Embed Size (px)
Citation preview

Cardiac Diseases in Pregnancy Cardiac Diseases in Pregnancy

Objectives:Objectives:
Normal Physiology during pregnancyNormal Physiology during pregnancy
Cardiac TestingCardiac Testing
Common cardiac problemsCommon cardiac problems

about 1% of pregnancies complicated by heart diseasesleading cause of maternal mortalityMortality rate 50% in case pulmonary hypertension
CARDIOVASCULAR CARDIOVASCULAR DISORDERSDISORDERS

Physiologic adaptation to pregnancy Physiologic adaptation to pregnancy
Increase blood volume on 40 -50 %Increase blood volume on 40 -50 % Increase cardiac output 30-50%Increase cardiac output 30-50% Decreased systemic vascular resistance Decreased systemic vascular resistance The heart elevated upward and rotated forward to the leftThe heart elevated upward and rotated forward to the left Pulse increase about 10-15 beat/min after 14-20 weeks, Pulse increase about 10-15 beat/min after 14-20 weeks,
palpitationpalpitation Disturbed rhythm: arrhythmia, premature atrial contractions, Disturbed rhythm: arrhythmia, premature atrial contractions,
premature ventricalar systolepremature ventricalar systole Increase clot factors (VII, VIII, IX, X, fibrinogen)Increase clot factors (VII, VIII, IX, X, fibrinogen) Cardiac output changes during labor and birthCardiac output changes during labor and birth Intravascular volume changes just after childbirthIntravascular volume changes just after childbirth
Cardiac hypertrophyCardiac hypertrophy

Physiologic adaptation to pregnancyPhysiologic adaptation to pregnancy
If cardiac changes are not well tolerated If cardiac changes are not well tolerated cardiac failure can develop during pregnancy, cardiac failure can develop during pregnancy, labour, postpartumlabour, postpartum
If myocardial disease develops, valvular If myocardial disease develops, valvular disease exists or congenital heart defect is disease exists or congenital heart defect is present, cardial decompensation is present, cardial decompensation is anticipated anticipated

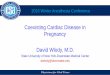
Percent change in heart rate, stroke volume, and Percent change in heart rate, stroke volume, and cardiac output measured in the lateral position cardiac output measured in the lateral position
throughout pregnancy compared with pregnancy throughout pregnancy compared with pregnancy valuesvalues

Hemodynamic changes during Hemodynamic changes during labor and deliverylabor and delivery
Anxiety, pain, uterine contraction.Anxiety, pain, uterine contraction. Oxygen consumption Oxygen consumption ↑ threefold.↑ threefold. ↑ ↑ CO during labor (↑ SV and ↑ HR).CO during labor (↑ SV and ↑ HR). ↑ ↑ SBP & DBP (especially 2SBP & DBP (especially 2ndnd stage) stage)
Those changes are influenced by the form of Those changes are influenced by the form of anesthesia and analgesia.anesthesia and analgesia.

Hemodynamic changes Hemodynamic changes post partumpost partum
Blood shifting “auto-transfusion” (from the contracting uterus to the
systemic circulation)
Increase in effective blood volume
Substantial increase in LV filling pressure, SV and CO
Clinical deterioration
Blood loss during delivery-
• HR and CO return to pre-labor values within 1 hour. MAP and SV within 24 hours.• Hemodynamic adaptation persists post partum and return to pre-pregnancy values within 12-24 weeks after delivery.
Increase in venous return(relief of caval compression)

HistoryExercise capacity
Current or past evidence of HFAssociated arrhythmias
Physical exam
Cardiac HemodynamicsSeverity of heart disease, PA pressures
Echo, MRI.
Exercise testingUseful if the history is inadequate to allow assessment of functional capacity
During pregnancyEvaluate once each trimester and whenever there is change in symptoms
Multidisciplinary approach, Fetal Echo
Bef
ore
co
nce
pti
on
During Labor & DeliveryMultidisciplinary approach (Obstetrician, Cardiologist, Anesthesiologist)
Tailor management to specific needs

High-risk pregnancyHigh-risk pregnancy Pulmonary HTN and Eisenmenger’s Pulmonary HTN and Eisenmenger’s
syndrome.syndrome. Symptomatic obstructive cardiac lesions:Symptomatic obstructive cardiac lesions:
■ AS, PS, uncorrected coarctation of the aorta.AS, PS, uncorrected coarctation of the aorta. Marfan’s Syndrome with dilated aortic root.Marfan’s Syndrome with dilated aortic root. Systemic ventricular dysfunction Systemic ventricular dysfunction Severe cyanotic heart disease.Severe cyanotic heart disease. Patients with prosthetic valves.Patients with prosthetic valves. Significant uncorrected CHD. Significant uncorrected CHD.

Contraindications to PregnancyContraindications to Pregnancy
Lesion Maternal death rate
(%)
• Severe Pulmonary Hypertension 50
• Severe obstructive lesions:
AS,PS, HOCM, Coarctation.
17
• Systemic Ventricular Dysfunction,
NYHA class III or IV
7

Cardiac Tests Performed Cardiac Tests Performed
Doppler echocardiographyDoppler echocardiography Stress testingStress testing

Routine chest radiography delivers 20 m.radsRoutine chest radiography delivers 20 m.rads Standard fluoroscopy delivers 1-2 rads/minStandard fluoroscopy delivers 1-2 rads/min Current recommendationCurrent recommendation
■ >5 rads: very low risk>5 rads: very low risk■ 5-10 rads: counseling for low risk5-10 rads: counseling for low risk■ 10-15 rads during 110-15 rads during 1stst 6 weeks: individual 6 weeks: individual■ >15 rads: termination pf pregnancy>15 rads: termination pf pregnancy
Cardiac Tests Performed Cardiac Tests Performed

Magnetic Resonance ImagingMagnetic Resonance Imaging
Pulmonary Artery Catheterization: Great help Pulmonary Artery Catheterization: Great help in managing high risk patient during in managing high risk patient during pregnancy, labor and deliverypregnancy, labor and delivery
Cardiac CatheterizationCardiac Catheterization■ Can be doneCan be done
Cardiac Tests Performed Cardiac Tests Performed

Pregnancy result in case of Pregnancy result in case of Cardiovascular Disorders Cardiovascular Disorders
miscarriagesmiscarriages Preterm labor and birthPreterm labor and birth IUGRIUGR Congenital heart lesions (4-16%)Congenital heart lesions (4-16%) Maternal mortality Maternal mortality

Maternal cardiac disease risk groupMaternal cardiac disease risk group Group I (mortality rate 1%)Group I (mortality rate 1%)
■ Corrected tetralogy FallotCorrected tetralogy Fallot■ Pulmonic/tricuspid diseasePulmonic/tricuspid disease■ Mitral stenosisMitral stenosis■ Patern ductus arteriosusPatern ductus arteriosus■ Ventricular septal defectVentricular septal defect■ Atrial septal defectAtrial septal defect
Group II (mortality rate 5-15%)Group II (mortality rate 5-15%)■ Mitral stenosis with atrial fibrillationMitral stenosis with atrial fibrillation■ Uncorrected tetralogy FallotUncorrected tetralogy Fallot■ Aortic coarctation (uncomplicated)Aortic coarctation (uncomplicated)■ Marfan syndrome with normal aortaMarfan syndrome with normal aorta
Group III (mortality rate 20-50%)Group III (mortality rate 20-50%)■ Aortic coarctation (complicated)Aortic coarctation (complicated)■ Myocardial infarctionMyocardial infarction■ Marfan syndrome with aortic involvementMarfan syndrome with aortic involvement■ Pulmonary hypertensionPulmonary hypertension

NEW YORK HEART ASSOCIATION FUNCTIONAL NEW YORK HEART ASSOCIATION FUNCTIONAL
CLASSIFICATION (NYHA) OF HEART DISEASE CLASSIFICATION (NYHA) OF HEART DISEASE
CLASS I CLASS I No signs or symptoms of cardiac No signs or symptoms of cardiac decompensation. decompensation.
CLASS II CLASS II No symptoms at rest but minor No symptoms at rest but minor limitation of physical activity.limitation of physical activity.
CLASS III CLASS III No symptoms at rest but marked No symptoms at rest but marked limitation of physical activity. limitation of physical activity.
CLASS IV CLASS IV Symptoms present at rest increses Symptoms present at rest increses discomfort with any kind of physical discomfort with any kind of physical activity. activity.

What is the prognosis for a woman What is the prognosis for a woman with a cardiac disease depending on with a cardiac disease depending on the NYHA risk group classification? the NYHA risk group classification?

Prognosis depending on the functional status
In general, women in NYHA classes I and II lesions usually do well during pregnancy and have a favorable prognosis with a mortality rate of <1%. Patients in NYHA classes III and IV may have a mortality rate of 5% to 15%. These patientsshould be advised against becoming pregnant.

What are the clinical features in a normal What are the clinical features in a normal pregnancy which can mimic a cardiac disease ? pregnancy which can mimic a cardiac disease ?

The clinical features in a normal pregnancy which can mimic a cardiac disease are
1. Dyspnea - due to hyperventilation, elevated diaphragm..
2. Pedal Edema 3. Cardiac impulse- Diffused and shifted laterally
from elevated diaphragm.4. Jugular veins may be distended and JVP raised.

What are the indications for Termination of What are the indications for Termination of
pregnancy?pregnancy?

The indications for Termination of pregnancy:
Because of high maternal risks, MTP is indicated
in:
1.Eisenmenger’s syndrome.
2.Marfan’s syndrome with aortic involvement
3.Pulmonary hypertension.
4.Coarctation of aorta with valvular involvement. •Termination should be done before 12 weeks of
pregnancy.

Contraindications to pregnancyContraindications to pregnancy
Pulmonary hypertensionPulmonary hypertension Shunt lesions associated with Eisenmenger Shunt lesions associated with Eisenmenger
syndromesyndrome Complex cyanotic congenital heart diseaseComplex cyanotic congenital heart disease Aortic coarctation complicated by artic Aortic coarctation complicated by artic
dissectiondissection Poor ventricular functionPoor ventricular function Marfan syndrome with marked aortic Marfan syndrome with marked aortic
dilatationdilatation

Associated Cardiovascular Disorders Associated Cardiovascular Disorders
I I Congenital cardiac diseaseCongenital cardiac disease■ Septal defectsSeptal defects
Atrial septal defect (ASD)Atrial septal defect (ASD) Ventricular septal defect (VSD)Ventricular septal defect (VSD) Patent ductus arteriosus (PDA)Patent ductus arteriosus (PDA)
■ Acyanotic lesionsAcyanotic lesions Coarctation of aortaCoarctation of aorta
■ Cyanotic lesionsCyanotic lesions Tetralogy of FallotTetralogy of Fallot

Associated Cardiovascular Disorders cont Associated Cardiovascular Disorders cont
Acquired cardiac diseaseAcquired cardiac disease■ Mitral valve stenosisMitral valve stenosis■ Aortic stenosisAortic stenosis■ Ischemic heart diseaseIschemic heart disease
Myocardial infarction (MI) Myocardial infarction (MI)
■ Other cardiac diseasesOther cardiac diseases (PPCM) Pulmonary hypertension(PPCM) Pulmonary hypertension Marfan syndromeMarfan syndrome Infective endocarditisInfective endocarditis Eisenmenger syndromeEisenmenger syndrome Valve replacementValve replacement Peripartum cardiomyopathyPeripartum cardiomyopathy

Arial septal defectArial septal defect
Left-to-right shuntLeft-to-right shunt Undetected because Undetected because
woman is asymptomaticwoman is asymptomatic Uncomplicated pregnancyUncomplicated pregnancy Right-side heart failure or Right-side heart failure or
arrhythmia as a result of arrhythmia as a result of increased blood volumeincreased blood volume


Ventricular septal defectVentricular septal defect Left-to-right shuntLeft-to-right shunt Diagnosed and corrected during Diagnosed and corrected during
infancy and childhood, not infancy and childhood, not common in pregnancycommon in pregnancy
Not complicated pregnancyNot complicated pregnancy Risk for: arrhythmias, heart failure, Risk for: arrhythmias, heart failure,
pulmonary hypertensionpulmonary hypertension
ManagementManagement■ Rest Rest ■ decrease of decrease of
physical physical activityactivity
■ anticoagulantsanticoagulants

Patent ductus arteriosusPatent ductus arteriosus Left-to-right shuntLeft-to-right shunt Diagnosed and corrected during Diagnosed and corrected during
infancyinfancy Possible complicationsPossible complications
■ arrhythmias, arrhythmias, ■ heart failure, heart failure, ■ pulmonary hypertensionpulmonary hypertension■ EndocarditisEndocarditis■ Pulmonary emboliPulmonary emboli
ManagementManagement■ Rest Rest ■ decrease of physical activitydecrease of physical activity■ anticoagulantsanticoagulants

Congenital Heart DiseaseCongenital Heart Disease
Acyanotic LesionsAcyanotic Lesions

Coarctation of the aortaCoarctation of the aorta Pregnancy safe for mother with Pregnancy safe for mother with
uncomplicated coarctationuncomplicated coarctation ComplicationsComplications
■ HypertensionHypertension■ Congestive heart failureCongestive heart failure■ Aortic ruptureAortic rupture
ManagementManagement■ RestRest■ Antihypertensive medications (beta-blockers)Antihypertensive medications (beta-blockers)■ Vaginal birth with epidural anesthesia and Vaginal birth with epidural anesthesia and
shortening of the II stage (vacuum- or shortening of the II stage (vacuum- or forceps assisted)forceps assisted)
■ Antibiotic prophylaxisAntibiotic prophylaxis

Congenital Heart DiseaseCongenital Heart Disease
Cyanotic LesionsCyanotic Lesions

Tetralogy of FallotTetralogy of Fallot 1. Ventricular septal defect1. Ventricular septal defect.. 2. 2. overriding aortaoverriding aorta 3. 3. right ventricular hypertrophyright ventricular hypertrophy 4. pulmonary 4. pulmonary stenosisstenosis Right-to-left shuntRight-to-left shunt Corrected at childhoodCorrected at childhood Management Management
■ AnticoagulantAnticoagulant■ OxygenOxygen■ hemodynamic monitoringhemodynamic monitoring

Acquired Heart DiseasesAcquired Heart Diseases

Mitral StenosisMitral Stenosis
The pressure gradient across the narrow valve The pressure gradient across the narrow valve increases secondary to the increases secondary to the increased heart rateincreased heart rate and and blood volumeblood volume
Left atrial pressure increases, back pressure into the Left atrial pressure increases, back pressure into the lungs causes lungs causes breathlessnessbreathlessness, , swelling in theswelling in the legslegs and may lead to and may lead to atrial arrhythmiasatrial arrhythmias. .
Stretching of the atrium can also occur causing Stretching of the atrium can also occur causing palpitations and arrhythmiapalpitations and arrhythmia..

Mitral StenosisMitral Stenosis
Maternal mortality rate in classes III and IV Maternal mortality rate in classes III and IV ■ 5 %without arterial fibrillation5 %without arterial fibrillation■ 15% with arterial fibrillation15% with arterial fibrillation
There is marked increase in the following There is marked increase in the following issues regarding the fetus issues regarding the fetus ■ Rate of prematurityRate of prematurity■ Fetal growth retardationFetal growth retardation■ Low neonatal birth weightLow neonatal birth weight

Mitral StenosisMitral Stenosis Therapeutic approach is:Therapeutic approach is:
■ to reduce the heart rate to reduce the heart rate ■ and decrease left atrial pressureand decrease left atrial pressure
Restrict physical activityRestrict physical activity Restrict salt intake Restrict salt intake diureticsdiuretics Beta blockersBeta blockers Digoxin (if patient is in a. fib)Digoxin (if patient is in a. fib) Calcium channel blockersCalcium channel blockers
if medical therapy is ineffective surgery if medical therapy is ineffective surgery may be necessary after 20 weeksmay be necessary after 20 weeks
■ Balloon valvuloplastyBalloon valvuloplasty■ Surgery (repair/replacement)Surgery (repair/replacement)

Mitral StenosisMitral Stenosis
Vaginal delivery can be permitted in most Vaginal delivery can be permitted in most patientspatients
Hemodynamic monitoring is recommended Hemodynamic monitoring is recommended (Swan) and should be continued several (Swan) and should be continued several hours following delivery hours following delivery

Aortic StenosisAortic Stenosis AS lead to obstruction to AS lead to obstruction to
left ventricular ejectionleft ventricular ejection Mild AS is usually tolerated Mild AS is usually tolerated Moderate to severe AS is Moderate to severe AS is
likely to be associated with likely to be associated with symptomatic deterioration symptomatic deterioration during pregnancyduring pregnancy
Women with valve area Women with valve area <1.0 should consider valve <1.0 should consider valve replacement prior to replacement prior to pregnancypregnancy

Aortic StenosisAortic Stenosis
Symptoms often develop in the 2nd and 3rd trimesterSymptoms often develop in the 2nd and 3rd trimester■ Exertional dyspneaExertional dyspnea■ Chest painChest pain■ SyncopeSyncope
Fetal effects includedFetal effects included■ Intrauterine growth retardationIntrauterine growth retardation■ Premature deliveryPremature delivery■ Reduced birth weightReduced birth weight■ Increase in cardiac defectsIncrease in cardiac defects

Ischemic Heart DiseaseIschemic Heart Disease MI is rare in childbearing womanMI is rare in childbearing woman Risk factors increaseRisk factors increase
■ AgeAge■ SmokingSmoking■ StressStress■ Cocaine useCocaine use■ HyperbilirubinemiaHyperbilirubinemia■ DMDM■ Family history of IHDFamily history of IHD■ HypertensionHypertension■ Oral contraceptivesOral contraceptives

Ischemic Heart DiseaseIschemic Heart Disease
MangementMangement■ OxygenOxygen■ AspirinAspirin■ Beta-blockersBeta-blockers■ NitratesNitrates■ HeparinHeparin■ Side-lying positionSide-lying position■ Vaginal birth is preferable with avoiding of maternal Vaginal birth is preferable with avoiding of maternal
pushing (vacuum- or forceps-assisted)pushing (vacuum- or forceps-assisted)■ Diuretic postpartumDiuretic postpartum

Other Heart DiseasesOther Heart Diseases

Primary Pulmonary HypertensionPrimary Pulmonary Hypertension Constriction of the arteriolar vessels in the Constriction of the arteriolar vessels in the
lung, leads to increase in the pulmonary lung, leads to increase in the pulmonary artery pressure right ventricular artery pressure right ventricular hypertension, hypertrophy, dilatation, right hypertension, hypertrophy, dilatation, right ventricular failure with tricuspid ventricular failure with tricuspid regurgitationregurgitation
Associated with high maternal mortality Associated with high maternal mortality estimated to be 50%, half of them occurs estimated to be 50%, half of them occurs a few hours to several days post partum a few hours to several days post partum usually related to sudden death or usually related to sudden death or progressive RV failure, although the exact progressive RV failure, although the exact cause of death is not clearcause of death is not clear
Deterioration usually occurs in the Deterioration usually occurs in the second/third trimestersecond/third trimester

Primary Pulmonary HypertensionPrimary Pulmonary Hypertension Symptoms may includeSymptoms may include
■ FatigueFatigue■ DyspneaDyspnea■ Chest painChest pain■ Edema and ascitesEdema and ascites■ SyncopeSyncope
Diagnostic testDiagnostic test■ Chest radiogramChest radiogram■ ECGECG■ EchoCGEchoCG■ Dopler studiesDopler studies

Primary Pulmonary HypertensionPrimary Pulmonary Hypertension
Fetal effects includeFetal effects include■ High incidence of prematurityHigh incidence of prematurity■ Fetal growth retardationFetal growth retardation■ Fetal lossFetal loss
Pregnancy should be discouraged in all Pregnancy should be discouraged in all patients with primary pulmonary HTNpatients with primary pulmonary HTN

Primary Pulmonary HypertensionPrimary Pulmonary Hypertension
For patients who chose to continue pregnancyFor patients who chose to continue pregnancy■ Nifedipin or prostacycline (for pulmonary Nifedipin or prostacycline (for pulmonary
vasodilatation)vasodilatation)■ AnticoagulantAnticoagulant■ Continuous hemodynamic monitoring during labor Continuous hemodynamic monitoring during labor
and delivery and delivery Antiembolic strockingAntiembolic strocking Side-lying positionSide-lying position Oxygen therapy Oxygen therapy Epidural analgesiaEpidural analgesia

Marfan SyndromeMarfan Syndrome Autosomal dominant genetic disorder Autosomal dominant genetic disorder
characterizedcharacterized■ weakness of the connective tissue, weakness of the connective tissue, ■ resulting in joint deformities, resulting in joint deformities, ■ ocular lens dislocation, ocular lens dislocation, ■ weakness of aortic wall and rootweakness of aortic wall and root
Mitral valve prolapse (90%)Mitral valve prolapse (90%) Aortic insufficiency (25%) risk of Aortic insufficiency (25%) risk of
aortic dissection and rupturingaortic dissection and rupturing
Pregnancy in patients with Marfan poses 2 Pregnancy in patients with Marfan poses 2 problemsproblems
■ Cardiovascular complications of the motherCardiovascular complications of the mother■ Risk of having a child who inherits Marfan’s Risk of having a child who inherits Marfan’s
syndromesyndrome
Cardiovascular problemsCardiovascular problems■ Dilation of the ascending aorta, may lead to Dilation of the ascending aorta, may lead to
development of aortic regurgitation and heart development of aortic regurgitation and heart failurefailure
■ Proximal and distal dissections of the aorta with Proximal and distal dissections of the aorta with possible involvement of the coronariespossible involvement of the coronaries

Marfan’s SyndromeMarfan’s Syndrome Obstetrical complications Obstetrical complications
■ Cervical incompetenceCervical incompetence■ Abnormal placental location (previa)Abnormal placental location (previa)■ Postpartum hemorrhagePostpartum hemorrhage
Preconception counselingPreconception counseling■ Patients with more than mild dilation of the aorta, or history of Patients with more than mild dilation of the aorta, or history of
aortic dissection should be advised against pregnancyaortic dissection should be advised against pregnancy■ Progressive dilation of the aorta during gestation may occur Progressive dilation of the aorta during gestation may occur
even with a normal-sized aortaeven with a normal-sized aorta Preconception echo evaluation allows for evaluation of the Preconception echo evaluation allows for evaluation of the
aortic root, CT, MRI.aortic root, CT, MRI. Periodic echocardiographic follow-up is recommendedPeriodic echocardiographic follow-up is recommended

Marfan’s SyndromeMarfan’s Syndrome
ManagementManagement■ Vigorous physical activity should be avoidedVigorous physical activity should be avoided■ Beta blockers (reduces the rate of aortic dilation)Beta blockers (reduces the rate of aortic dilation)■ If substantial dilation/dissection should occur, If substantial dilation/dissection should occur,
depending on the stage of pregnancydepending on the stage of pregnancy therapeutic abortion, therapeutic abortion, early delivery or early delivery or surgical intervention should be consideredsurgical intervention should be considered

Infective endocarditisInfective endocarditis
Inflammation of endocardiumInflammation of endocardium Cause: microorganismsCause: microorganisms Clinical manifestation: Clinical manifestation:
■ incompetence of heart valvesincompetence of heart valves■ Congestive heart failureCongestive heart failure■ Cerebral emboliCerebral emboli
TreatmentTreatment■ AntibioticsAntibiotics

Eisenmenger SyndromeEisenmenger Syndrome
Right-to-left or bidirectional shunting at Right-to-left or bidirectional shunting at atrial or ventricular level and combined atrial or ventricular level and combined with elevated pulmonary vascular with elevated pulmonary vascular resistanceresistance
High risk of maternal (30-50%) and fetal High risk of maternal (30-50%) and fetal (50%) morbidity and mortality(50%) morbidity and mortality
Pregnancy is contraindicated Pregnancy is contraindicated (contraception or termination of (contraception or termination of pregnancy)pregnancy)
Death usually (75%) occurs between the Death usually (75%) occurs between the first few days and weeks after delivery, first few days and weeks after delivery, but the cause is unclearbut the cause is unclear

Eisenmenger SyndromeEisenmenger Syndrome
Patients should be monitored closely for any signs of Patients should be monitored closely for any signs of deteriorationdeterioration
Early elective hospitalization is recommendedEarly elective hospitalization is recommended Activity is strictly limitedActivity is strictly limited Hemodynamic monitoring is requiredHemodynamic monitoring is required Anticoagulant???Anticoagulant??? Prophylaxis of hypovolemiaProphylaxis of hypovolemia OxygenOxygen Epidural analgesiaEpidural analgesia

CardiomyopathyCardiomyopathy
Cardiomyopathies are diseases of the heart are diseases of the heart muscle itself. People with cardiomyopathies -- muscle itself. People with cardiomyopathies -- sometimes called an enlarged heart -- have sometimes called an enlarged heart -- have hearts that are abnormally enlarged, hearts that are abnormally enlarged, thickened, and/or stiffened. As a result, the thickened, and/or stiffened. As a result, the heart's ability to pump blood is weakened. heart's ability to pump blood is weakened. Without treatment, cardiomyopathies worsen Without treatment, cardiomyopathies worsen over time and often lead to heart failure and over time and often lead to heart failure and abnormal heart rhythms.abnormal heart rhythms.

Hypertrophic CardiomyopathyHypertrophic Cardiomyopathy Most cases have favorable outcomesMost cases have favorable outcomes Symptoms may worsen, especially in patients who Symptoms may worsen, especially in patients who
were already symptomaticwere already symptomatic■ Increased SOBIncreased SOB■ FatigueFatigue■ Chest painChest pain■ SyncopeSyncope
The risk of the fetus of inheriting the disease is as The risk of the fetus of inheriting the disease is as high as 50%high as 50%

OTHER TYPES ARE:OTHER TYPES ARE:
Dilated cardimyopathyDilated cardimyopathy
Consticted myopathyConsticted myopathy

Prosthetic valves and Prosthetic valves and pregnancypregnancy
AnticoagulationAnticoagulation

Valve replacementValve replacement

10.What is warfarin fetal embryopathy ?10.What is warfarin fetal embryopathy ?

Warfarin use in first trimester can be teratogenic and can cause fetal embryopathy( 15 to 25 % ) which includes
· Nasal cartilage hypoplasia,
· Stippling of bones,
· IUGR and
·

Warfarin vs. HeparinWarfarin vs. HeparinWarfarinWarfarin
Crosses the placenta.Crosses the placenta. ↑↑early abortion, prematurity, early abortion, prematurity,
and and embryopathy embryopathy when used in when used in 11stst trimester (6 trimester (6thth–12–12thth weeks). weeks).
CNS & Eye abnormalities (2CNS & Eye abnormalities (2ndnd & 3& 3rdrd trimester). trimester).
Bleeding in the fetus Bleeding in the fetus (especially at delivery)(especially at delivery)■ Should be stopped before Should be stopped before
delivery.delivery.
HeparinHeparin
Does not cross the placentaDoes not cross the placenta No teratogenicityNo teratogenicity No fetal bleedingNo fetal bleeding
Twice daily SC injectionTwice daily SC injection Risk of osteoporosis Risk of osteoporosis
■ <2% symptomatic fractures.<2% symptomatic fractures.■ but 30% decrease in bone density.but 30% decrease in bone density.
Risk for thrombocytopeniaRisk for thrombocytopenia ↑↑ ↑↑ Risk of thrombosisRisk of thrombosis
“warfarin embryopathy”: Nasal hypoplasia, Bone epiphysis, optic atrophy, blindness, seizures. Overall risk around 5%. Decreases with the use of UFH in the first 3 months

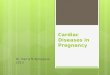
Dose-dependent Fetal Complications of warfarin in Dose-dependent Fetal Complications of warfarin in pregnant women with Mechanical Heart Valvespregnant women with Mechanical Heart Valves
Outcome of pregnanciesOutcome of pregnanciesWARFARIN DOSE (MG)
Healthy fetuses Fetal complications
Total
≤ 5 28• 27 FT•1 PR
5/33 (15%)• 4 SA
• 1 GR•0 WE (0%)
33
> 5 3 FT 22/25 (88%)• 2 WE (9%)• 18 SA• 1 SB• 1 VSD
25
Total 31 27 58
FT = full term, GR = growth retardation; PR = preterm; SA = spontaneous abortion; SB = still birth; WE = warfarin embryopathy
.

Unfractionated HeparinUnfractionated Heparin 4X higher incidence of Thrombo-embolism 4X higher incidence of Thrombo-embolism
during pregnancy than oral anticoagulantsduring pregnancy than oral anticoagulants ..
1.1. Hanania G, et al. pregnancy in patients with valvular prosthesis-Hanania G, et al. pregnancy in patients with valvular prosthesis-retrospective cooperative study in France (155 Cases). J Arch Mal Coeur retrospective cooperative study in France (155 Cases). J Arch Mal Coeur Vaiss 1994;87:429-437Vaiss 1994;87:429-437..
Failure of adjusted dose SC heparin to prevent Failure of adjusted dose SC heparin to prevent thrombo-embolic phenomena in pregnant thrombo-embolic phenomena in pregnant women women (n= 40)(n= 40) with mechanical valve prosthesis. with mechanical valve prosthesis.
■ Adjusted doses of SC heparin does not improve Adjusted doses of SC heparin does not improve fetal outcome and increases maternal mortalityfetal outcome and increases maternal mortality ..
2. Salazare E, et al. Filure of adjusted dose heparin to prevent thromboembolisc phenomena in pregnant patients with mechanical cardiac valve prosthesis. J Am Coll Cardiol 1996;1698-1703.

Frequency of fetal and maternal complications according to the Frequency of fetal and maternal complications according to the anticoagulation regimen used during pregnancy in women with anticoagulation regimen used during pregnancy in women with
mechanical heart valve prosthesis. mechanical heart valve prosthesis. Adapted from Chen et al. (976 women, 1234 pregnancies)Adapted from Chen et al. (976 women, 1234 pregnancies)
Anticoagulation regimenEmbryopath
y (%)
Spontaneous abortion
(%)
Thrombo-embolic
complications (%)
Maternal death (%)
Vitamin K antagonist throughout pregnancy
6.4 25 31/788 (3.9%) 10/561 (1.8%)
Heparin throughout pregnancy
0 24 7/21 (33%) 3/20 (15%)
• Low dose 0 20 60 40
• Adjusted dose 0 25 25 6.7
Heparin during first trimester, then vitamin K antagonists (with or without heparin before delivery)
3.4 25 21/229 (9.2%) 7/167 (4.2%)

Low-dose ASALow-dose ASA
The additional use of low-dose aspirin should The additional use of low-dose aspirin should be considered, particularly inbe considered, particularly in
Women with high-risk valves.Women with high-risk valves. Patients with cyanosis.Patients with cyanosis. Patients with intra-cardiac shunts.Patients with intra-cardiac shunts. Women with previous TIAs and/or strokes. Women with previous TIAs and/or strokes. And women with atrial fibrillation. And women with atrial fibrillation.

LMWHLMWH Do not cross the placenta. Do not cross the placenta. Do not require frequent PTT monitoringDo not require frequent PTT monitoring and have a longer half-life than UFH. and have a longer half-life than UFH. The data to support the use of LMWH, however, is not yet The data to support the use of LMWH, however, is not yet
available. available. A successful use of LMWH was reported in small number of A successful use of LMWH was reported in small number of
patients and more information is required before LMWH can patients and more information is required before LMWH can be recommended for anticoagulation in a patient with a be recommended for anticoagulation in a patient with a prosthetic valve during pregnancyprosthetic valve during pregnancy11..
Recently, two cases of LMWH treatment failure resulting in Recently, two cases of LMWH treatment failure resulting in thrombosed prosthetic heart valves were reported in 2000thrombosed prosthetic heart valves were reported in 200022..
LMWH should not be recommended at the present time in LMWH should not be recommended at the present time in patients with heart valve prostheses during pregnancy.patients with heart valve prostheses during pregnancy.

Mechanical Valves and Mechanical Valves and Anticoagulation during PregnancyAnticoagulation during Pregnancy Heparin may not prevent valve thrombosis: ?how Heparin may not prevent valve thrombosis: ?how
much ?route.much ?route. Adequate anticoagulation difficult.Adequate anticoagulation difficult. Heparin can produce osteoporosis.Heparin can produce osteoporosis. Little data regarding LMWH.Little data regarding LMWH. Warfarin can cause embryopathy.Warfarin can cause embryopathy. Baby ASA safe + probably beneficial.Baby ASA safe + probably beneficial.1-4% mortality in pregnant women with mechanical 1-4% mortality in pregnant women with mechanical
valve prosthesis, Whatever the anticoagulation valve prosthesis, Whatever the anticoagulation regimen. regimen.
No Ideal Solution

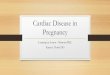
Suggested algorithm for the management of Suggested algorithm for the management of anticoagulation in patients with mechanical anticoagulation in patients with mechanical
prosthetic heart valves during pregnancyprosthetic heart valves during pregnancy
Pregnancy in patients with prosthetic heart valves
Higher riskFirst-generation prosthesis
In the mitral position
Lower riskSecond-generation prosthesis
And any mechanical prosthesis in the aortic position
Coumadin to INR 3.0-4.5 for 36
weeks followed by IV heparin to
aPTT of > 2.5-3.5
SC or IV (better) heparin-(aPTT 2.5-3.5)
for 12 weeks
Coumadin (INR 3.0-4.5) to 36th week
IV heparin(aPTT > 2.5)
SC Heparin(aPTT 2.0-3.0) for 12 weeks
Coumadin (INR 2.5-3.0) to 36th week
SC Heparin(aPTT 2.0-3.0)
SC heparin(aPTT 2.0-3.0)
Throughout pregnancy
1-4% mortality in pregnant women with mechanical valve prosthesis, Whatever the anticoagulation regimen.

Mode of deliveryMode of deliveryVaginal deliveryVaginal delivery
With facilitated second stage With facilitated second stage is preferred & safe is preferred & safe
Invasive hemodynamic Invasive hemodynamic monitoring only in:monitoring only in:
■ Severe valve stenosis Severe valve stenosis ■ Recent heart failure.Recent heart failure. ■ Severe cyanotic heart diseaseSevere cyanotic heart disease■ Pulmonary HTN.Pulmonary HTN.
Cesarean sectionCesarean section Avoids physical stress of laborAvoids physical stress of labor but but notnot free from hemodynamic free from hemodynamic
consequences.consequences. Indications in CHD only for:Indications in CHD only for:
■ Obstetric reasons.Obstetric reasons.■ Therapeutic anticoagulation with Therapeutic anticoagulation with
coumadin at onset pf labor.coumadin at onset pf labor.■ Pulmonary hypertension.Pulmonary hypertension.■ Unstable aortic lesion with risk of Unstable aortic lesion with risk of
dissection.dissection.■ Severe obstructive lesionsSevere obstructive lesionsBreast-feeding
• Can be encouraged in women taking anticoagulants. • Heparin is not secreted in
breast milk • and the amount of warfarin is
low.

Endocarditis prophylaxisEndocarditis prophylaxis Antibiotic prophylaxis at the time of delivery is not recommended for Antibiotic prophylaxis at the time of delivery is not recommended for
patients expected to have uncomplicated vaginal delivery or patients expected to have uncomplicated vaginal delivery or cesarian section, unless clinically overt infection is present cesarian section, unless clinically overt infection is present 1,21,2
Patients at Patients at high risk for endocarditishigh risk for endocarditis may receive antibiotics at the may receive antibiotics at the discretion of their physiciandiscretion of their physician22::
■ Those with prosthetic heart valves.Those with prosthetic heart valves.■ Previous IE.Previous IE.
Antibiotics for prophylaxis against endocarditis
Ampicillin No major adverse effects
Given along with gentamicin to high-risk patients to prevent IE
B 2 gr IV or IM within 30 min before delivery.
And 1 gr PO, IV or IM 6 hrs later.
Vancomycine No major adverse effects
Given along with gentamicin to high-risk patients to prevent IE
Cm I gr IV over 1-2 hours, given 30 min before delivery.
Gentamicin No major adverse effects
Given along with Ampicilline or Gentamicin to high-risk patients to prevent IE
C 1.5 mg/kg within 30 min before delivery (max 120 mg)

Peripartum CardiomyopathyPeripartum Cardiomyopathy A form of dilated CMP with LV systolic dysfunction that results A form of dilated CMP with LV systolic dysfunction that results
in the signs and symptoms of heart failurein the signs and symptoms of heart failure CriteriaCriteria
■ Development in last month of pregnancy or the first 5 months after Development in last month of pregnancy or the first 5 months after deliverydelivery
■ Absence of heart disease prior to last month of pregnancyAbsence of heart disease prior to last month of pregnancy■ Absence of identifiable cause of heart failureAbsence of identifiable cause of heart failure■ LV systolic dysfunctionLV systolic dysfunction
Etiology is unknownEtiology is unknown TheoriesTheories
■ Genetic predispositionGenetic predisposition■ AutoimmunityAutoimmunity■ Viral infectionViral infection

Peripartum CardiomyopathyPeripartum Cardiomyopathy
Associated risk factors:Associated risk factors:■ Age - over 35Age - over 35■ twin pregnancytwin pregnancy■ gestational hypertensiongestational hypertension■ MultiparityMultiparity■ African-american raceAfrican-american race■ use of tocolytic therapyuse of tocolytic therapy
Motality rate 25-50%Motality rate 25-50%

Peripartum CardiomyopathyPeripartum Cardiomyopathy
Clinical findingsClinical findings■ Left ventricular failureLeft ventricular failure
DyspneaDyspnea FatigueFatigue EdemaEdema Enlarged heartEnlarged heart TachycardiaTachycardia arrhythmiasarrhythmias

Peripartum CardiomyopathyPeripartum Cardiomyopathy
clinical course varies clinical course varies ■ 50-60% of patients demonstrate complete recovery 50-60% of patients demonstrate complete recovery
within the first 6 monthswithin the first 6 months■ The rest of the patients demonstrate either further clinical The rest of the patients demonstrate either further clinical
deterioration, leading to cardiac transplant or premature deterioration, leading to cardiac transplant or premature death, or persistent LV dysfunction and chronic heart death, or persistent LV dysfunction and chronic heart failurefailure
■ No agreement on recommendation for future No agreement on recommendation for future pregnanciespregnancies
■ Pregnancy contraindicated Pregnancy contraindicated Persistent cardiomegalyPersistent cardiomegaly Cardiac dysfunctionCardiac dysfunction

Peripartum CardiomyopathyPeripartum Cardiomyopathy
ManagementManagement■ Acute heart failure treatment with O2, Acute heart failure treatment with O2,
diuretics, digoxin and vasodilators diuretics, digoxin and vasodilators (hydralazine is safe)(hydralazine is safe)
■ Because of the increased incidence of Because of the increased incidence of thromboembolic events, anticoagulation thromboembolic events, anticoagulation therapy is recommendedtherapy is recommended

11. What are the risk factors for cardiac failure 11. What are the risk factors for cardiac failure during pregnancy ?during pregnancy ?

Risk factors for cardiac failure during pregnancy
Infection Anemia Obesity Hypertension Hyperthyroidism Multiple pregnancy

Pulmonary hypertension as a risk of Pulmonary hypertension as a risk of adverse outcomeadverse outcome
Pulmonary hypertensionPulmonary hypertension
(Eisenmenger Syndrome)(Eisenmenger Syndrome)Increased rate of adverse maternal eventsIncreased rate of adverse maternal events
Up to 30-40% (Up to 30-40% (↑ PVR)↑ PVR)
When systolic PAP > 75% systemic pressure
↑ ↑ intravascular volume intravascular volume HF HF (CO limited by Pulmonary vascular disease and Ventricular dysfunction)(CO limited by Pulmonary vascular disease and Ventricular dysfunction)
↓ ↓ SVR (after 1SVR (after 1stst trimester) trimester) ↑↑R-L ShuntR-L Shunt CyanosisCyanosis
Exacerbated during labor and deliveryExacerbated during labor and delivery
Bed rest (2Bed rest (2ndnd trimester), O2 (if helpful), ? Anticoagulation, trimester), O2 (if helpful), ? Anticoagulation, Cesarian section, invasive monitoring, early ambulation Cesarian section, invasive monitoring, early ambulation

Care managementCare management
Preconceptual councellingPreconceptual councelling■ Peripartum riskPeripartum risk
PregnancyPregnancy■ Decisions after evaluation riskDecisions after evaluation risk
If possible – multidisciplinary approch If possible – multidisciplinary approch (cardiologist, perinsatologist, (cardiologist, perinsatologist, anesthesiologist, ginecologist)anesthesiologist, ginecologist)

AssessmentAssessment
InterviewInterview■ Personal medical historyPersonal medical history■ Heart disease (congenital, streptococcal infections, rheumatic Heart disease (congenital, streptococcal infections, rheumatic
fever, valvular disease, endocarditis, angina, MI)fever, valvular disease, endocarditis, angina, MI)■ Factors increase stress of the heart (anemia, infection, edema)Factors increase stress of the heart (anemia, infection, edema)■ Review cardiovascular and pulmonary systemReview cardiovascular and pulmonary system
Chest pain, edema on face, hand, feet, hypertension, heart Chest pain, edema on face, hand, feet, hypertension, heart murmur, palpitation,dyspnea, diaphoesis, pallor, syncopemurmur, palpitation,dyspnea, diaphoesis, pallor, syncope
Cough, hemoptysis, shortness of breath, Cough, hemoptysis, shortness of breath, ■ MedicationMedication■ Emotional status (depression, anxiety, fear of morbidity and Emotional status (depression, anxiety, fear of morbidity and
mortality for herself and featus) mortality for herself and featus)

Assessment Assessment ExaminationExamination
■ Vital signVital sign■ Oxygen saturation levelOxygen saturation level■ Pattern of edemaPattern of edema■ Discomphort of pregnancyDiscomphort of pregnancy■ Weight gainWeight gain■ Sign of potential cardiac decompensationSign of potential cardiac decompensation

Sign of potential cardiac Sign of potential cardiac decompensationdecompensation
Subjective symptomsSubjective symptoms■ Increasing fatigue or difficulty of Increasing fatigue or difficulty of
breathing or both with usual activitiesbreathing or both with usual activities■ Feeling of smotheringFeeling of smothering■ Frequent coughFrequent cough■ Palpitations; feeling that her heart is Palpitations; feeling that her heart is
racingracing■ Swelling of face, feet, legs, fingersSwelling of face, feet, legs, fingers

Conti…….Conti……. Objective signsObjective signs
■ Irregular weak, rapid pulse (more 100b/m)Irregular weak, rapid pulse (more 100b/m)■ Progressive generalised edemaProgressive generalised edema■ Cracles at the base of lungsafter 2 Cracles at the base of lungsafter 2
inspirations and exhalationsinspirations and exhalations■ Orthopnea; increasing dyspneaOrthopnea; increasing dyspnea■ Rapid respirations (more 25 b/m)Rapid respirations (more 25 b/m)■ Moist, frequent coughMoist, frequent cough■ Increasing fatiqueIncreasing fatique■ Cyanosis of lips and nail bedsCyanosis of lips and nail beds

AssessmentAssessment
LabLab■ UrinalisisUrinalisis■ CBCCBC■ Blood chemistryBlood chemistry■ ECGECG■ EchoCGEchoCG■ Pulse oximetryPulse oximetry■ Chest filmChest film■ Fetal ultrasoundFetal ultrasound■ NST NST

Antepartum careAntepartum care Critical period 28-32 weeks – hemodinamic Critical period 28-32 weeks – hemodinamic
changes reach their maximumchanges reach their maximum Reduce emotional stress, hypertension, anemia, Reduce emotional stress, hypertension, anemia,
hyperthyroidism, obesityhyperthyroidism, obesity Class I and II Class I and II
■ 8-10 h of sleeping + 30 min naps after eating8-10 h of sleeping + 30 min naps after eating■ Activities: housework, shopping, exercise limitedActivities: housework, shopping, exercise limited
Class IIClass II■ Avoid any activities that causes even minor signs of Avoid any activities that causes even minor signs of
cardiac decompensationcardiac decompensation■ Admit to the hospital near termAdmit to the hospital near term
Class III, IVClass III, IV■ Bed rest at the hospital Bed rest at the hospital

Antepartum careAntepartum care Treatment of infections of GI, UT, RespiratoryTreatment of infections of GI, UT, Respiratory Adequate nutrition (folic acid, protein, fluid, fiber)Adequate nutrition (folic acid, protein, fluid, fiber) Medication:Medication:
■ anticoagulant – anticoagulant – heparin (large molecule does not cross the placenta)heparin (large molecule does not cross the placenta)
● Recurrent vein thrombosisRecurrent vein thrombosis● Pulmonary embolusPulmonary embolus● rheumatic heart diseaserheumatic heart disease● Prostetic valvesProstetic valves● Cyanotic congenital heart defectsCyanotic congenital heart defects
Monitiring clotting factors (blood test)Monitiring clotting factors (blood test) Avoid food high in vit K (raw, dark green and leafy Avoid food high in vit K (raw, dark green and leafy
vegetablesvegetables Folic acidFolic acid

Antepartum careAntepartum care Digoxin: crosses placentaDigoxin: crosses placenta Procainamide: crosses placenta, no known teratogenic Procainamide: crosses placenta, no known teratogenic
effectseffects Verapamil: crosses placenta, can produce maternal Verapamil: crosses placenta, can produce maternal
hypotensionhypotension Propranolol: crosses placenta, no known teratogenic Propranolol: crosses placenta, no known teratogenic
effects, associated with fetak bradicardia, IUGR, preterm effects, associated with fetak bradicardia, IUGR, preterm labour, neonatal respiratory depressionlabour, neonatal respiratory depression
Warfarin: crosses placenta, fetal anomalies, and Warfarin: crosses placenta, fetal anomalies, and hemorrhage, congenital malformation, preterm birth, hemorrhage, congenital malformation, preterm birth, stillbirthstillbirth
Furosemide: crosses placenta, no known teratogenic Furosemide: crosses placenta, no known teratogenic effects, thiazides: crosses placenta, neonatal jaudice, effects, thiazides: crosses placenta, neonatal jaudice, thrombocitopenia, anemiathrombocitopenia, anemia

Conti…..Conti…..
Lidocaine: crosses placenta, safe as long as Lidocaine: crosses placenta, safe as long as toxic leves avoidedtoxic leves avoided
Quinidine: crosses placenta, no known Quinidine: crosses placenta, no known teratogenic effects, neonatal thrombocytopeniateratogenic effects, neonatal thrombocytopenia
Nifedipine: crosses placenta, maternal Nifedipine: crosses placenta, maternal hypotensionhypotension
Diazoxide: crosses placenta, hyperglycemia, Diazoxide: crosses placenta, hyperglycemia, potential relaxant of uterine smooth musclepotential relaxant of uterine smooth muscle
Sodium nitroprusside: crosses placenta, only in Sodium nitroprusside: crosses placenta, only in critical care unitcritical care unit

Antepartum careAntepartum care
Heart surgeryHeart surgery■ Ideal scenario – before pregnancyIdeal scenario – before pregnancy■ If need present – early at the second trimIf need present – early at the second trim
Closed cardiac surgery – low riskClosed cardiac surgery – low risk Open heart surgery – high risk r/t with Open heart surgery – high risk r/t with
artificial circulation an temporary artificial circulation an temporary hypoxiahypoxia

Intrapartum Care Intrapartum Care Routine assessment of laboring womanRoutine assessment of laboring woman Assessment of cardiac decompensationAssessment of cardiac decompensation Arterial blood gasesArterial blood gases ECGECG BP, Ps, OxymetryBP, Ps, Oxymetry Position: elevated upper part of body or side-lyingPosition: elevated upper part of body or side-lying Management of discomfort: supportive care, epidural analgesiaManagement of discomfort: supportive care, epidural analgesia Preterm laboue: betaadrenergic agonist (ritodrine, terbutaline)Preterm laboue: betaadrenergic agonist (ritodrine, terbutaline) Labour induction (syntocinon)Labour induction (syntocinon) Cervical rippening (prostaglandins)Cervical rippening (prostaglandins) Vaginal birth Vaginal birth
■ in side-lying positionin side-lying position■ Oxygen maskOxygen mask■ EpisiotomyEpisiotomy■ vacuum extractionvacuum extraction■ ForcepsForceps
CS: risk r/t with dramatic fluid shifts, sustained hemodinamic changes CS: risk r/t with dramatic fluid shifts, sustained hemodinamic changes and increased blood loss and increased blood loss
Dilute oxytocin is indicated, ergot products are contraindicated Dilute oxytocin is indicated, ergot products are contraindicated

Postpartum CarePostpartum Care First 24-48 h are the most hemodinamically difficultFirst 24-48 h are the most hemodinamically difficult AssessmentAssessment
■ Vital signVital sign■ Oxygen saturation levelsOxygen saturation levels■ Lung and heart auscultationLung and heart auscultation■ EdemaEdema■ Character of bleeding, uterine toneCharacter of bleeding, uterine tone■ Fundal heightFundal height■ Urinary outputUrinary output■ PainPain
Activity rest patternActivity rest pattern Elevated the head of the bedElevated the head of the bed Family member helpFamily member help Brestfeeding is not contraindicatedBrestfeeding is not contraindicated

13. Which is the ideal contraceptive for women 13. Which is the ideal contraceptive for women with heart disease ?with heart disease ?

Contraception
1. OC pills are not ideal as they can cause thrombo embolism.
2. IUCD can cause infection- endocarditis.
3. Barrier contraceptives – Have high failure rates.
4. Progestin only pills or Long acting injectable progesterone are better
PILL - Desogestrel
INJECTABLES
a. Medroxy progesterone 150mg IM every 3 months.
b. Norethisterone.200 mg every 2 months
5. Sterilization is best.

Pregnancy and CHDPregnancy and CHDConclusionsConclusions
Most women with heart disease can have a Most women with heart disease can have a pregnancy proper care.pregnancy proper care.
Pre-pregnancy evaluation mandatory.Pre-pregnancy evaluation mandatory.
High-risk cases benefit from combined high-risk High-risk cases benefit from combined high-risk OB and cardiac care in the same center. OB and cardiac care in the same center.

THANKSTHANKS