Embed Size (px)
Citation preview
Mohammed Almuzian
Breathing and malocclusion as well as Obstructive sleep apnoea
13

Contents
Respiration is controlled by the followings..............................................................................1
Breathing and the upper airway system..................................................................................1
Causes of upper airway obstruction.........................................................................................2
Consequences of nasal obstruction..........................................................................................2
Head posture or position..........................................................................................................3
Treatment option for nasopharyngeal and oropharyngeal obsrtuction...................................4
Sleep related sleeping disorders OSA.......................................................................................5
Types of sleeping disorders......................................................................................................5
Definition of OSA......................................................................................................................5
Pathophysiology.......................................................................................................................5
Prevalence................................................................................................................................5
Classification of OSA.................................................................................................................5
Aetiological factors...................................................................................................................6
Sign and Symptoms, Jurdya 2004, Coborune 2011..................................................................6
Complications...........................................................................................................................7
Diagnosis.................................................................................................................................. 7
Treatment................................................................................................................................ 8
Ideal Features of MAA............................................................................................................10
Classification of MAA..............................................................................................................10
Advantages of MAA................................................................................................................10
Disadvantage of MAA.............................................................................................................11
Breathing and malocclusion as well as Obstructive Sleep Apnoea
Mohammed Almuzian, University of Glasgow 1
Respiration is controlled by the followings:
1. Sensors:
Central chemoreceptors, which respond to changes in the chemical composition of the
blood or other fluid around it (found in the ventral surface of the medulla)
Peripheral chemoreceptors in the carotid bodies which respond to decreases in arterial 0 2
and pH levels
Lung receptors - stretch receptors, irritant receptors and others
2. Other reflex mechanism
Nasal and upper airway (mechanical and chemical)
Gamma system in inter-costals muscles (detect stretching)
Joint and muscle (stimulate breathing in exercise)
Arterial baroreceptors (detect blood pressure levels)
Pain and temperature
Breathing and the upper airway system
In the nose, the nasal passages contain three conchae which are lined with
mucous membranes that aid in:
1. Air warming, within 37 degree of body temperature.
2. Air humidifying through the mucous within 2-3% of the maximum humidification.
3. Air filtering by the mechanism of nasal hair filteration, turbinlation mechanisim
as well as the cilia of the pseudostratified columnar epithelium.
4. The turbinate bone - the conchae - also aids to increase the size of the surface
area of the nasal passage.
When breathing is done through a tube (as for example, in a tracheostomy), this
effect will be absent and so the drying effect on the lower lung can lead to
serious lung crusting and infection (Guyton and Hall, 1996).
Causes of upper airway obstruction
A. Nasal
1. Soft tissue
Mohammed Almuzian, University of Glasgow 2
Allergies
Hyperplasia
2. Hard tissue
Nasal anomalies
Deviated nasal septum Trauma
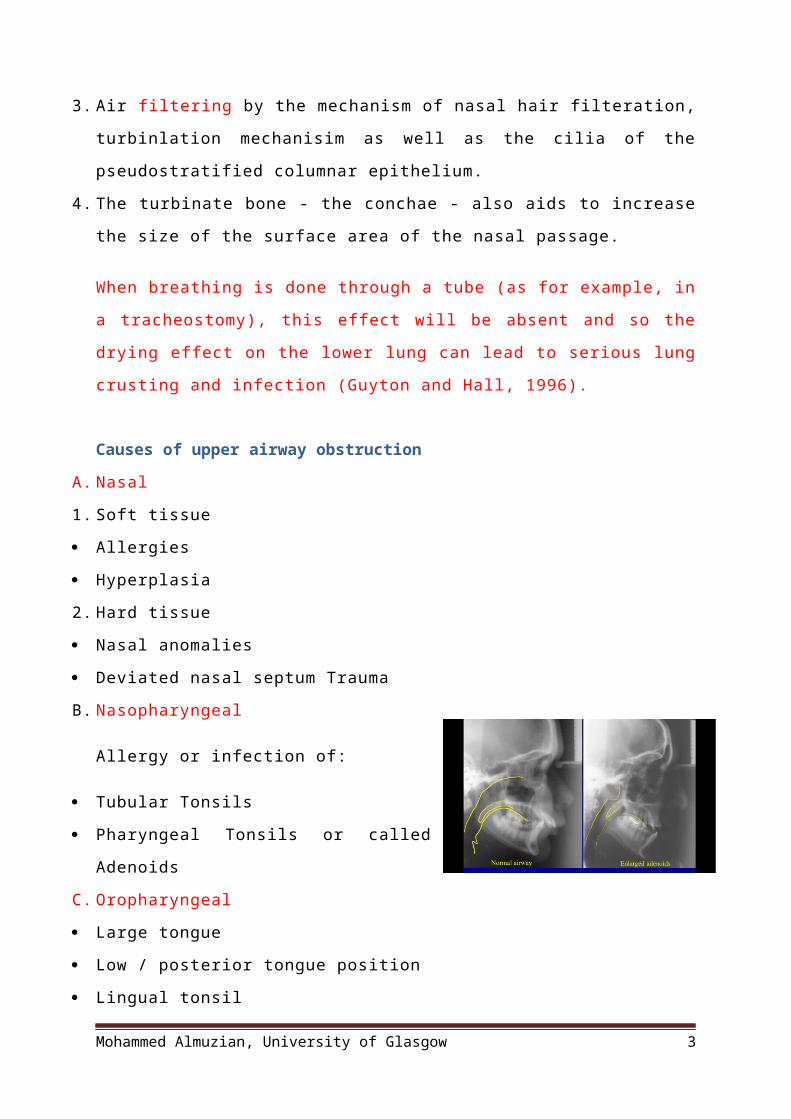
B. Nasopharyngeal
Allergy or infection of:
Tubular Tonsils
Pharyngeal Tonsils or called Adenoids
C. Oropharyngeal
Large tongue
Low / posterior tongue position
Lingual tonsil
Waldeyer's tonsillar ring
• Waldeyer's tonsillar ring is an anatomical term collectively describing the
arrangement of lymphoid tissue in the pharynx. Waldeyer's ring was named after
the nineteenth century German anatomist Heinrich Wilhelm Gottfried von
Waldeyer-Hartz.
• The ring consists of the (from posterior to anteriro):
A. One pharyngeal tonsils (or nasopharyngeal tonsil(s), due to the location; also
known as 'adenoid(s)' when inflamed/swollen
B. Two tubal tonsil (bilaterally, where each Eustachian tube opens into the
nasopharynx)
C. Two palatine tonsils (commonly called "the tonsils" located in the oropharynx)
D. One (or many) lingual tonsils (on the posterior tongue).
Mohammed Almuzian, University of Glasgow 3

Head posture or position
Represent the relationship of the head to H or V lines and mainly the position or angulation
of the cranial base in relation to vertebral axis. It is very reproducible position. It depends
on:
1. Visual axis
2. Hearing
3. Balance
4. Breathing
5. Swallowing
6. Gravity
Treatment option for nasopharyngeal and oropharyngeal obsrtuction
1. Pharmacological
2. Turbinectomy
3. Nasal septoplasty
4. Tonsileectomy or adenictomy ( no evidence)
5. Tongue reduction
6. BSSO advancement
7. RME (no evidence)
8. MAA
Functions of sleep
1. Fatigue reversal: Sleep allows the individual to recover and reenergize.
2. Biochemical refreshment
• Sleep promotes synaptic efficiency, protein synthesis, neurogenesis, metabolic (eg,
glycogen) restoration, growth (secretion of growth hormone peaks during sleep), etc.
• Immune function and Reset or protection.
3. Memory
• Daytime learning needs sleep for memory consolidation.
• Sleep seems to facilitate encoding of new information.
Mohammed Almuzian, University of Glasgow 4
4. Psychologic well-being
• Dreams occur in all sleep stages. REM dreams are more vivid.
• Lack of sleep presents a risk of mood alteration to depression.
Sleep efficiency
it is defined as the amount of time asleep divided by the amount of time spent in bed,
expressed as a percentage. Sleep efficiency greater than 90% is an indicator of good sleep.
Sleeping cycle
• Sleep Rechtschaffen and Kales introduced a standardization of human sleep that divides it
into five distinct stages, the first four belonging to slow-wave (non-REM) sleep and the last
one being REM sleep.
• The duration of a sleep cycle is about 90 minutes, and the first cycles are shorter than the
last ones.
• There are in general four to six sleep cycles during a night, depending on the total sleep
time.
• The first two cycles are generally complete with successive attendance in all sleep stages.
• During the later cycles the contribution of stages 3 and 4 diminishes gradually, and sleep
bounces between stage 2 and REM sleep.
• The REM episodes are generally short (5 minutes) in the early cycles but can attain 1 hour
during the last cycle.
A. Non-REM sleep:
• During non-REM sleep the muscular tone remains present in the EMG.
• Ocular and axial muscular movements are absent, with the exception of occasional postural
adjustments.
Mohammed Almuzian, University of Glasgow 5

1. Sleep begins with stage 1, which is a transitory epoch of about 1 to 10 minutes,
characterized by a slight increase in the EEG amplitude and appearance of scattered
triangular waveforms called vertex waves (they are most evident in the vertex leads).
2. Deepening of non-REM sleep toward stage 2 is announced by increased amplitude of the
EEG. Vertex waves increase in amplitude and are termed K-complexes also termed sigma
waves; generally 10 to 14 Hz
3. Stage 3 is generally equivalent to the beginning of deep sleep. Between 20% and 30% of the
EEG activity consists of high-amplitude (greater than 50 μV) slow waves (less than 4 Hz,
termed delta waves).
4. Sleep stage 4 is recognized when more than 50% of the EEG activity is spent in delta waves.
The amplitude of the waves reaches the highest values (around 100 μV). In clinical
recordings, stages 3 and 4 are usually reported as one sleep state.
B. Transition to REM sleep
• Stage 4 is ended by a return to lighter sleep (stages 3 and 2) and subsequent entrance into
REM sleep.
• Major features are specific for REM sleep:
1. Very low EMG activity,
2. Axial muscular hypotonia,
3. Rapid eye saccades that trigger large deflections in the EOG.
Elements of the medical and social history and clinical examination to include in the
patient’s medical record
A. History
1. Symptoms related to insomnia:
- Sleep duration (when the patient goes to sleep and when the patient awakens)
- Number of awakenings
- Trouble falling or staying asleep (number of nights per week)
Mohammed Almuzian, University of Glasgow 6
- Number of times the patient gets up in the night to go to the bathroom
- Use of medication or alcohol to fall asleep
- Use of pain or anxiety-related medication
2. Symptoms related to sleep-disordered breathing:
- Snoring
- Cessation of breathing
- Choking
- Awakening gasping for breath
- Tendency to fall asleep during the daytime (Epworth sleepiness scale)
- History of hypertension and other cardiovascular disorders (eg, ischemic heart disease,
stroke, night sweating, loss of memory, morning headache, difficulty concentrating)
- Nocturia/enuresis
3. Symptoms related to movement disorders:
- Tooth grinding sounds during sleep (sleep bruxism)
- Tooth tapping (faciomandibular myoclonus or sleep-related epilepsy)
- Leg or arm movement during sleep, with or without injuries (periodic limb movement,
REM behavior disorder)
- Body rocking or head banging
4. Other symptoms:
- Eating during the sleep period (may exacerbate insomnia or sleepd isordered breathing)
B. Clinical examination
• Weight, height, and body mass index
• Neck circumference (at risk if greater than 41cm [women] or 43 cm [men])
• Retrognathia (Class II)
• Deep palate
• Narrow dental arches
• Tongue size (macroglossia)
• Tongue indentation (tongue thrusting habit or tic)
• Adenoids and tonsil size
• Oropharyngeal size, viewed through the mouth (Mallampati classification). Modified
Mallampati Scoring:[3]
I. Class I: Soft palate, uvula, fauces, pillars visible.
Mohammed Almuzian, University of Glasgow 7
II. Class II: Soft palate, uvula, fauces visible.
III. Class III: Soft palate, base of uvula visible.
IV. Class IV: Only hard palate visible.
• Nose shape (narrowing) and obstruction
• Usual body position (supine is a risk factor for respiratory disorders and bruxism)
• Tooth wear or damage or use of oral splint (bruxism or orofacial pain)
• Absence of tooth or protrusive mandibular movement (precludes use of oral appliance to
treat sleep-disordered breathing)
Sleep related sleeping disorders OSA
Types of sleeping disorders
1. Sleep bruxism
2. upper airway resistance syndrome (UARS)
3. Habitual snoring
Mohammed Almuzian, University of Glasgow 8

4. Obstructive sleep apnoea (OSA)
5. Central sleep apnea
UARS
It is characterized by partial collapse of the upper airway, without the occurrence of
obstructive apneas and hypopneas.3 It is thought to be an intermediate form of sleep-
related breathing disorder, between snoring and frank OSA.
Sleep bruxism (tooth grinding)
It is a repetitive activity (repeated at least 3 times per episode) in the jaw muscles (rhythm
at 1 Hz, of bursts lasting more than 0.5 and upto 2.0 seconds) that generates tooth grinding
sounds and occasional jaw clenching (a sustained muscle contraction of more than 2.0
seconds). As is the case with snoring,generally sleep partners are the ones who complain of
tooth grinding sounds.
Prevalence: in infants 14% to 18%. And in adult 8%
The consequences of sleep bruxism may include tooth destruction (tooth wear or
restoration destruction), morning headache, jaw pain, and a limited ability to open the
mouth due to muscle tension or meniscus displacement
Habitual Snoring
Snoring is an acoustic phenomenon produced by the vibration of the pharyngeal tissues as
air passes through a narrow orifice created by the relative positions of the soft palate and
the base of the tongue. It is an almost exclusively inspiring noise but can persist on
expiration when there is a partial blockage of the airway as is the case with patients with
OSA. It initiates when falling asleep, intensifies as sleep progresses to non-REM sleep and
then weakens and discontinues during REM sleep. Snoring is one of the cardinal symptoms
of OSA, but not all snorers have sleep apnea. Itappears to be the milder and initial form of
upper airway dysfunction leading to OSA.
Habitual snoring has been reported as occurring in up to 24% of the male population and up
to 14% of the female population. The prevalence increases with age, reportedly affecting
40% - 60% of the middle-aged population”.
Mohammed Almuzian, University of Glasgow 9

OSA
OSA is characterized by more than 5 repetitive episodes (more than 10 seconds) of upper
airway obstruction in each hour of sleeping, usually associated with a reduction in blood
oxygen and associated symptoms such as daytime sleepiness, impaired cognition and
fatigue an AHIof 15 or greater regardless of associated symptoms.
Before Measurement Techniques were outlined in 2010 the prevalence of OSA was varied in
the literature due to different measurements used in the past. Using AHI > 5 with no other
symptoms gives a prevalence of 24% of men and 9% of women whilst an AHI > 15may be
found in 9% of men and 4% of women. When the second criteria of day-time sleepiness is
added as required for OSAS, these figures fall to 4% and 2% for men and women
respectively
The prevalence of OSA increases as Body Mass Index [BMI] increases. The prevalence ofOSA
is 41% in overweigh people with a BMI over 28 and as high as 78% in morbidly obese
patients.
Central Sleep Apnea (CSA)
CSA is characterized by recurrent apneic episodes during sleep in the absence of an upper
airway obstruction and with minimal or no respiratory effort due to cessation of respiratory
drive. Similar to OSA this results in oxygen desaturations, recurrent arousal and day-time
s1eepiness.
the exact prevalence remains unknown
Apnea-Hypopnea Index (AHI)
The Apnea-Hypopnea Index [AHI] is the average number of apneas and hypopneas perhour.
The suggested AHI cut points are 5, 15, and 30 events/hour to indicate mild, moderate, and
severe levels of OSA respectively
Mohammed Almuzian, University of Glasgow 10
Respiratory Disturbance Index (RDI)
This is also measured as events per hour of sleep and takes into account the average
frequency of apneas and hypopneas as well as reductions of airflow with resultant arousal
but without meeting the desaturation criteria for a hypopnea
Pathophysiology
1. The respiratory blockage occurs at the level of the nasopharynx or oropharynex when the
tongue falls backward and blocks the airway during sleep.
2. Obstruction can occur at a single or multiple levels along the upper airway, with
theoropharynx or retroglossal airway being the most common site
3. The sleep is interrupted by periods of apnoea where the patient stops breathing for up to
15-20 seconds at a time.
4. When the CO2 level in the blood rises to a certain point (hypercapncea), it causes a sudden
reflex intake of breath and breathing starts again.
Prevalence
1. Adult population: 2% female and 4% male. (Bixler 2009)
2. In children 0.7% in Europe & 1,2% in USA (Bixler 2009)
3. More in Afro-Caribbean than other
Classification of OSA
This is done according to HAI (hypopnea and apnoea index)
1) Mild (5-15) episode of apenea per hour
2) Moderate (16-30) episode of apenea per hour
3) Sever (>30) episode of apenea per hour. In people with severe OSA these apnoea can
happen up to 400 times per night.
Aetiological factors
A. Anatomical factors
1. Genetically determined retro-positioned facial skeleton
2. Functional impairment of the upper airway dilatory muscles.
Mohammed Almuzian, University of Glasgow 11
3. Chronic snoring: Upper airway muscle activity decreases during sleep leading to increased
collapsibility of the pharyngeal tissues.“ Oedema or inflammation of pharyngeal tissues due
to heavy snoring might not only narrow the upper airway but might also impair normal
function of the receptors responsible for initiating protective reflexes.”
4. Craniofacial anatomy
Congenitally reduced nasopharyngeal and /or oropharyngeal dimensions as in some
syndrome like Down, hypothyrodisim, Achndroplasia, Apert & Pierr Robin syndrome
Enlarged tongue.
Enlarged tonsils.
Nasal septal deviation
Blocked nose by allergy or rhinitis
B. Risk factors
1. Age: OSA prevalence increases steadily with age throughout midlife with a 2- to 3-fold
higher prevalence in persons above 65 years of age compared with those between 30-64
years of age. After 65 years it seems to plateau. This is due to
Dimensional changes in the airways related to age,
increased size of the soft palate,
Posterior positioned tongue
the inferior repositioning of the hyoid bone,
2. Gender: Twice more in male than female. This may be attributed to differences in:
upper airway shape
genioglossal muscle activity during the awake state, in craniofacial morphology,
pattern of fat deposition around the pharynx. Males have greater upper-body fat
distribution and fat in the neck which males make them more susceptible to upper airway
collapse
3. Genetics; The association of OSA amongst family members may be a reflection of lifestyle,
but there are studies supporting a genetic predisposition to OSA in relation to craniofacial
structure, body fat distribution and neural control of the upper airway muscles
Mohammed Almuzian, University of Glasgow 12
4. Ethnicity; OSA has a greater prevalence in Asian and African—American populations
according to some studies, but at present, data from studies of groups other than white
subjects are too sparse to determine with confidence if prevalence differs worldwide.”
5. Obesity: It is estimated that a 10% increase in weight is associated with a 6-fold greater risk
of developing OSA among persons initially free of OSA. The correlation between OSA and
BMI is weak though due to the fat distribution not being homogenous among obese people
6. Alcohol Intake: Alcohol and sedatives have an acute inhibitory effect on the genioglossal
activity of thetongue & upper airway dilators that leads to an increase in snoring and as well
as apnea andhypopnea frequency
7. Smoking
8. Sedatives, which can relax throat muscles, contributing to the collapse of the airway at night
9. Hypothyroidism.
10. Sleeping posture: Supin-dependent OSA or positional sleep apnea refers to patients who
displays higher AHI when they are sleeping on their back compared to when they are
sleeping on their side and comprises of an average of 56% of patients with OSA. Positional
therapy can be used to prevent a patient from sleeping in the worst sleeping position which
is usually, but not exclusively, the supine position.
11. Hormonal:
• increase in testosterone
• reduction in progesterone or menopause
• Hypothyroidism
• Acromegaly
• Down syndrome
• Marfan syndrome
Sign and Symptoms
Signs and symptoms associated with OSA (mentioned by Magliocca & Helman 2005, Jordan
2005)
A. Nocturnal Signs and symptoms
1. Snoring or witness snoring
2. Apnoeas or witness apnea
Mohammed Almuzian, University of Glasgow 13
3. Choking or gasping
4. Restless sleep
5. Notcturia
6. Drooling
7. Xerostomia
B. Daytime Signs and symptoms
1. Presence of the risk factors mentioned above
2. Morning headaches assessed by Epworth sleeping Score
• Sleepiness over recent times can be subjectively measured in using the Epworth Sleepiness
Scale (ESS), first described by Johns 1991.
• This self-reported 8 item scale assesses the likelihood of falling asleep in various scenarios
commonly encountered in daily life
• Subjects are asked to rate the chance of falling asleep in each circumstance from 0 (no
chance of dozing) to 3 (high chance of dozing).
• The scores are tallied to give a total between 0 – 24, with those above 12 indicating
excessive sleepiness
• The ESS focuses on levels of sleepiness over the preceding two weeks and can be used to
subjectively quantify sleepiness and assess change due to treatment effects
3. Excessive sleepiness
4. Impaired concentration
5. Depression
6. Decreased libido (Sexual problem)
7. Irritability
C. Cephalometric feature
Solow et al. (1993, 1996) found that OSAHS patients have a high cervico-cranial angle
compared to non-OSAHS subjects. This had been explained by Hellsing (1989) who found
that elevation of the head also resulted in widening of the airway at this level, and as a
result it may be stated that OSAHS patients tend to hold their head in a more extended
position.
The SNA and SNB are severely reduced
Mohammed Almuzian, University of Glasgow 14
D. If OSA developed at early age with chronic nasal obstruction the following could be
occurred
1. Blockage of the nasal airway results in elevation of the head in relation to the true vertical
and the cervical column, in order to allow more air into the lungs. This has been shown in a
primate experiment by Solow and Talgren 1969 as well as Harvold (1981), where artificial
obstruction of the nasal airway in monkeys resulted in altered mandibular posture and an
anterior open bite after a year with class II tendency. However there is no strong evidence
to support this hypothesis. Vig et al 1981??
2. Pectoris excavatim where the intercostal muscle fail to develop.
3. Hearing problem due to obstruction in the Austachian tube and this could be improve by
RME, since RME help to increase the drainage from the tube
4. Nocturnal enuresis because of reduced vasopressin which normal released during Rapid Eye
Movement stage of sleeping (REM). In case of sever chronic nasal blockage, there will be
associated repeated apnea and so the REM is not achieved. (Kurol 2008)
5. Mental development because REM is not achieved then growth hormone will not be
secreted.
6. Due to the above reason there is an impact on psychology and quality health of life
Complications
1. Negative influence on the physical and mental growth, since the REM not achieved which is
essential to secrete growth hormone.
2. Due to poor sleep at night, consequently, drowsiness during the day with cognitive
impairment, impaired ability to operate a motor vehicle, and an increased automobile
accident rate.
3. Rise in CO2 levels over a long period of time can result in pulmonary hypertension, heart
failure and in some cases, sudden death during sleep due to stroke.
Diagnosis
1. History from patient and sleeping partner
2. Examination including
ENT visual examination and assessment.
Mohammed Almuzian, University of Glasgow 15
laryngoscopy,
endoscopy during wakefulness: Endoscopy during wakefulness of patients with OSA is
usually performed in the supineposition to assess the level of maximum narrowing in the
upper airway. The patient can beasked to perform the Muller maneuver, which consists of a
forced inspiratory effort againsta closed mouth and nose. The retropalatal and retrolingual
level of the pharynx can beinvestigated during this maneuver and may be used to detect
collapse in these areas. Thepredictive value of this maneuver is limited though, as it does
not necessarily reflect theobstructions during sleep,
nasendoscopy during sleep: Fiberoptic endoscopy performed whilst the patient is asleep is
known as nasendoscopy.It is a time consuming procedure if sedation is not used, but there
is a risk that sedativesmay increase OSA due to hypotonia of the genioglossus. A further
disadvantage is thatvarious levels of the airway cannot be observed simultaneously and
quantifying the cross-sectional area is difficult and once again semi-objective. Videotaped
images of the lumen canbe digitized and the cross-sectional area calculated, but it is a very
time-consuming task
Somnofluoroscopy: SomnofluoroscopyFluoroscopy is a dynamic radiographic examination of
the upper airway and incombination with PSG is called somnofluoroscopy. A preliminary
image is recorded of thepatient in the supine position whilst they are awake and then
further images are obtainedonce an obstructive event is witnessed on the PSG. This method
is not widely used due tothe significant radiation exposure and the airway only being shown
two—dimensionallywithout the possibility to make cross—sectional cuts
lateral cephalography,
CT scanning,
CBCT scanning and
MRI scanning.
3. Overnight polysomnography in sleep laboratory, measurements include:
AHI
Sleep time,
Sleep stages,
Respiratory effort,
Airflow,
Cardiac rhythm,
Mohammed Almuzian, University of Glasgow 16
Oximetry,
Limb movements
Body position
Treatment
1. Conservative treatment:
Supine dependent OSA is indicated by a difference of 50% or more in AHI between supine
and non-supine positions. Positional therapy can be used to prevent patients from sleeping
in the worst sleeping positions, which is usually, but not always, the supineposition. Long
term compliance remains an issue, but various techniques are used to prevent patients from
assuming the supine position such as positional alarms, tennis balls sown into vests, or
special pillows. MRI study has found that patients with positional have wider upper airways
in the lateral dimension, which may explain the maintenance of pharyngeal airway patency
in the lateral sleep position
Behavioural therapy: this will aim to reduce the risk factors. Many patients are told to avoid
smoking or alcohol, sleeping pills, and other sedatives, which can relax throat muscles,
contributing to the collapse of the airway at night
Bariatric surgery is increasingly performed for refractory medically complicated obesity. Due
to the improvement in AHI with weight loss, it is thought that bariatric surgery may play a
role in the treatment of morbidly obese OSA patients as an adjunct.
Pharmacological option: according to SIGN 2003 Pharmacological therapy should not be
used as first line therapy for OSAHS.
2. Surgery to widen the nasopharynx like:
Septoplasty
Turbinate surgery
Tonsillectomy
Uvulo-palato-pharyngo-plasty (UPPP or UP3) are available to address pharyngeal
obstruction. According to SIGN guidelines 2003 ‘’the use of UPPP or LAUP for the treatment
of OSAHS is not recommended’’.
Soft palate implants: it may attempt to shrink or stiffen excess tissue in the mouth or
throat; the insertion of a small piece of stiff plastic is used in the case of surgery whose goal
is to stiffen tissues, According to NICE guidelines 2007 Current evidence on soft-palate
Mohammed Almuzian, University of Glasgow 17

implants for obstructive sleep apnoea (OSA) raises no major safety concerns, but there is
inadequate evidence that the procedure is efficacious in the treatment of this potentially
serious condition for which other treatments exist. Therefore, soft-palate implants should
not be used in the treatment of this condition.
Tongue advancement.
By moving the major anchor point for the tongue forward, the procedure creates more
room for the tongue to relax during sleep without obstructing the throat. The result is an
enlargement and stabilization of the airway.
An incision is made inside the lower lip. The chin muscle and other soft tissues are cleared
away to expose the central part of the lower jaw. Small rectangular cuts (roughly 1 x 2 cm,
or less than ½ x 1 inch) are made in the lower jaw below the lower front teeth to capture
the area of attachment of the genioglossus muscle. This rectangle of bone is moved forward
and turned slightly. A small titanium screw is used to hold the bone fragment in place by
securing it to the remainder of the lower jawbone.
RISKS
1. Bleeding
2. Infection
3. Tooth injury
4. Chin and lower lip numbness
5. Change in appearance
6. Weakening of the lower jawbone
The jaw’s thickest, strongest portion is along the lower edge. This procedure is designed so
that this part of the bone is not disturbed.
7. Trouble swallowing.
Mandibular advancement surgery where the mandible is markedly class II (which advances
the tongue forward), With MMA, all the soft-tissue structures making up the pharyngeal
walls are tightened at once (including the palatophyrangeous, hyoglossus, genioglossus,)
this stops them from collapsing. The tongue is also pulled forward. The result is a significant
increase of posterior airway space (PAS) and the resolution of the syndrome in a high (95%)
percentage of cases
Mohammed Almuzian, University of Glasgow 18

Tracheostomy has proven value; due to the fact the incision by-passes the pharyngeal
airway. Naturally, the procedure is reserved for very severe obstructions which fail to
respond to other treatment modalities, in view of its psychosocial morbidity.
3. Non-surgical treatment
I- RME
II- PFM
III- Class II functional appliance
IV- CPAP (Continuous Positive Airway Pressure)
A CPAP device consists of a unit that generates airflow, which is directed to the airway via a
mask. Positive pressure is generated by the airflow, which prevents upper airway collapse.
Should be used for at least 6 hour per day/7 days a week
According to NICE guidelines 2006 and SIGN 2003, CPAP is recommended as a treatment
option for adults with mild OSAHS.
V- Tongue stabilising device (TSD)
A tongue-stabilizing device (TSD) is a preformed appliance and uses suction to protrude the
tongue and improve upper airway structure and function. The earlier designs were similar to
a mouthguard, covering the upper and lower teeth to assist retention, with a flexible bulb
into which the tongue was protruded (Cartwright, 1985). The current design has no dental
coverage, reduced bulk, and has the bulb being retained in place only by suction. There are
currently only limited data on the efficacy of the current device, which is commercially
available.
A tongue stabilizing device attaches to the end of the tongue using gentle suction andholds
the tongue in a protruding position. It increases the anteroposterior diameter of
thevelopharynx by displacing the tongue and soft palate anteriorly and the
velopharyngeallateral diameter is extended more with TSD than compared to MAS.
This mouthpiece is made of soft medical grade silicone that is non-irritating to the gums.
Unlike many oral devices that need to be fitted either in a laboratory or by using a boil-and-
bite technique, aveoTSD is ready-to-use right out-of-the-box. It is available in small,
medium, and large sizes, but the manufacturer states the medium fits about 95 percent of
patients.
Mohammed Almuzian, University of Glasgow 19

Indication and advantages:
When PD is compromised or when there is few teeth to hold MARA.
Less gag reflex
Less dental side effect
Deane and Darendeliler 2009 (RCT) Objective testing showed the MAS and TSD had similar
efficacy in terms of AHI reduction. Patients reported improvements with both devices;
however, better compliance and a clear preference for MAS was apparent when both
devices were offered. Longer term studies are needed to clarify the role of TSD.
VI- Mandibular advancement device (MAD) which are similar to functional appliances
SIGN 2003 guidelines: It is an alternative therapy for patients who are unable to tolerate
CPAP.
Cochrane review: by Carvalho 2008 for apnoea in children. It found that at present there is
no sufficient evidence to state that oral appliances or functional orthopaedic appliances are
effective in the treatment of OSAS in children. Another recent Cochrane review evaluated
randomised trials in adults with OSA (Lim 2004). The review found that oral appliances were
less effective than nasal CPAP and the use of oral appliances should be restricted to OSA
subjects unwilling or unable to cope with nasal CPAP.
Ideal Features of MAA
1. Robust
2. Adjustable
3. Minimal chair side time
Mohammed Almuzian, University of Glasgow 20
4. Good retention
5. Allow non-restricted movement of the mandible when it is in use.
6. Full occlusal coverage to prevent over-eruption of the teeth
7. Clinically proven
Mechanism of action
The first is that it protrudes the lower jaw forward to thrust the tongue base forward,
thereby enlarging the upper airway.
Another theory is that it decreases the pharyngeal collapsibility through improved muscle
tone. “ The lateral wall of the soft palate anatomically connects to the base of the tongue
through the palatoglossal arch. Anterior displacement of the mandible and tongue stretches
the soft palate, stiffening the Velopharyngeal segment and decreasing its collapsibility
Clinical and cephalometric predictors of successful treatment within MRA
1. Clinical predictors
• Younger age
• Lower body mass index
• Supine-dependent OSA
• Supine-dependent OSA
• Smaller oropharynx
• Smaller overjet
• Shorter soft palate
• Smaller neck circumference
• Lower AHI
2. Cephalometric predictors
• Shorter soft palate
• Longer maxilla
• Decreased distance between mandibular plane and hyoid bone
Mohammed Almuzian, University of Glasgow 21

Activation of the appliance
In general, the maximum protrusion is around 10mm. 20% of the maximum protrusion
increase in the advancement of the mandible can improve the polysomnographic variables
by 20%, but the ideal scenario is to undertake 75% advancement.
The degree of vertical opening has been shown not to have a significant impact on
treatment efficacy. For comfort levels, a decreased Vertical opening of 4mm compared
to14mm was preferred by patients.104 One study reported a decrease in the airway lumen
with increased vertical opening of the MAS most likely due to the posterior rotation of the
mandible.
Follow-up appointments with a dental specialist is recommended at least annually
toevaluate the health of the oral structures and integrity of the occlusion, evaluate
devicedeterioration and monitor patient adherence. If there are any signs and symptoms
tosuggest worsening of OSA, the patient should be referred to a sleep physician for
furtherassessment
Classification of MAA
The currently available appliances could be broadly classified into three types, based on a
succession of design modifications, which importantly permit incremental advancement of
the mandible:
A. First generation . (non-adjustable)These were primarily one-piece in
design, with no ability to incrementally advance the mandible.
B. Second generation . (semi-adjustable)This type of appliance was
principally two-piece in design and offered the potential for
incremental advancement. However, this would often necessitate
laboratory support and potentially were more time-consuming at the
chair side.
C. Third generation . (fully-adjustable)These appliances may be regarded as the ‘gold standard’
in design. They not only permit incremental advancement, which is
self-adjustable, but also lateral movement of the mandible, and
ensure the mandible is retained in its postured state during sleep
Mohammed Almuzian, University of Glasgow 22

Advantages of MAA
1) Non-invasive
2) Inexpensive
3) Easy to use in case of travelling
4) Clinically proved (Johal, 2004) to:
Effective in reducing snoring (40-60%)
Improve sleep quality
Reduce blood pressure
The durability of 0A is estimated at 1.5 to 3 years,
Compliance rate of 52-100% reported (Johal 1999)
Disadvantage of MAA
1) Hypersalivation
2) Muscle discomfortability
3) Change in the bite
4) TMJ problem
1.
Mohammed Almuzian, University of Glasgow 23





























