Embed Size (px)
Citation preview

CARDIAC BIOMARKER
Dr Anurag YadavPostGraduate

BIOMARKER
“A biomarker is a substance used as an indicator of a biologic state”.
Accurate repeated measurements at reasonable cost
Must provide additional information
Should aid treatment

CARDIAC BIOMARKERS
Cardiac biomarkers are protein molecules released into the blood stream from damaged heart muscle
Since ECG…… inconclusive ….biomarkers !!!!!?????• myocardial injury
These biomarkers have a characteristic rise and fall pattern

CHARACTERISTICS
High cardiac specificity
Pharmacokinetics of cardiac biomarker
Easy diagnosis
Marker should play a designed role in the treatment and management of clinical subject

HISTORY OF CARDIAC BIOMARKERS
1954 - SGOT (AST)1955 - LDH 1960 - CPK 1972 - CPK isoforms by Electrophoresis 1975 - CK - MB by immunoinhibition 1975 - Myoglobin 1985 - CK - MB Mass immunoassay 1989 - Troponin T 1992 - Troponin I

CLASSIFICATION OF CARDIAC BIOMARKERS
Biomarkers of myocardial injury• markers of myocardial necrosis• markers of myocardial ischemia
Biomarkers of haemodynamic stress
Inflammatory and prognostic Biomarkers

CLASSIFICATION OF
CARDIAC BIOMARKERS
ACCORDING TO VARIOUS STAGES DURING CARDIAC DISEASE PROCESS


BIOMARKERS OF MYOCARDIAL INJURY
Markers of myocardial necrosis• Creatine kinase – MB• Myoglobin • Cardiac troponinsMarkers of myocardial ischemia• Ischemia Modified Albumin (IMA)• Heart-type fatty acid binding protein (H-
FABP

Marker for inflammatio
nhsCRP sCD40L Homocystei
n
Marker for plaque
DestabilizationPAPP-A LP-PLA2
Marker for hemodynamic
stress
Natriuretic peptides• ANP• BNP• Pro-BNP• CNP• DNP

Time of increase
Peak Return to normal
CK-MB 4-8 h 12-24h 72-96h (3-4D)
LDH 2-5 D 10 D
Myoglobin 2-4 h 8-10h 24 h
cTnI 4-6 h 12 h 3-10 D
cTnT 4-6 h 12-48 h 7-10 D

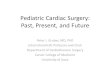
0 4 8 12 16 20 24 28 32 36 40 44 480
1
2
3
4
5
6
7
myoglobinCK-MBcTnTcTnI
COMPARISON OF CTN, CK-MB , MB
Time after onset of AMI (hours)
Χ up
per l
imit
of re
fere
nce
inte
rval

OTHER CARDIAC MARKERS
miRNA
IMA
MPO
MMP-9
FFAU
sCD40L
PIGF
PAPP-A
Choline

Stefan Blankenberg, MD; Renate Schnabel, MD; Edith Lubos, MD, et al., Myeloperoxidase Early Indicator of Acute Coronary Syndrome and Predictor of Future Cardiovascular Events 2005



TROPONIN ASSAYS
TropT (Roche Diagnostics, Germany) ; Trop I (Siemens Healthcare Diagnostics)
Troponin T • 99th percentile limits - 0.01 ng/mL • assay ranges - 0.01-25 ng/mL
(Troponin I) • 99th percentile limits -0.04 ng/mL • assay range -0.04-40 ng/mL
Reference limits based on the 99th percentile for a healthy population are 0.01 ng/mL (Troponin T) and 0.04 ng/mL (Troponin I)

Creatine kinase (CK) is a cytosolic enzyme
CK-MB

CK-MB :
it is a valuable tool for the diagnosis of MI because of its
relative high specificity for myocardial damage.
Rise : 4-6 hrs after onset of symptoms
Peak : 12 hrsReturn to normal : 24-36 hrs
Can be used to indicate early re-infarction if level normalizes and
then increases again.

CK-MBRelative Index = χ
100 Total CK
*The relative index allows the distinction between increased total CK due to myocardial damage and
that due to skeletal or neural damage.
*A relative index exceeding 3 is indicative of AMI

Small-size heme protein found in all tissues mainly assists in oxygen transport
• Earliest Rise: 1-4 hrs• Peak 6-9 hrs• Return to normal: 12 hrs
It is released from all damaged tissues
Its level rises more rapidly than cTn and CK-MB.
Released from damaged tissue within 1 hour
Normal value: 17.4-105.7 ng/ml
Timing:
Myoglobin

CONDITIONS FOR MYOGLOBIN INCREASE :
Acute myocardial infarction
Skeletal muscle damage, muscular dystrophy, inflammatory
myopathies
Renal failure, severe uremia
Shock and trauma

Clinical usefulness of myoglobin :*if myoglobin concentration remains within the reference range 8 hours after the onset of chest pain, AMI can be ruled out essentially.*because of its rapid clearance by the kidney, a persistently normal Mb concentration will rule out reinfarction in patient with recurrent chest pain after AMI*Rapid monitor of success of thrombolytic therapy
DRAWBACKS Due to poor specificity, myoglobin levels do not always
predict myocardial injury

0 4 8 12 16 20 24 28 32 36 40 44 480
1
2
3
4
5
6
7
myoglobinCK-MBcTnTcTnI
COMPARISON OF CTN, CK-MB , MB
Time after onset of AMI (hours)
Χ up
per l
imit
of re
fere
nce
inte
rval

Ischemia Modified Albumin (IMA)
A novel marker of ischemia, is produced when circulating serum albumin contacts ischemic heart tissues
IMA can be measured by the albumin cobalt binding (ACB) assay that is based on IMA's inability to bind to cobalt
Mechanism- due to structural change in the amino terminal end of albumin
IMA levels rise within 6 hours
remain elevated for 12 hours

Drawbacks IMA levels raised in non- cardiac ischemia
Modification to n- terminal end may also be induced by extracellular hypoxia, acidosis etc,
Conclusion FDA in 2010 has approved a multimarker
approach for using the combination of ECG, the cTnI, and the IMA levels achieving a sensitivity of 95% for ACS

Heart type fatty acid binding protein is a very stable low molecular weight (14-15kDa) in the cytoplasm of myocardial cells.
FABPs are involved in active fatty acid metabolism where it transports fatty acid from cell membrane to mitochondria for oxidation.
Small size of H-FABP facilitates rapid diffusion through interstitial space, appearing as early as 1-3 hrs after onset and peaking within 6hrs. It return to normal levels with in 12-24hrs.
Normal levels : 1.6 – 19 ng/ml
H-FABP

NATRIURETIC PEPTIDES
The natriuretic peptides (NP) are a group of structurally similar but genetically distinct peptides.
NPs are identified as regulatory diuretic-natriuretic substances responsible for salt and water homeostasis
Lowers blood pressure.

The NP family includes
ANP : -atrial natriuretic
peptide (28 a.a.)
N-terminal proANP (98 a.a.)
BNP : brain natriuretic
peptide (32 a.a.)
N-terminal proBNP (76 a.a.)
CNP : C-type natriuretic
peptide (22 and 53 a.a.)

Fig. Schematic representation of the ANP and BNP precursors with sequence numbering defining low-molecular-mass forms, N-terminal forms and high-molecular-mass precursors

OTHER CARDIAC MARKERS
miRNA
IMA
MPO
MMP-9
FFAU
sCD40L
PIGF
PAPP-A
Choline
hsCRP

Homocysteine
Intermediary amino acid formed by the conversion of methionine to cysteine
Moderate hyperhomocysteinemia occurs in 5-7% of the population
Recognized as an independent risk factor for the development of atherosclerotic vascular disease and venous thrombosis
Can result from genetic defects, drugs, vitamin deficiencies, or smoking

Homocysteine implicated directly in vascular injury including:• Intimal thickening• Disruption of elastic lamina• Smooth muscle hypertrophy• Platelet aggregation
Vascular injury induced by leukocyte recruitment, foam cell formation, and inhibition of NO synthesis
Homocysteine

Elevated levels appear to be an independent risk factor,
Screening recommended in patients with premature CV disease (or unexplained DVT) and absence of other risk factors
Treatment includes supplementation with folate, B6 and B12
Homocysteine

C-REACTIVE PROTEIN
CRP is an acute-phase protein produced by the liver
Pentameric structure consisting of five 23-kDa identical subunits
Plasma levels can increase rapidly to 10000x levels
High-sensitivity CRP (hs-CRP) assays


CRP previously known to be a marker of high risk in cardiovascular disease
More recent data may implicate CRP as an actual mediator of atherogenesis
Mechanism of CRP-mediated atherogenesis:
Once ligand-bound, CRP can:• Activate the classical compliment pathway• Stimulate phagocytosis• Bind to immunoglobulin receptors• Endothelial dysfunction via ↑ NO synthesis• ↑LDL deposition in plaque by CRP-stimulated macrophages



Clinical Uses • Screening for cardiovascular risk in
otherwise “healthy” individuals• Predictive value of CRP levels for disease
severity in pre-existing Coronary artery disease
Elevated levels predictive of• Long-term risk of first MI• Ischemic stroke

Limitations of CRP
Low specificityNo evidence that lowering CRP levels decreases CV risk• Industry and FDA staff guidelines 2005 had given clinical cut off
value as less than 1 mg/l as safe levels with hs-CRP tests
CRP Risk for CVD
Less than 1.0 mg/L Low1.0-2.9 mg/L IntermediateGreater than 3.0 mg/L High

miRNAs are appx. 20-25 nucleotide long non coding RNAs, that negatively regulate or inhibit gene expression by binding to sites in the untranslated regions of targeted messenger RNAs.
miRNA

miRNA are found to be involved in almost every biological process, from cellular differentiation and proliferation to cell death and apoptosis
Many different types of miRNA can be detected in circulating blood and these miRNA are present in remarkably stable form that even withstand repetitive freezing/thawing cycle and are protected against Rnases.
Thousands of miRNAs have been described in human to date which ehibits tissue specific pattern of expression.

miRNAs that regulates cardiovascular system can be divided into 4 groups :
1. miRNA regulating endothelium function and angiogenesis : miR126, miR17-92 cluster, miR130a, miR221, miR21
2. cardiac myocyte specific mRNA : miR208a
3. cardiac myocyte and skeletal muscle miRNA : miR1, miR133a, miR499
4. smooth muscle miRNAs :miR143, miR145
miRNAs hold promise as very specific and accurate marker of cardiac dysfunction.

CYTOKINES
Variety of interleukins (TNF, IL-1, IL-6, IL-8, IL-12, IL-18) are responsible for the atherosclerosis events.Regulated through the T cell-mediated and monocytes.
At present there are no standardized assay, reference interval studies.

MYELOPEROXIDASE (MPO)
Released from aggregated neutrophils.
Increased in CAD, ACS.
Is one of the best prognostic marker
At present no standardized assay method, nor consistency validation of the test.
Further, Type of specimen collect have shown variations.
Normal level: 640 pmol/L

Previously known as PAF ( platelet activating factor)
Synthesised from monocytes and lymphocytes.
Known to form lipid fragments which are most atherogenic which increase endothelial adhesion.
FDA approved for the assay.
Threshold for high risk: >200μg/L

It is an metaloprotimase.
Produced from the plaque which are prone to rupture.
Marker for the adverse CV events.
At present no standardized assay, consistency validation is present.
By two approach, median value for free PAPP-A is 0.18 mIU/L.

CHOLINE
Is released after stimulation by phospholipase D.
Touted as a test of prognosis in pt with chest discomfort.
Not available

UNBOUND FREE FATTY ACID (FFA-U)
Marker for ischemia.
Ischemia increase the small unbound fraction.
Studies revealed mixed result.
Not available

NOURIN
Small protein released by stressed myocytes.
Induce changes of inflammatory cytokines and attract neutrophils.
Preliminary studies have made attempt to validate its use.

30 a.a glycoprotein.
Prognostic marker in hemorrhagic and sepsis.
Recently, early biomarker for rule out the AMI with normal cTn.
The test method has to undergo many trials and head-to-head comparison with cTn.
COPEPTIN