Embed Size (px)
Citation preview

Brain and Craniofacial Trauma
Lt. Colonel Brenda Sowards, RN

Head Trauma
• 50-99% of moderate head trauma victims have permanent injury.
• Motor Vehicle Crashes are primary cause.
• Falls for elderly and children
• High velocity missiles/blast injuries
• 30% have at least one significant concurrent injury.


Pathophysiology
• Primary brain injury
• Direct Trauma
• Involves bleeding, tearing, shearing, neuron damage
• Secondary brain injury
• Hypoxia, hypercapnea, hypotension, hyperglycemia, hypoglycemia, increased intracranial pressure, swelling, seizures

Head Injuries
• Scalp Lacerations
• Skull Fractures
• Concussions
• Contusions
• Intracranial Bleeding
• Cerebral Edema

Scalp Lacerations
• Rich blood supply
• Can cause hypovolemic shock
• Often deeper brain injury has occurred
• Direct pressure to control bleeding
• Do not apply excessive pressure
• Complete neurological exam

Skull Fractures
• Significant force has been applied to the skull.
• Injuries from bullets, blasts,blunt force, other penetrating objects.
• Risk of infection, if open skull fracture.
• X-ray or CT
• Deformity
• Skull fragments

Skull Fractures
• Raccoon Eyes• Indicates maxilofacial fractures around eyes
• Ecchymosis (Black eyes)
• Visual Acuity
• Eye bulges out (Exopthalmos)
• Eye sinks in (Enopthalmos)

Skull Fractures
• Battle’s sign• Associated with basilar skull fracture
• Blood accumulation behind one or both ears (forms bruising 12-24 hours later)
• Hemotympanum
• CSF drainage from ears or nose (never pack)
• Check extraocular movements

Concussion
• Temporary loss of brain function
• May result in loss of consciousness
• Confusion
• Amnesia
• Dizzyness
• Weakness

Concussion
• Coup- same side injury
• Contra-coup-opposite side injury
• Contusions may occur as the brain scrapes the inside of the skull• Bleeding, permanent injury, swelling, amnesia,
unconsciousness

Intracranial Bleeding
• Epidural Hematoma
• Subdural Hematoma
• Intracerebral Hemorrhage

Epidural Hematoma
• Occurs above the dura lining
• Occurs below the skull
• Most often arterial bleeding
• Develops rapidly
• Rapid deterioration of neurologic functions
• Lucid phase

Subdural Hematomas
• Occurs beneath the dura
• Occurs outside the brain
• Usually venous in nature
• Develops slowly
• Progressive loss of neurological function
• Patients may not remember blunt trauma

Intracranial Hemorrhage
• Bleeding occurs within the brain itself
• Caused by tearing, shearing of blood vessels
• Spinal Taps contraindicated due to increased swelling

Cerebral Edema
• Most common complication of head injury
• Aggravated by low oxygen levels
• Seizures increase oxygen consumption
• Causes increased intracranial pressure
• Normal ICP 10-15 mm

Cerebral Ischemia
• Headache
• Nausea and vomiting
• Amnesia for events before or after injury
• Altered level of consciousness
• Restlessness, drowsiness
• Changes in speech
• Loss of judgement

Intracranial Pressure
• Cerebral Perfusion Pressure (CPP)
• Mean Arterial Pressure (MAP)
• Autoregulation

Autoregulation
• An increase in mean arterial pressure leads to vasoconstriction of cerebral vessels.
• A decrease in mean arterial pressure leads to vasodilation of cerebral vessels.
• Hypoxia and Hypovolemia are the main causes of secondary brain injury.

Intracranial Pressure
• Cerebral perfusion must be adequate to prevent secondary brain injury.
• Prevention starts by treating shock.• Keep mean arterial pressure between 60 and 180
mm Hg.• One episode of hypotension significantly increases
morbidity and mortality. • Position patient to facilitate venous drainage.

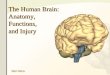
Monro-Kellie Doctrine

Glasgow Coma ScaleEYE OPENING
• Spontaneous
• To Voice
• To Pain
• None
4
3
2
1

Glasgow Coma Scale
VERBAL RESPONSE
• Oriented
• Confused
• Inappropriate Words
• Incomprehensible Words
• None
5
4
3
2
1

Glasgow Coma ScaleMOTOR RESPONSE
• Obeys Commands
• Localizes Pain
• Withdraws (pain)
• Flexion (pain)
• Extension (pain)
• None
6
5 4
3
2
1

Glasgow Coma Scale
• Predicts mortality
• Measures level of consciousness
• Motor component most sensitive subset
• Indicates improvement or deterioration
• GCS of 9-15 indicates mild to moderate injury
• GCS of 3-8 indicates severe head injury

Pupil Assessment
• Size
• Light Response
• Equal
• Compare

Posturing
• Decorticate- hands turn inward toward
• Decerebrate-hands turn outward
• Happens prior to herniation syndrome.

Treatment
• Prevent secondary injury
• Airway-oxygen and intubation if GCS < 8
• Treat shock-normotensive
• Hyperventilation is only indicated if patient shows signs of impending herniation
• Control bleeding from other injuries
• RAPID transport if possible

Treatment
• Continual assessment-pupils & GCS
• Treat seizures-increased oxygen consumption of the brain
• Watch for respiratory pattern changes-may indicate your patient is worsening.

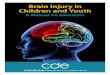
Management of Suspected Traumatic Brain Injury
P e rfo rm E nd o tra ch e a l In tu b a tion
Y e s
C o n tin u e T ra nsp o rt
N O
C o n tin u e T ra nsp o rt
S ed a tionP a ra lys is
O sm o th era pyC o n tro lle d H yp erve n tila t ion
Y e s
S ig n s o f inc re ase d IC P ?
C h e ck b lo o d g lu co se le ve l
T re a t S e izu res
V o lu m e resu scita t ion
In it ia te tra n sp o rt
C o n tro l E x te rna l H em o rrh a ge
A ss is t V e n tila t io ns
A p p ly o xyg enM a in ta in S p O 2
N o
G la sgo w C o m a S ca le< 8
S u spe c te d T B I

QUESTIONS ?