Embed Size (px)
DESCRIPTION
OECD Mark Pearson - Can health become an even bigger part of the economy without undermining fiscal sustainability? 31 January 2014.
Citation preview

CAN HEALTH BECOME AN
EVEN BIGGER PART OF THE
ECONOMY WITHOUT
UNDERMINING FISCAL
SUSTAINABILITY?
Mark Pearson
Deputy Director
Employment, Labour and Social Affairs
New Approaches to Economic Thinking Seminar on Project C3, 31 January 2014

• Health spending is likely to continue to
grow as a share of the economy
• This will put great pressure on public
budgets unless:
– We improve value for money
– We reallocate public funds from other areas
– We raise the efficiency of public funding for health
– We get more private finance into the system
2
Key points

HEALTH AND THE ECONOMY
3

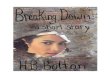
Health spending outpaced economic growth
in the pre-crisis period
Source: OECD Health Statistics 2013 4
Annual growth rate of health spending per capita and real GDP per capita, 2000-2009
AUS
AUT
BEL CAN
CHI
CZE
DEN
EST
FIN
FRA DEU
GRC
HUN
ISL
IRL
ISR ITA
JPN
KOR
LUX
MEX
NLD
NZL
NOR
POL
PRT
SVK
SVN ESP
SWE
CHE
GBR
USA
0%
2%
4%
6%
8%
10%
12%
-1% 0% 1% 2% 3% 4% 5% 6%
Av
er
ag
e a
nn
ua
l g
ro
wth
ra
te i
n r
ea
l h
ea
lth
e
xp
en
dit
ur
e p
er
ca
pit
a
Average annual growth rate in real GDP per capita

5
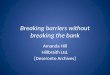
The crisis has moderated rapid growth in
health spending 5.3
7.0
1.6
7.2
1.8
5.3
3.3
3.8
5.9
4.1
1.6
3.0
4.1
2.2
2.8
3.7
3.1
2.1
3.5
4.5
5.5
7.1
3.4
1.9
3.9
3.4
2.1
3.1
10.9
1.3
2.8
7.5
9.3
-11.1
-6.6
-3.8
-3.0
-2.2
-1.8
-1.8
-1.2
-0.8
-0.5
-0.4
0.0
0.2
0.2
0.5
0.6
0.7
0.7
0.8
0.8
1.0
1.2
1.3
1.4
1.6
1.8
2.1
2.6
2.8
3.4
4.9
5.5
6.3
-15
-10
-5
0
5
10
15
Gre
ece
Irela
nd
Icela
nd
Esto
nia
Port
ug
al
Un
ite
d K
ing
dom
De
nm
ark
Slo
ven
ia
Czech R
epu
blic
Spain
Ita
ly
Austr
alia
OE
CD
32
Austr
ia
No
rwa
y
Belg
ium
Me
xic
o
Fra
nce
Ca
nad
a
Ne
w Z
eala
nd
Ne
therl
and
s
Pola
nd
Un
ite
d S
tate
s
Sw
itzerl
and
Fin
land
Sw
ede
n
Germ
any
Hu
nga
ry
Slo
vak R
epub
lic
Isra
el
Japa
n
Ch
ile ¹
Kore
a
2000-2009 2009-2011
1. CPI used as deflator. Source: OECD Health Statistics 2013
Annual avera
ge g
row
th r
ate
(%
)
Annual average growth rate in per capita health expenditure, real terms, 2000 to 2011 (or nearest year)

6
But even still, health has been a major
contributor to growth over the last decade
Contribution of health to growth in GDP per capita (%), 2000 to 2011

Health and social care is a fast growing
source of employment in many countries
Source: OECD Database on Labour Force Statistics, countries selected reflect the availability of data 7
Change in employment between 2000 and 2011, various industries
-60%
-40%
-20%
0%
20%
40%
60%
80%
100%
Ireland Spain Australia Canada UnitedKingdom
Austria France Finland CzechRepublic
All activities Agriculture Industry Services Human health and social work activities

Poor physical and mental health hits the labour market
Employment Wages Absenteeism
Obesity
Lower probability of employment (causal)
Larger wage penalties
(causal)
(Lundborg et al. 2010, Sweden)
More sickness absences,
especially for women (causal)
Alcohol Use
Long-term light
drinkers have better employment opportunities
(Jarl et al 2012, Sweden)
Moderate drinking positively associated with
wages
(Hamilton and Hamilton 1997, Canada)
Absences 20% higher
among abstainers, former and heavy drinkers (causal)
(Vahtera et al 2002, Finland)
Smoking
Heavy smokers more
likely to be unemployed (Jusot et al. 2008, France)
(possible causality)
Smokers earn 4-8% less than non-smokers
(causal)
(Levine et al. 1997, USA)
Smokers 33% more likely
to be absent from work than non-smokers
(causal)
(Weng et al. 2012, meta-analysis) 8

Sickness absence incidence Average absence duration Presenteeism incidence
42
28
19
21
0
5
10
15
20
25
30
35
40
45
Severe disorder
Moderate disorder
No disorder
7.3
5.6
4.8
5.2
0
1
2
3
4
5
6
7
8
Severe disorder
Moderate disorder
No disorder
88
69
26
35
0
10
20
30
40
50
60
70
80
90
Severe disorder
Moderate disorder
No disorder
Source: OECD (Sick on the Job:? Myths and Realities about Mental Health and Work).
Sickness absence (% and duration) and productivity losses at work (%)
Productivity losses through mental-ill health are
large

HEALTH AND PUBLIC FINANCES
10

Health care is predominately publicly funded
8
73
85
5 9
83
75
9
82
51
11
78
32
4 7
10
60
7 2
68
27
35
6
69 68 67
24
64
19
8
17
11 6
22
38
77
12
79 74
8
73
30
69
45
73 70
65
15
67
71
5
46
37
65
1
42
1
46
56
45
46
43
25
7
6
15 13 15 12
10 11 15 17 18 18 18 17
8 12
20 20 24
12
21 19 20 24
16 20 18
31 29
26 27
25 37
12
49
38
6
2 0
3 5
2 1 5
14 10
4 2
14
6 6 1
13 8 12
3 5
9 3 10
6
35
4
17
0
10
20
30
40
50
60
70
80
90
100
Ne
therl
and
s
No
rwa
y
De
nm
ark
Czech R
epu
blic
Lu
xe
mbo
urg
Un
ite
d K
ing
dom
¹
Ne
w Z
eala
nd
Japa
n
Sw
ede
n
Icela
nd
Esto
nia
Ita
ly ¹
Austr
ia
Fra
nce
Germ
any
Belg
ium
Fin
land
Slo
vak R
epub
lic
Slo
ven
ia
Spain
Turk
ey
OE
CD
34
Pola
nd
Ca
nad
a
Austr
alia
Irela
nd
¹
Gre
ece
Port
ug
al
Sw
itzerl
and
Hu
nga
ry
Isra
el
Kore
a
Un
ite
d S
tate
s
Me
xic
o ¹
Ch
ile
General Government Social Security Private out-of-pocket Private insurance Other
% o
f c
urr
en
t e
xp
en
dit
ure
1. Data refer to total health expenditure. Source: OECD Health Statistics 2013
11

This will make health a major pressure on public budgets
across all OECD countries
Source: OECD Economic Policy Paper n°06, 2013 12
0%
2%
4%
6%
8%
10%
12%
Average public spending 2006-2010 Increase of public spending 2010-2030 Increase of public spending 2030-2060
% GDP

Drivers of healthcare expenditure growth between 1995 and 2009 in OECD countries
Ageing is not the key driver of health spending
growth
Healthcare expenditure growth (100%)
Demography (12%)
Age structure
Health by age
Income (42%)
Residual (46%)
Relative prices
Technology
Institutions and policies
Source: OECD Economic Policy Paper n°06, 2013
13

• Implications:
– Intergenerational transfer
– As ageing is not the driver we cannot ‘ride out’ health spending by letting budgets run into deficit
– The policy challenges are productivity, relative budget priority and the boundaries of financing
What do we mean by fiscal
sustainability?
14
IMF: The capacity of a government, at least in the future, to finance its desired expenditure programs, to service any debt obligations […] and to ensure its solvency.
EU: This considers the ability of the government to meet the costs of its current and future debt through future revenues (Indicator S1). The finite version of the budget constraint is assessed with reference to a target date of 2030 and a target level of debt of 60 % of GDP (Indicator S2)

OPTIONS 1. EFFICIENCY
15

16
Improving health sector productivity can
dramatically change the fiscal outlook
Sensitivity of public sector net debt projections to interest rates
Sensitivity of public sector net debt projections to health productivity
Source: Fiscal Sustainability Report, UK Office for Budget Responsibility, July 2013

The target areas for expenditure control are
well known among Finance Ministries
17
0 5 10 15 20
Outpatient care spending
Primary health care services
Spending on prevention programs
Long term care spending
Pharmaceutical costs
Hospital expenditure
Source: OECD Survey on Budget Practices and Procedures, 2013
Number of countries
Self-reported priorities for expenditure control, 22 OECD countries

18
The crisis has been used to slow growth in desirable
areas, but we have fallen short on prevention
4.8% 4.8%
5.9%
2.9%
6.9%
2.5%
3.2%
4.6%
6.2%
2.8%
6.4%
3.5%
0.7% 0.9%
5.3%
0.2%
-1.5%
-0.9%
1.0%
1.7% 1.6%
-1.7% -1.7%
1.7%
-3%
-2%
-1%
0%
1%
2%
3%
4%
5%
6%
7%
8%
Inpatient care Outpatient care Long-term care Pharmaceuticals Prevention Administration
2007/08 2008/09 2009/10 2010/11
Source: OECD Health Statistics 2013
Average annual growth rates of spending for selected functions, OECD average, in real terms

Proportion of people being treated by a specialist or non-specialist, by severity of their mental disorder
0
10
20
30
40
50
60
70
80
Seve
re
Mo
de
rate
No
ne
Seve
re
Mo
de
rate
No
ne
Seve
re
Mo
de
rate
No
ne
Seve
re
Mo
de
rate
No
ne
Seve
re
Mo
de
rate
No
ne
Seve
re
Mo
de
rate
No
ne
Seve
re
Mo
de
rate
No
ne
Austria Belgium Denmark Netherlands Sweden United Kingdom OECD-21
Non-specialist Specialist
Treatment rate (in %)
Source: OECD (Sick on the Job:? Myths and Realities about Mental Health and Work).
There are pervasive under-treatment issues in
mental health

Worthwhile processes are not being
undertaken with consistency
Distribution of French GPs: % of diabetic patients having 3 or more HBA1C tests during the year in the last 12 months (2009)
Average=40% Target=65%
10 20 30 40 50 60 70 80 90

Considerable medical practice variations
within and between countries
21
Note: Rates are standardised using OECD’s population structure. Missing country data will be added once available. Source: National reports submitted for the OECD project on Medical Practice Variations.
Rates of PTCA (standardised for age and sex) per 100,000 population, 2011 (or earliest
available)
Rates of Coronary Artery Bypass Grafting (standardised for age and sex) per 100,000
population, 2011 (or earliest available)

OPTIONS: 2. REALLOCATE PUBLIC
SPENDING TOWARDS HEALTH
22

23
Countries have allowed health to become a
bigger share of their budget
Source: OECD National Accounts Statistics (database). Data for Australia are based on Government Finance Statistics provided by the Australian Bureau of Statistics.
-2%
-1%
-1%
0%
1%
1%
2%
2%
Social protection Health Recreation,culture and
religion
Environmentalprotection
Public order andsafety
Education Housing andcommunityamenities
Defence Economic affairs General publicservices
Change in the structure of general government expenditures on average in OECD countries by function (2001 to 2011)

OPTIONS: 3. GET A MORE SUSTAINABLE WAY OF FINANCING PUBLIC EXPENDITURE ON HEALTH
24

25
Our models incorporate estimates of how an ageing
population will increase utilisation of health services…
26% 27% 28% 28% 29% 29% 30%
31% 32%
32% 33%
34% 35%
35% 36%
37% 38%
39% 39% 40% 41% 41% 42% 43% 43% 44% 44% 45%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
201
3
201
4
201
5
201
6
201
7
201
8
201
9
202
0
202
1
202
2
202
3
202
4
202
5
202
6
202
7
202
8
202
9
203
0
203
1
203
2
203
3
203
4
203
5
203
6
203
7
203
8
203
9
204
0
Old age (+65) dependency ratio (20-64), OECD

… but they do not account for shortfalls in revenues
for countries that rely heavily on payroll taxes
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Other
Sin taxes
Taxes on (company) profits
Taxes on goods and services
Income taxes
Mandatory health insurancepremium
Payroll contributions
Other general taxation
Average share of different sources of revenues for funding health care expenditure, selected OECD countries

• ‘Sin taxes’ are increasingly being used by OECD countries
– These taxes target lifestyle choices that can affect productivity and employment outcomes.
– The arguments for using taxes to attain public health objectives are strong for tobacco products and alcohol.
– The poor are likely to pay more but have greater health benefits.
Some new taxes could be effective in improving
health, but will not be major sources of revenue
27

OPTIONS: 4. LET PRIVATE SPENDING RISE
28

29
Source: Paris et al., Measuring coverage (Forthcoming)
Boundaries between public and private
need to be debated

It is unlikely that countries will want to step back from
covering 100% of their population
100.0
100.0
100.0
100.0
100.0
100.0
100.0
99.8
100.0
100.0
100.0
100.0
100.0
100.0
100.0
100.0
100.0
100.0
100.0
100.0
99.9
99.9
88.9
99.9
99.0
99.5
98.8
97.2
79.8
96.6
95.2
92.9
86.7
31.8
0.2
11.0
0.9
17.0
53.1
0 20 40 60 80 100
Australia
Canada
Czech Rep.
Denmark
Finland
Greece
Hungary
Iceland
Ireland
Israel
Italy
Japan
Korea
New Zealand
Norway
Portugal
Slovenia
Sweden
Switzerland
United Kingdom
Austria
France
Germany
Netherlands
Spain
Turkey
Belgium
Luxembourg
Chile
Poland
Slovak Rep.
Estonia
Mexico
United States
Total public coverage Primary private health coverage
Percentage of total population
30 Source: OECD health data, 2013

Some shift to private financing
-0.4%
0.1% 0.0% 0.5%
-1.0%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
GeneralGovt./SHI
Private HealthIns.
Out-of-Pocket Total Health Exp.
2007/08 2008/09 2009/10 2010/11
Source: OECD Health Statistics 2013

• The ‘theoretical’ advantages of private health insurance:
– Expanding individual choice
– Spur innovation and flexibility
– Reduce public cost pressure
• The practical risks associated with private health insurance:
– higher administrative costs
– less bargaining power for insurers
– risk selection
– Pressure for tax incentives
32
Private health insurance markets are not
necessarily cost reducing

• Be more specific and selective in defining the range of services covered
• Health systems have become better at assessing new activities, but this misses most spending:
– Cost effectiveness analysis studies are used to assess whether a new service or drug should be funded
– A more systematic assessment of therapeutic strategies by disease should be conducted
33
A better way to cost share…

• Health spending is likely to continue to
grow as a share of the economy
• This will put great pressure on public
budgets unless:
– We improve value for money
– We reallocate public funds from other areas
– We raise the efficiency of public funding for health
– We get more private finance into the system
34
Key points

CAN HEALTH BECOME AN EVEN
BIGGER PART OF THE ECONOMY
WITHOUT UNDERMINING FISCAL
SUSTAINABILITY?
31st January 2014 Mark Pearson Deputy Director Employment, Labour and Social Affairs