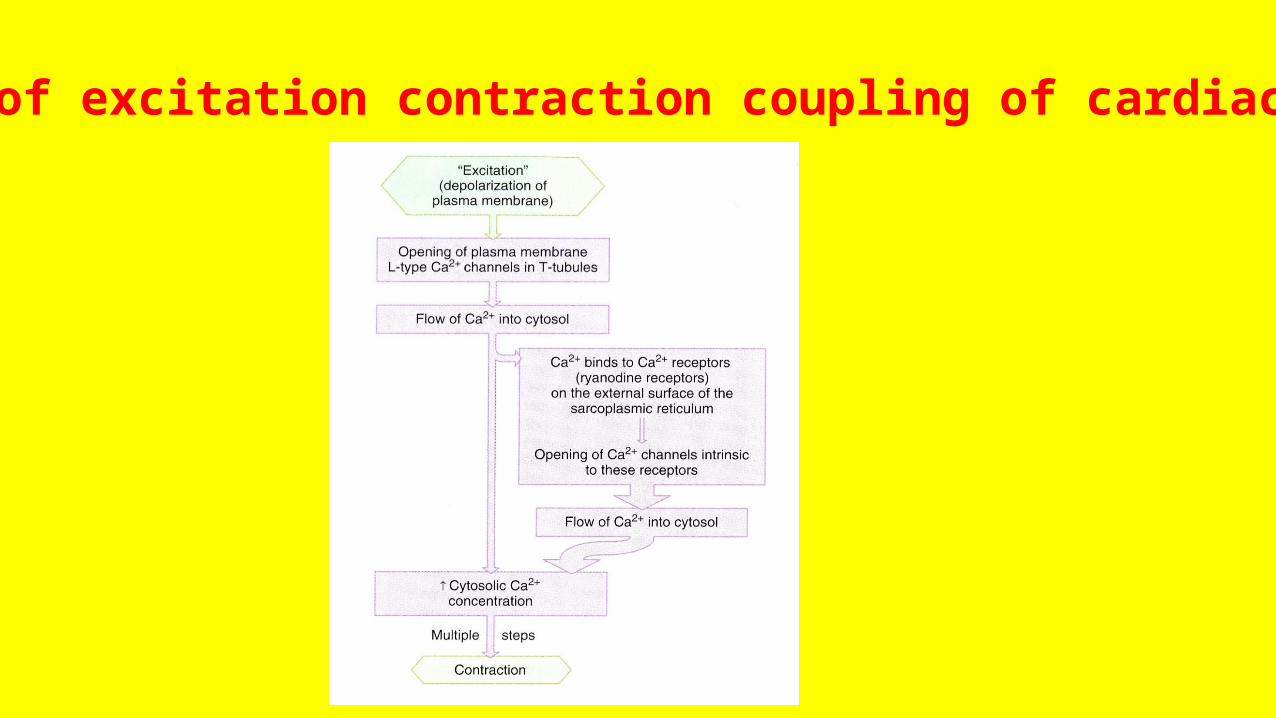
Summary of excitation contraction coupling of cardiac myocyte
Rules controlling contractility
1. All or non law: • This means that: the cardiac muscle when stimulated it either
produces maximum response or does not produces response at all, provided that the other factors are kept constant.
• The 2 atria are considered as one unit and the 2 ventricles are considered as one unit.
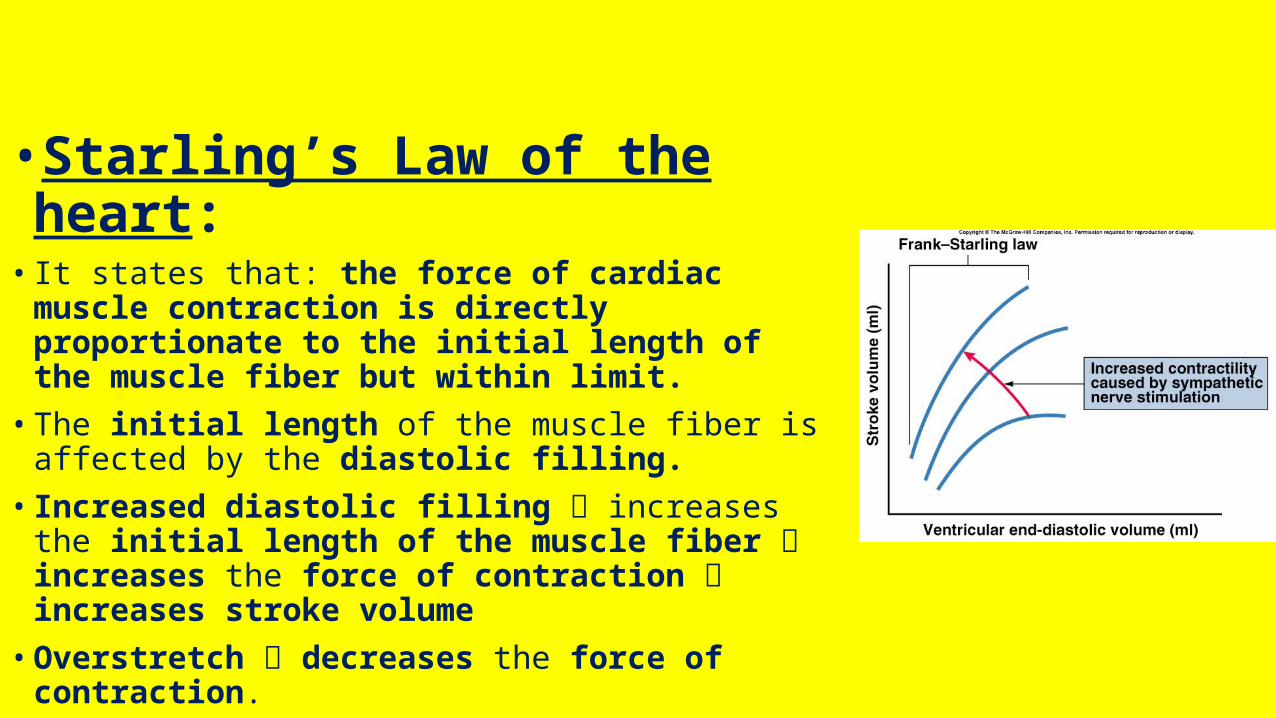
•Starling’s Law of the heart:• It states that: the force of cardiac muscle contraction is
directly proportionate to the initial length of the muscle fiber but within limit.• The initial length of the muscle fiber is affected by the
diastolic filling.• Increased diastolic filling increases the initial length of the
muscle fiber increases the force of contraction increases stroke volume • Overstretch decreases the force of contraction.• Normally the pericardium prevents the overstretch of the
cardiac muscle fibers.
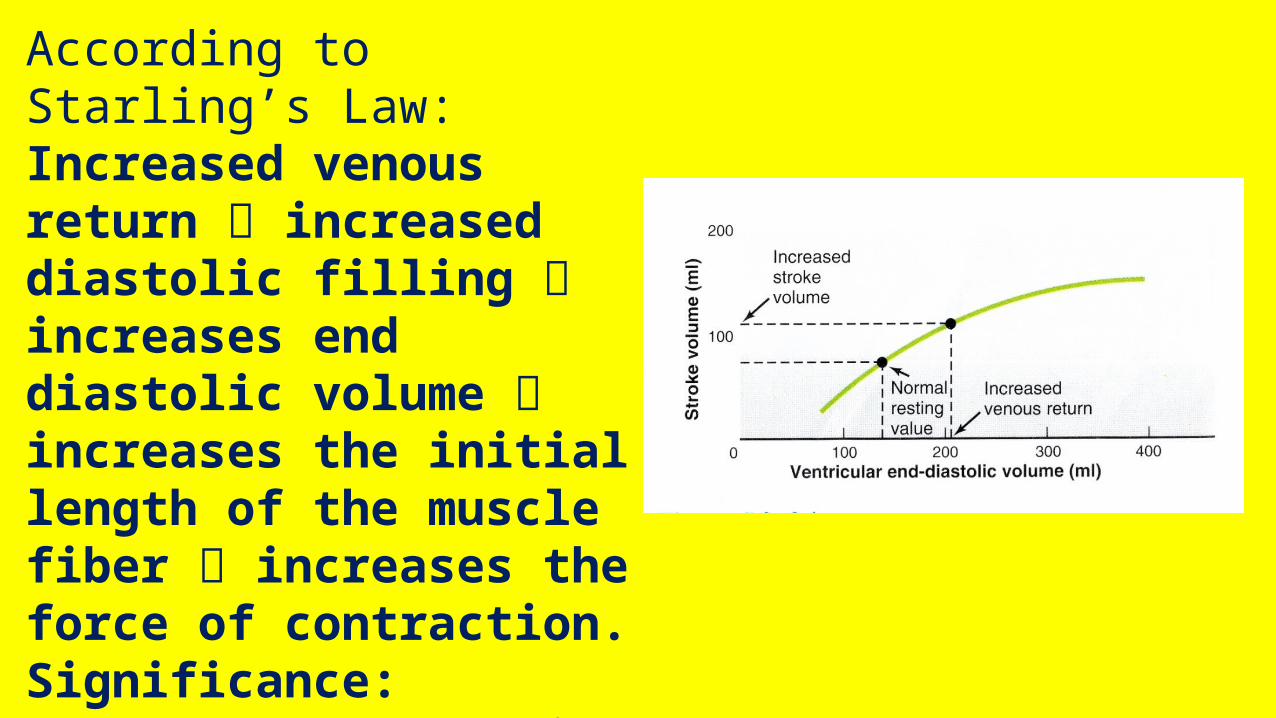
According to Starling’s Law:Increased venous return increased diastolic filling increases end diastolic volume increases the initial length of the muscle fiber increases the force of contraction.Significance: prevents accumulation of blood on venous side.Origin: Myogenic
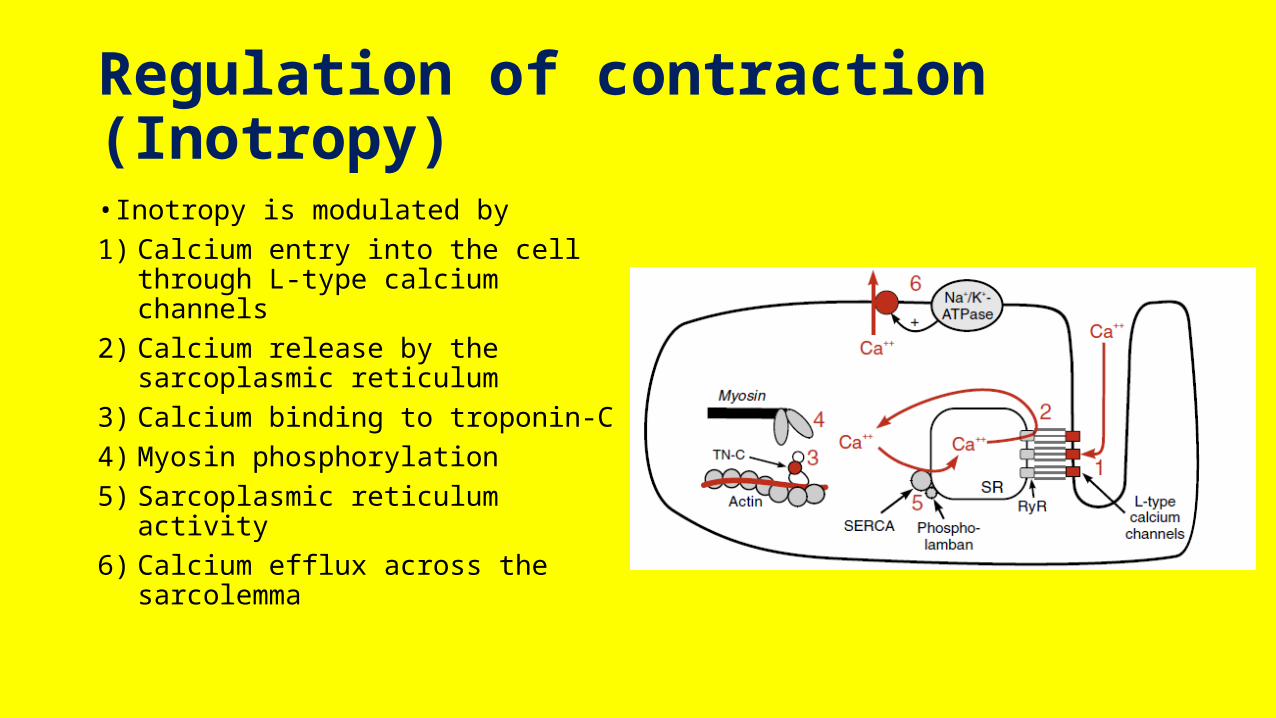
Regulation of contraction (Inotropy)• Inotropy is modulated by 1) Calcium entry into the cell
through L-type calcium channels2) Calcium release by the
sarcoplasmic reticulum3) Calcium binding to troponin-C4) Myosin phosphorylation5) Sarcoplasmic reticulum activity6) Calcium efflux across the
sarcolemma
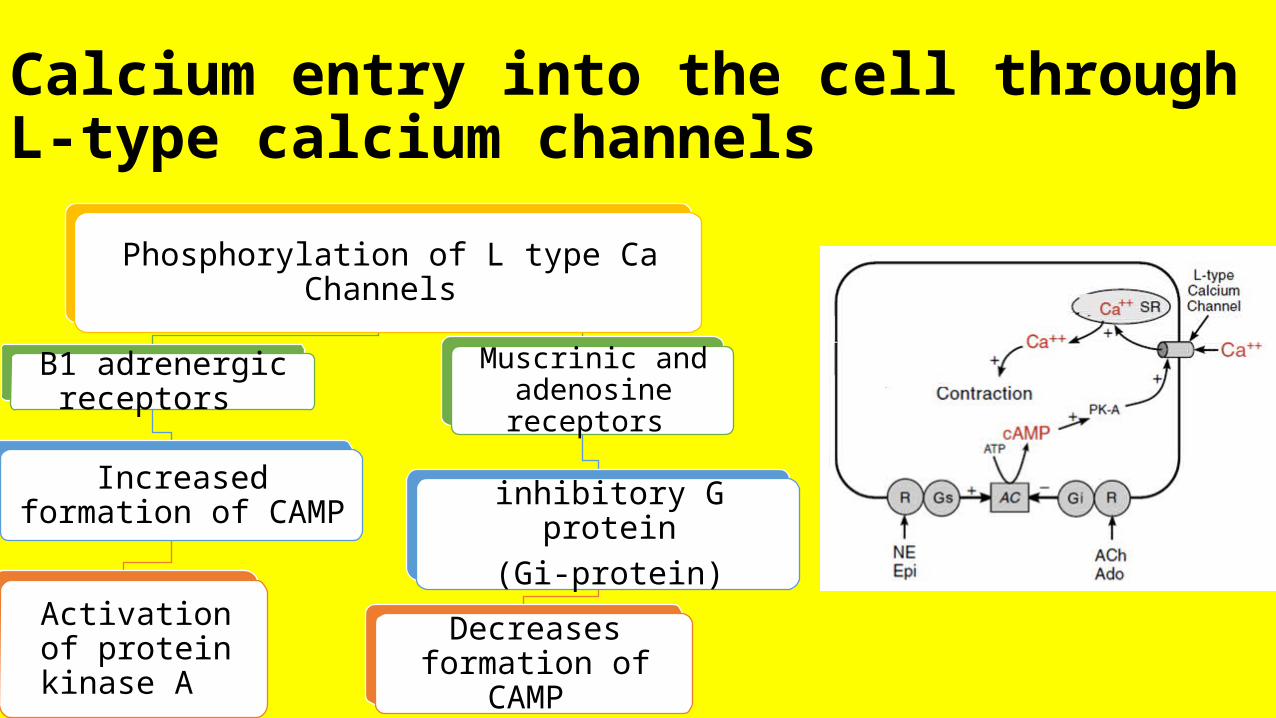
Calcium entry into the cell through L-type calcium channels
Phosphorylation of L type Ca Channels
B1 adrenergic receptors
Increased formation of CAMP
Activation of protein kinase A
Muscrinic and adenosine receptors
inhibitory G protein(Gi-protein)
Decreases formation of CAMP
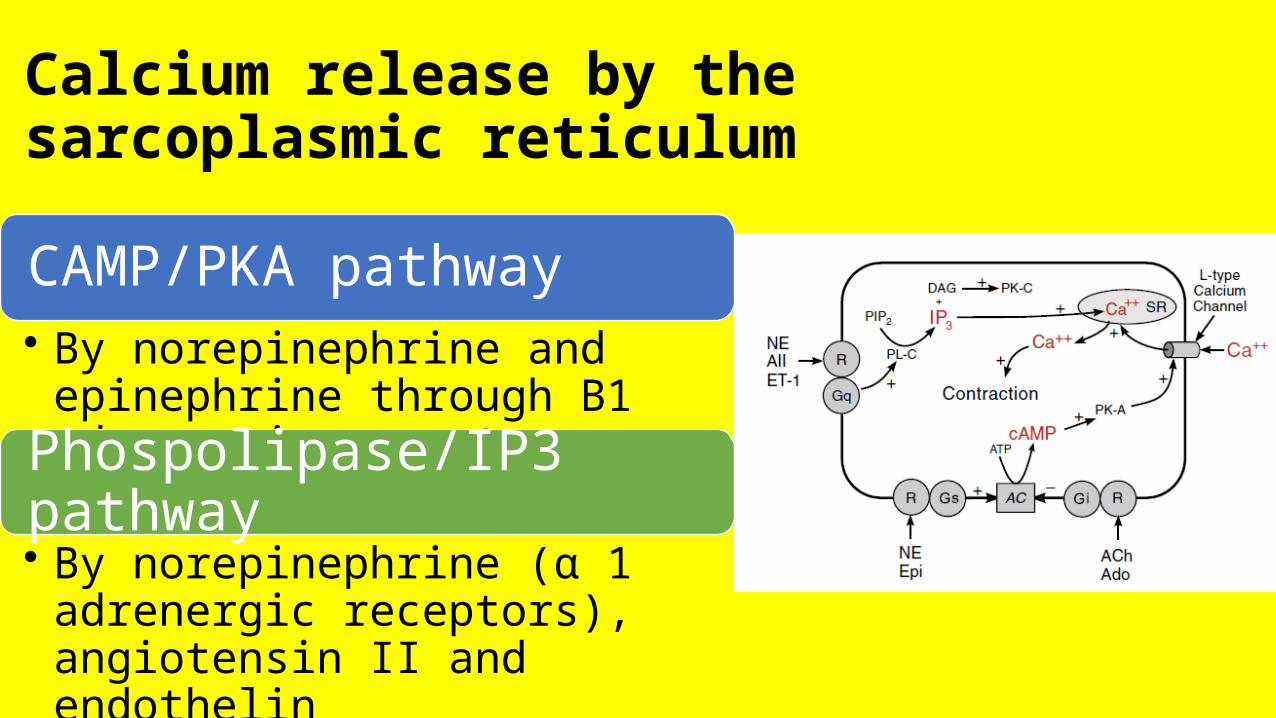
Calcium release by the sarcoplasmic reticulum
CAMP/PKA pathway • By norepinephrine and epinephrine
through B1 adrenergic receptors
Phospolipase/IP3 pathway • By norepinephrine (α 1 adrenergic
receptors), angiotensin II and endothelin
Calcium binding to troponin-C• The binding of Ca to troponin C is
determined by the availability of Ca • Increased cytoplasmic
concentration is associated with increased affinity between Ca and troponin C• Acidosis, which occurs during
myocardial hypoxia, has been shown to decrease troponin C affinity for calcium. This may be one mechanism by which acidosis decreases the force of contraction
Myosin ATPase Activity• Increased cAMP is known to be
associated with increased phosphorylation of the myosin heads, which may increase inotropy. The physiologic significance of this mechanism, however, is uncertain
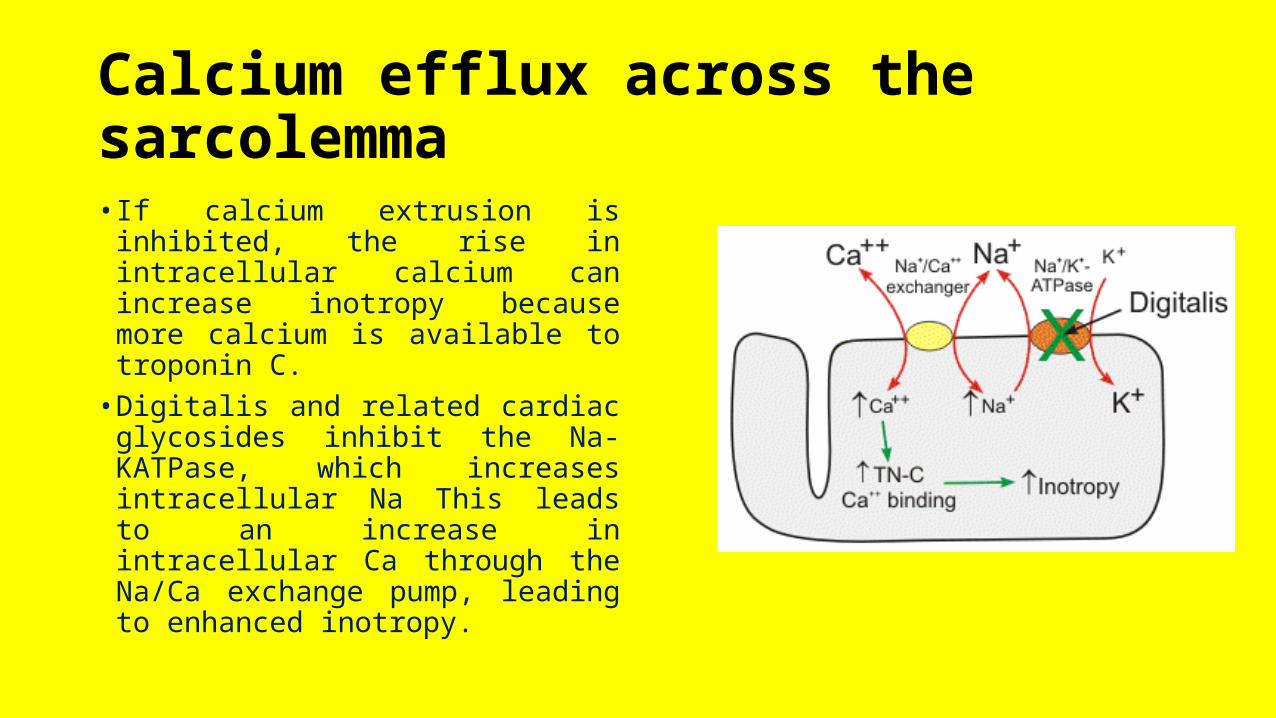
Calcium efflux across the sarcolemma• If calcium extrusion is inhibited,
the rise in intracellular calcium can increase inotropy because more calcium is available to troponin C.• Digitalis and related cardiac
glycosides inhibit the Na-KATPase, which increases intracellular Na This leads to an increase in intracellular Ca through the Na/Ca exchange pump, leading to enhanced inotropy.
Regulation of Relaxation (Lusitropy)• The rate of myocyte relaxation (lusitropy) is determined by the ability
of the cell to rapidly reduce the intracellular concentration of calcium following its release by the sarcoplasmic reticulum. • This reduction in intracellular calcium causes calcium that is bound to
troponin- C to be released, thereby permitting the troponin-tropomyosin complex to resume its resting, inactivated conformation.
The rate that calcium enters the cell at restand during action potentials influences intracellularconcentrations. Under somepathologic conditions (e.g., myocardialischemia), the cell becomes more permeableto calcium, leading to “calcium overload,”which impairs relaxation.
The rate with which calcium leaves the cellthrough the sarcolemmal calcium ATPasepump and the Na/Ca exchange pumpaffects intracellular concentrations.Inhibiting these transport systemscan cause intracellular calcium concentrationsto increase to a point at whichrelaxation is impaired.
Phosphorylation of phospholamban, a regulatory protein associated with sarcoplasmic reticulum. Phosphorylation of phospholamban removes its inhibitory effect on sarcoplasmic reticulum. This is a normal physiologic mechanism in response to B adrenoceptor stimulation, which increases cAMP and PK-A, the latter of which phosphorylates phospholamban. The impairment of the activity of the SERCA pump, as occurs in some forms of heart failure, causes intracellular calcium concentrations to rise, leading to impaired relaxation.
The binding affinity of troponin-C for calcium also influences lusitropy. Calcium binding to troponin-C can be modulated by PK-A phosphorylation of troponin-I. This increases calcium dissociation from troponin- C, thereby increasing relaxation. The increased lusitropy caused by B adrenoceptor stimulation may be partly related to troponin-I phosphorylation.