Embed Size (px)
Citation preview

CARDIO-PULMONARYADAPATATION IN NEWBORN
DR CHANDAN C.KFellow in-
Neonatology,BAPUJI- CHI & RC,
DAVANGERE
Guide:DR .G.GURUPRASAD
Prof & HODDept. of
NeonatologyBapuji-CHI & RC

"Nature is neither lazy nor devoid of foresight. Having given the matter thought, she knows in advance that the lung of the fetus does not require the same arrangements of a perfected lung. She has therefore anastomosed the pulmonary artery with the aorta, and the left and right atria. . . .”
Galen, 2nd Century

Uniqueness of Fetal Circulation: The placenta provides for gas and meatbolite
exchange.
Rt and Lt ventricle exist in parallel circuit.
Three structures maintaining parallel circln.
1. Ductus venosus
2. Foramen ovale
3. Ductus arteriosus
Pulmonary vasculature are constricted diverting blood away from pul.circulation


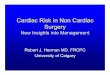
Ductus
arteriosusDuctus
Venosus
Foramen ovale

IVC(Po2-28mm Hg)
Umbilical
vein(Po2-35mm Hg)
Hepatic crcln(50%)
Right Atrium
Left Atrium
Left Ventricle
Ascndn aorta &upper body
,brain
DuctusVenosus
Foramen ovale

SVC(paO2-14mmHg)
Right Ventricle
Pulmonary artery
Descending Aorta
Lower part of body & umbilical
arteries
Lungs(5%)DuctusArteriosus
Right Atrium

Total fetal cardiac output,combined output of both ventricles, is 450ml/kg/min.
Right ventricular output is 1.3 times of left venticularoutput.
65% of descendin aorta blood returns to placenta ,35% perfuses fetal organs and tissues.

The Transitional circulation:
At birth ,the fetal circulation must adapt to extrauterine life as gas exchange is transferred from placenta to lungs.
.

Immediate changes in circln.
1. Pulmonary vascular resistance decreases due to mechanical expansion of lungs and increase in arterial Po2
2. Systemic vascular resistance increases due to removal of low resistance placental circulation.

3. a) As systemic vascular resistance > pulmonary resistance shunt through ductus arteriosus becomes L R.
b). High Po2 eventually closes ductus arteriosus over days and becomes ligamentum arteriosum.
4. Increase in volume of Lt atrium closes flap of foramen ovale functionally.
5. Removal of the placenta from the circulation also in results in closure of ductus venosus

6. The left ventricle must now deliver the entire systemic cardiac output(350/ml/kg/min),its wall thickness and mass begin to increase.
7. Right ventricle is now connected to low resistance pulmonary circulation and its mass and thickness begin to decrease.

The Neonatal Circulation
Some of these changes in circulation are instantenous with first breath wheareas others develop over a period of hours or weeks.

Pulmonary vascular resistance decreases immediately due to lung expansion and high Pao2.
Largest decline in PVR usually occurs within 2-3 days.
Over few weeks pumonary vascular resistance further decreases secondary to remodelling of pulmonary vasculature i.e thinning of vascular smooth muscle and recruitment of new vessels.
This decreaes influences timing of manifestation of CHD that are dependent on pulmonary and systemic vascular resistance.

Significant differences between neonatal and older infant circulation :
1. Right to left or left to right shunting may persist across foramen ovale.
2. In the presence of cardiopulmonary disease ductusarteriosus may allow lt to rt or rt to lt or bidirectional shunting

3. Pulmonary vasculature constricts more vigorously in response to hypoxia,hypercapnia and acidosis.
4. Wall thickness and muscle mass of both ventricles are almost equal.
5. Newborn have high cardiac output (350ml/kg/min),at 2th month (150ml/kg/min) .
6. High fetal hemoglobin may interfere with delivery of O2 to tissues.

Foramen ovale: Foramen ovale is usually functionally closed by 3rd
month of life.
It is possible to pass a probe through overlapping flaps in 15-25% of adults

Ductus arteriosus: DA represents persistence of terminal portion of sixth
branchial arch.
The aortic end of ductus is just distal to origin of subclavian artery and it enters pulmonary artery at its bifurcation.

Term infants functional closure has occurred in 50% by 24 hrs,90% by 48 hrs and in all by 72hrs.
Functional closure occurs by smooth muscle contraction.
Anantomical closure occurs over several days by neointimal thickening and loss of smooth muscle cells from inner muscle media.

In term infant found to have PDA the wall is deficient in both mucoid endothelial layer and muscular media.
Whereas PDA in preterm infant is usually normal structure.
Thus PDA persisting in term infant rarely closes spontaneously or pharmacologically.

Refrences:1. Nelson textbook of pediatrics,20e.
2. Manual of neontal care,7e/Cloherty et al.
3. Fetal and neonatal physiology/R.A.Polin,Wiliam Fox,
4. Care of newborn,8e/Meharban Singh.

Any neonate who fails hyperoxia test is likely to have heart disease involving ductal dependent systemic or pulmonary blood flow.
These should receive PGE1 infusion until anatomic definition can be accomplished.



NRP 2015: On October 15, 2015, the American Heart Association
(AHA) and American Academy of Pediatrics released new 2015 Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care of the Neonate. The guidelines serve as foundation for the Neonatal Resuscitation Program® (NRP®) 7th edition materials that will be released in Spring 2016 and must be in use by January 1, 2017.


The order of the 3 assessment questions has changed to (1) Term gestation (2) Good tone? and (3) Breathing or crying.
There is a new recommendation that delayed cord clamping for longer than 30 seconds is reasonable for both term and preterm infants who do not require resuscitation at birth.

If an infant is born through meconium-stained amniotic fluid and presents with poor muscle tone and inadequate breathing efforts, the infant should be placed under a radiant warmer and PPV should be initiated if needed. Routine intubation for tracheal suction is no longer suggested because there is insufficient evidence to continue this recommendation.

Assessment of heart rate remains critical during the first minute of resuscitation and the use of a 3-lead ECG may be reasonable, because providers may not assess heart rate accurately by auscultation or palpation, and pulse oximetrymay underestimate heart rate. Use of the ECG does not replace the need for pulse oximetry to evaluate the newborn’s oxygenation.

Resuscitation of preterm newborns of less than 35 weeks of gestation should be initiated with low oxygen (21% to 30%) and the oxygen titrated to achieve preductal oxygen saturation approximating the range achieved in healthy term infants.