Embed Size (px)
Citation preview

Cardiac Rhythm Disorders

Initial Management of Cardiac Arrest The first step in any potential cardiac arrest
patient is to:• Make sure the patient is truly unresponsive.• Call for help: Call 911/activate Emergency Medical Services (EMS). It is critical to make sure that the patient is
truly unresponsive and not just sleeping or having a syncopal episode. Rescue breaths on a person who is breathing are counterproductive.
Performing chest compressions on a person with a pulse is dangerous.

After the patient has been shown to be unresponsive, and EMS activated, the next step is:
1. Open the Airway: head tilt, chin lift, jaw thrust.2. Give rescue Breaths if not breathing.3. Check pulse and start Chest compressions if pulseless.



CPR does not restart the heart; CPR keeps the patient alive until cardioversion can be performed .
TIPWhen is a "precordial thump" the answer?• Very recent onset of arrest (less than 1 0 minutes) with no defibrillator available• You know it is recent because you saw it happen ("witnessed").


Pulselessness The sudden loss of a pulse can be
caused by:1.Asystole2. Ventricular fibrillation (VF)3.Ventricular tachycardia (VT)4. Pulseless electrical activity (PEA)The best initial management of all forms of pulselessness is CPR.


1. Asystole
Besides CPR, therapy for asystole is with epinephrine.
Vasopressin is an alternative to epinephrine. They both constrict blood vessels in tissues such as the skin.
This shunts blood into critical central areas like the heart and brain.


Ventricular Fibrillation The best initial therapy for ventricular
fibrillation (VF) is an immediate, unsynchronized cardioversion followed by the resumption of CPR if this was not effective.
Unsynchronized cardioversion is synonymous with defibrillation.
Generally, all electrical cardioversions should be synchronized to the cardiac cycle except VF and pulseless VT.
In VF, there is no organized electrical activity to synchronize with.


After another attempt at defibrillation, the most appropriate next step in management is epinephrine or vasopressin followed by another electrical shock.
Medications do not restart the heart. They make the next attempt at defibrillation more likely to succeed.
Amiodarone or lidocaine is given next to try to get subsequent shocks to be more successful. Magnesium is given with ventricular arrhythmia without waiting for a level. Amiodarone is the first choice.


VF is managed with shock,drug, shock, drug, shock,drug, and CPR at all timesin between the shocks.


Pulseless Electrical Activity Pulseless electrical activity (PEA),
formerly called electrical-mechanical dissociation (EMD), means that the heart is electrically normal, but there is no motor contraction.
In other causes of PEA, the heart may still be contracting but without blood inside there will be no meaningful cardiac output.


TIP To diagnose PEA, look for a patient with
a normal EKG and no pulse.

TreatmentSince the treatment of PEA is to correct the underlying cause, knowing the etiology is identical to knowing the treatment. PEA is caused by: Tamponade Tension pneumothorax Hypovolemia and hypoglycemia Massive pulmonary embolus (PE) Hypoxia, hypothermia, metabolic acidosis Potassium disorders, either high or low







Ventricular Tachycardia VT is a wide complex tachycardia with a regular
rate. Management is entirely based on the hemodynamic status.
• Pulseless VT: Manage in exactly the same way as VF.• Hemodynamically stable VT: Treat with medications such as amiodarone, then lidocaine, then procainamide. If all medical therapy fails, then cardiovert the patient.• Hemodynamically unstable VT: Perform electrical cardioversion several times, followed by medications such as amiodarone, lidocaine, or procainamide.


Hemodynamic instability is defined as:• Chest pain• Dyspnea/CHF• Hypotension• Confusion
These qualities of instability are the same for all rhythm disturbances.
~ TIPDirect intracardiac medication administration is always a wrong answer

Atrial Arrhythmias Atrial rhythm disturbances are rarely
associated with hemodynamic compromise because cardiac output is largely dependent upon ventricular output, not atrial output. Look for the following findings in the history to suggest an atrial arrhythmia:
• Palpitations, dizziness, or lightheadedness• Exercise intolerance or dyspnea• Embolic stroke

TIP An irregularly irregular rhythm
suggests atrial fibrillation as "the most likely diagnosis" even before an EKG is done.
Atrial fibrillation is the most common arrhythmia in the United States.

Atrial Fibrillation and Atrial Flutter
These 2 disorders have nearly identical management. The major points of difference are:
• Flutter is a regular rhythm whereas fibrillation is irregular.• Flutter usually goes back into sinus rhythm or deteriorates into fibrillation.




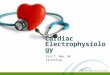
An irregular heart rhythm (#1) with no discernible P waves is shown. Without close examination of an ECG, rapid AF may be hard to differentiate from a narrow supraventricular tachycardia, which has a more regular rhythm (#2). The 2 conditions can have similar symptoms of heart palpitations and shortness of breath. Patients with rapid AF are commonly given adenosine to either aid in the diagnosis or treat presumed supraventricular tachycardia. The irregularity of AF can be difficult to discern, but the underlying atrial rhythm may be accurately determined when conduction to the ventricles is transiently disrupted. Atrial flutter, which typically has sawtooth flutter waves (#3), can also be diagnosed with adenosine. ECG tracings courtesy of ECG Wave-Maven.

Treatment Hemodynamically unstable atrial
arrhythmias are managed with synchronized! cardioversion.
Synchronization prevents electricity from being delivered during the refractory period (ST-T wave).
Synchronization helps prevent deterioration into VT or VF.
Hemodynamic instability is defined as it is for VT: hypotension, confusion, CHF, and chest pain.

Chronic atrial fibrillation
should be anticoagulated before cardioversion.
Unstable, acute disease does not need anticoagulation.

Chronic Atrial Fibrillation
By definition, chronic atrial fibrillation is defined as lasting for more than 2 days. It takes several days for there to be a risk of clot formation.
Routine cardioversion is not indicated. The majority of those who are converted into sinus rhythm will not stay in sinus.

Atrial fibrillation and flutter are caused by anatomic abnormalities of the atria from hypertension or valvular heart disease.
Shocking the patient into sinus rhythm does not correct a dilated left atrium.
Over 90% will revert to fibrillation even with the use of antiarrhythmic medications . ... TIP
Rate control and anticoagulation are the standard of care for atrial fibrillation.

Treatment The best initial therapy for fibrillation and flutter is to
control the rate with beta blockers, calcium channel blockers, or digoxin.
Once the rate is under 100 per minute, the most appropriate next step is to give warfarin, dabigatran, or rivaroxaban.
1. Slow the rate.2. Anticoagulate. (Aspirin for low risk.) The calcium blockers used to control heart rate with atrial
arrhythmias are diltiazem and verapamil. These reliably block the AV node. The other calcium channel blockers control BP.

Rate control drugs do not convert the patient into sinus rhythm
No matter how much you might think it better to shock every patient into sinus, it just does not work in the long run.

Warfarin, Dabigatran, Rivaroxaban
Without anticoagulation, there will be about 6 embolic strokes per year for every 100 patients with atrial fibrillation (6% a year).
When the INR is maintained between 2 and 3, the rate is 2% to 3%.
You need to use heparin only if there is a current clot in the atrium.
Heparin is not necessarybefore starting a patient onwarfarin.

Atrial fibrillation is caused by anatomic cardiac defects dilating the atrium.
These defects do not go away with cardioversion. That is why the vast majority revert.
Many patients with acute atrial fibrillation from alcohol, caffeine, cocaine, or transient ischemia will simply convert back to sinus rhythm on their own.

Hence, acute disease normalizes spontaneously; don't force it.
Chronic disease reverts into the arrhythmia. Don't force it either.
Dabigatran is an alternative oral anticoagulant for a trail fibrillation. It prevents stroke and does not need to be monitored with INR.
Atrial rhythm problems can causeacute pulmonary edema from loss of atrial contribution in those witha cardiomyopathy.

Lone" Atrial Fibrillation: CHADS Score ~1
Patients with a low risk of stroke can have their strokes safely prevented with using aspirin alone without warfarin, dabigatran, or rivaroxaban as an anticoagulant.
If the annual risk of stroke is only 2% to 3% per year, there is no point in subjecting these patients to the 1% a year risk of major bleeding.

"Major" bleeding from warfarin is defined as:
-Intracranial hemorrhage-Requiring a transfusion
Normally the atrium contributes 10% to 15% to cardiac output. In a diseased heart, this rises to 30% to 50%.

CHADS ScoreC: CHF or cardiomyopathyH: hypertensionA: age >75D: diabetesS: stroke or TIA = 2 points
When CHADS score is 1 or less, use aspirin. When CHADS score is 2 or more, use warfarin, dabigatran, or rivaroxaban.