Embed Size (px)
DESCRIPTION
Bone loss following knee arthroplasty potential t
Citation preview

1 3
Arch Orthop Trauma SurgDOI 10.1007/s00402-014-1941-8
Knee RevISIOn SuRgeRy
Bone loss following knee arthroplasty: potential treatment options
Michele Vasso · Philippe Beaufils · Simone Cerciello · Alfredo Schiavone Panni
Received: 1 May 2013 © Springer-verlag Berlin Heidelberg 2014
Conclusions Modular augmentation may significantly reduce the need for allografting, whose complications appear to limit the long-term success of knee revisions.
Keywords Revision knee arthroplasty · Knee reconstruction · Bone loss · Augments · Tantalum · Allografts
Introduction
The optimal management of bone defects during revision total knee arthroplasty (TKA) remains controversial, espe-cially in case of large defects. Bone loss after TKA can make implant alignment and the establishment of a stable bone–implant interface extremely challenging. The vari-ability in size and location of bone defects has led to the development of a multitude of techniques aimed at restor-ing physical integrity of the knee and supporting prosthetic replacement: metal augments, metaphyseal tantalum cones and porous sleeves, morcellized or structural grafts, and spe-cial prosthetic components [1–3]. The knee surgeon should know all possible causes of bone loss following knee joint replacement, both to prevent and to manage them.
The purpose of this paper was to analyze the indications, the results and the complications of the potential treatment options used to manage bone loss within revision TKA. Furthermore, possible causes of bone loss after TKA were reviewed.
Etiology of bone loss
Several factors can be responsible for bone defects fol-lowing the failure of a knee arthroplasty: primitive cause
Abstract Introduction The management of bone loss is a crucial aspect of the revision knee arthroplasty. Bone loss can hin-der the correct positioning and alignment of the prosthetic components, and can prevent the achievement of a stable bone–implant interface. There is still controversy regarding the optimal management of knee periprosthetic bone loss, especially in large defects for which structural grafts, metal or tantalum augments, tantalum cones, porous metaphyseal sleeves, and special prostheses have been advocated. The aim of this review was to analyze all possible causes of bone loss and the most advanced strategies for managing bony deficiency within the knee joint reconstruction.Materials and methods Most significant and recent papers about the management of bone defects during revision knee arthroplasty were carefully analyzed and reviewed to report the most common causes of bone loss and the most effec-tive strategies to manage them.Results Modular metal and tantalum augmentation showed to provide more stable and durable knee revisions compared to allografts, limited by complications such as graft failure, fracture and resorption. Moreover, modular augmentation may considerably shorten operative times with a potential decrease of complications, above all infec-tion which has been frequently associated to the use of allografts.
M. vasso (*) · S. Cerciello · A. Schiavone Panni Department of Medicine and Science for Health, university of Molise, via Francesco De Sanctis, Campobasso, Italye-mail: [email protected]
P. Beaufils Department of Orthopedics and Trumatology, versailles “Andrè Mignot” Hospital, versailles Saint Quentin university, Rue de versailles 177, Le Chesnay, France

Arch Orthop Trauma Surg
1 3
of revision, mechanical loosening, chronic infection, wear debris-induced osteolysis, implant and cement removal, antibiotic spacer, spacer removal and delayed reimplanta-tion of the prosthesis.
Primitive cause of revision
Primitive failure of primary TKA may be directly respon-sible for bone loss, as it occurs because of a periprosthetic fracture or subsidence of one or both the prosthetic compo-nents. In these cases, bone loss often occurs regardless of a well-defined biological or mechanical status.
Mechanical loosening
Mechanical loosening represents the most frequent cause of failure of the modern TKAs [4, 5]. Mechanical loosen-ing following TKA may be potentially determined by com-ponent malalignment, prosthesis instability, patellofemoral disorders, and other minor causes. All these factors may produce knee periprosthetic bone loss by wear-induced osteolysis (due to an increased asymmetrical loading and the generation of shear stress), loosening and subsidence of the femoral and/or tibial components, and stress shielding. Moreover, sportive or lavorative activities involving squat-ting, and kneeling postures in daily activities represent risk factors for mechanical loosening of TKA [5].
Large numbers of wear particles detached from TKA trigger and perpetuate particle disease, as highlighted by progressive growth of inflammatory/granulomatous tis-sue around the joint cavity. An increased accumulation of osteoclasts at the bone–implant interface, impairment of osteoblast function, mechanical stresses and increased pro-duction of joint fluid contribute to bone resorption and sub-sequent loosening of the implant [6].
Chronic periprosthetic infections
Infection remains the second most common cause of TKA failure [5]. During chronic periprosthetic infections, cel-lular mechanisms of osteolysis can be determined by (1) the direct damage of infectious organisms and (2) the host inflammatory response. Infectious bacteria produce a wide variety of enzymes and toxins resulting in enzymatic deg-radation, activation of fibrinolytic activity, vascular dam-age and subsequent bone necrosis. Furthermore, bacterial endotoxins (lipopolysaccharides) exert powerful effects on a large variety of cells, including macrophages, neu-trophils and B lymphocytes [7]. As a result of this activa-tion, in addition to antibodies, host cells secrete a variety of cytokines such as interleukin-1 (IL-1), granulocyte and macrophage colonies stimulating factor (gM-CSF), tumor necrosis factor (TnF), and IL-6 [7]. Some of these
cytokines are mainly involved in maturation and activation of osteoclasts and macrophages, leading to osteolytic reac-tion and bone resorption that make the prosthesis unstable and needing revision [8].
Wear and osteolysis
Due to great improvements in implant and instrument design, in manufacturing processes, and in surgical tech-nique with expanding appreciation of the importance of appropriate sizing, soft tissue balancing and joint line recon-struction, polyethylene wear-induced osteolysis is no longer the main factor of knee periprosthetic bone loss [4]. How-ever, polyethylene wear remains a relatively frequent cause of failure in modern TKA [9, 10]. etiology of polyethyl-ene wear in knee replacement is multifactorial: prosthetic design, articular congruence, knee alignment, component fixation, third body wear, manufacturing and sterilization procedures, and thickness of the polyethylene itself [11].
The presence of articular polyethylene debris leads to an inflammatory response by macrophages and histiocytes, which induces activation of osteoclastic bone resorption, resulting in periprosthetic osteolysis and possible implant loosening [6, 12].
During metallosis following TKA, metal debris act simi-larly to polyethylene debris. Metal debris cause the release of cytokines by inflammatory cells (including IL-1, IL-6, IL-8, TnF), resulting in chronic synovitis, osteoclastic bone resorption, and periprosthetic osteolysis. A synergis-tic action has been hypothesized between metal debris and polyethylene debris in the activation of the macrophage response, with an increase in cytokine release [6, 13].
Implant and cement removal
Prosthesis removal represents a further source of bone loss. In the presence of a cementless prosthesis, removal of a stable implant could cause significant bone loss, while removal of a loosed implant generally preserves much more bone stock. In the presence of a cemented prosthe-sis, implant removal is usually easier because a detachment usually occurs at the cement–metal interface. However, removal of the bone cement can represent an additional source of bone loss.
Once an infected prosthesis is removed, removal of all necrotic and infected bone tissues is essential to eradicate infection: therefore, accurate debridement may cause fur-ther bone loss.
Antibiotic-loaded spacer
Two-stage reimplantation involves the use of antibiotic-loaded cement spacers to eradicate infection and preserve

Arch Orthop Trauma Surg
1 3
joint space. These spacers release microparticles of cement into the joint, stimulating an inflammatory response of the synovial membrane, with consequent damage to bone and soft tissues. Moreover, the shear forces that are gener-ated at the cement–bone interface during knee flexion are responsible for additional erosion by friction of the host bone. This occurs especially when the spacers (almost exclusively the static spacers) are not perfectly shaped to bone profiles of the distal femur and/or proximal tibia [14]. Significant bone loss of the metaphyseal spongiosa can also occur after migration of an undersized static spacer. A degree of osteopenia is finally caused by the partial immo-bilization of the limb, which is necessary in patients treated with static spacers [15, 16].
More recent articulating spacers allow weight bearing and knee motion during the period following prosthesis removal, thus reducing rigidity and osteopenia before reim-plantation [17–19].
Spacer removal and prosthesis reimplantation
During the second phase of a two-stage reimplantation, bone loss is caused by spacer removal, and by bone resec-tions necessary for placement of the new prosthesis.
Removal of an articulating spacer is generally a simple procedure: it does not require a dedicated instrumentation and allows preservation of bone stock more than static spacers. Once the spacer is removed, articular surfaces have to be thoroughly debrided, with further bone loss.
As already mentioned, a variable amount of bone is sac-rificed as the result of resections necessary for implantation of the revision prosthesis. Wedges, augments and cones require further bone resection to be positioned. Finally, use of stem extensions could require debridement and curettage of the femoral and/or tibial endomedullary canals.
Classification of the knee periprosthetic bone defects
engh et al. [20] proposed the classification of the knee bone defects according to the “Anderson Orthopaedic Research Institute” (AORI). This classification defines the extent and severity of the knee bone loss on the distal fem-oral side (F1, F2, F3) and on the proximal tibial side (T1, T2, T3). Type 1 defects (F1 or T1) are characterized by intact metaphyseal segments, with only mild defects of the spongiosa, no subsidence of the components and absence of osteolysis. Type 2 defects present damaged metaphyseal bone segments in one (F2A or T2A) or both (T2B or F2B) femoral and/or tibial condyles. In particular, on the femoral side subsidence of the components or osteolysis is distal to the epicondyles; on the tibial side, subsidence or osteolysis is up to or below the head of the fibula. Type 3 defects (F3
or T3) include major defects of the metaphyseal segments, which are generally associated with partial or total insuf-ficiency of the ligamentous structures. On the femoral side, subsidence or osteolysis is proximal to the epicondyles, thus being absent; on the tibial side, subsidence or osteoly-sis is distal to the tibial tuberosity, often with serious prob-lems of the knee extensor mechanism.
The AORI classification does not distinguish between contained and non-contained defects. Contained or cavitary defects have an intact cortical ring surrounding the area of bone loss, while non-contained or segmental defects are more peripheral and do not have a surrounding intact corti-cal ring.
Historically, Rand [21] classified the bone defects in relation to their symmetry, position and extent. An under-sized tibial component could cause a symmetrical defect linked to the subsidence of the middle part of the tibia. On the other hand, an asymmetrical defect can be caused by the angular mobilization of the tibial component, resulting in an asymmetrical bone loss of the tibial plate. The loca-tion of a bone defect can be defined as central or peripheral relative to the integrity of the cortex. On the tibial side, a central defect is usually due to the mobilization of an old surface component, which leaves a peripheral border of bone intact. A peripheral defect is associated with an angu-lar deformity in the primary arthroplasty and is usually pos-terior and medial in a varus knee. On the femoral side, the bone loss associated with revision surgeries is distal, poste-rior, or both. The extent of bone defects can be divided into four types: minimum (type I), moderate (type II), extensive (type III), and massive cavitary (type Iv). The amount of bone loss has to be evaluated after tibial and femoral resec-tions. A minimum defect involves less than 50 % of a sin-gle condyle, with a depth of less than 5 mm. A moderate defect involves an area of 50–70 % of a single condyle, with a depth of 5–10 mm. An extensive defect involves more than 70 % of a condyle, with a depth greater than or equal to 10 mm. Finally, a massive cavitary defect involves the total disruption of one or both condyles and can be of two types based on the presence (a) or absence (b) of an intact peripheral rim.
Management of bone loss
For small, cavitary, type 1 defects according to AORI clas-sification [20], cement, morcellized autografts and bone substitutes can be sufficient. For larger, segmental, type 2 or 3 defects, impaction or structural grafts, augments, tan-talum cones, metaphyseal sleeves, and special prostheses have been advocated [1, 2, 22–26].
Bone grafts have been widely used in revision TKA as being well suited to adapt to bone profiles without

Arch Orthop Trauma Surg
1 3
requiring excessive bone resections, and to transfer loads to the underlying bone in a physiological manner. Autologous grafts are generally used for the management of mild, con-tained defects, and are used mainly in the form of cancel-lous bone [27]. For larger defects, impaction or structural allografts are needed. The advantages of structural allo-grafts include relative cost-effectiveness, versatility, poten-tial for bone stock restoration and potential for ligamentous reattachment. However, many disadvantages have been associated to the use of structural allografts: risk of dis-ease transmission, nonunion, malunion, collapse or resorp-tion of the graft [25]. Further disadvantages of structural allografts are their availability and meticulous preparation required to maximize surface contact between the allograft and the host-bone interfaces [28]. Recently, impaction allo-grafts have been advocated to address variable and irregular defects that are commonly encountered in knee revisions; moreover, impaction allografts could incorporate into host bone and, successively, remodel and function like native bone [29]. However, impaction allografting remains a time- consuming and a technically demanding procedure [29]. Finally, a higher risk of periprosthetic infection has been reported when using allografts [30].
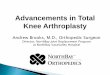
Metal augments have been introduced in knee revision surgery for the management of segmental bone defects. Augments offer several advantages as compared to allo-grafts: extensive modularity, quick and easy use with decreased surgical time, great availability, and fewer com-plications [22]. Modular metal and tantalum augmentation allow a surgeon to produce a custom implant, re-establish component levels (and therefore the anatomic joint line), restore limb alignment, and balance soft tissues. Moreo-ver, modular augmentation presents excellent biomechani-cal properties, require minimal bone resection, and allow immediate mobilization and loading [2]. Tibial augments are either wedge or blocks shaped. Hemiwedges and hemi-blocks can be used to fill small and asymmetric peripheral defects, whereas full wedges and blocks can be used to cor-rect axial alignment beneath the tibial tray or to substitute for more extensive cortical bone loss elevating the tibial baseplate (Fig. 1). Therefore, tibial augments can assist the surgeon to recreate a flat platform, restore anatomic joint line, and balance extension and flexion spaces.
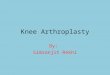
Femoral augmentation has received less attention in the literature. Current knee systems include femoral augments of variable thicknesses for the medial and lateral condyles, both distally and posteriorly or in combination. Poste-rior femoral augments are particularly useful in restoring proper anteroposterior dimension of the femoral com-ponent, achieving the correct femoral component (extra)rotation (Fig. 2), optimizing mediolateral bone coverage, and addressing the extension-flexion mismatch as impact-ing flexion gap. Distal femoral augments are useful in
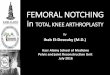
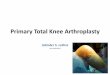
re-establishing the anatomic joint line, therefore impacting extension gap. Trabecular tantalum augmentation has been recently introduced in revision TKA for the management of massive segmental bone defects. Trabecular tantalum has been proposed to allow the restoration of bone stock by promoting osseointegration; this may prove extremely ben-eficial for younger patients, in whom a further revision is likely [31, 32]. Tantalum cones can help restore the struc-tural stability of the proximal tibial and/or distal femoral metaphysis with severe type 2 or 3 bone defects (Fig. 3). Cones can be used in combination with other metal aug-ments, made of tantalum or other materials [2, 31]. Cones are placed in direct contact with the host bone; prosthetic components, eventually augmented, are then cemented on the cones and on the metaphyseal bone (Fig. 4).
Press-fit metaphyseal sleeves represent a relatively new strategy to manage structural defects in revision knee arthroplasty. Taking advantage of biological fixation of osseous integration, these components avoid potential com-plications and the potential disease transmission of allo-grafts, while providing a stabile scaffold for joint recon-struction. Porous metaphyseal sleeves have been advocated primarily for large tibial defects [1]. When the sleeve is osseointegrated, it carries a portion of the axial load, effec-tively protecting the epiphyseal fixation and improving the rotational stability of the construct [33]. The primary dif-ference between tantalum cones and porous sleeves is that
Fig. 1 Full tibial blocks can be used for the management of exten-sive cortical bone loss. elevating the tibial baseplate helps to restore anatomic joint line and reduces the polyethylene thickness, therefore decreasing stresses at the insert locking mechanism

Arch Orthop Trauma Surg
1 3
the interface of the sleeve with the implant is created via a Morse-tapered junction rather than with cement. A well-osseointegrated sleeve or cone would more effectively resist rotational stress than a cylindrical stem alone [33].
Modular stems can provide correct component position-ing, enhance fixation, decrease stress at the bone–implant interface in presence of severe and asymmetric bone loss [34]. elevated stress at the interface occurs when the col-laterals are insufficient or absent, the bone–prosthesis inter-face is reduced, metal augments are used, and osteotomy of the tibial tuberosity is performed. When bone stock is quite
preserved, uncemented stems are preferred. The length and diameter of the extension depend on the integrity of the residual bone and the dimensions of the intramedullary
Fig. 2 Segmental defect of the postero-lateral femoral condyle a should be managed with a metal augment, b to avoid intrarotation of the femoral component and potential patellofemoral maltracking and instability
Fig. 3 Massive metaphyseal tibial and femoral defects can be recon-structed with highly porous tantalum cones. Tantalum cones have been developed to prevent the incidence of nonunion and resorption associated with structural allograft reconstructions
Fig. 4 Tantalum cones, with their potential for bony ingrowth, are placed in direct contact with the host bone; the augmented prosthetic components are then cemented onto the cones

Arch Orthop Trauma Surg
1 3
canal. Offset stems can assist with implant alignment when the metaphyseal portion of the bone may not be directly centered over the diaphysis [35]. Offset stems can prevent mediolateral or anteroposterior components from protrud-ing, enable achievement of the correct mechanical axis, balance the spaces in extension and flexion through the transfer of the components.
Materials and methods
The primary research question of this review was to deter-mine the outcome of revision TKAs in which different treatment options for bone loss management were used. Outcomes of interest were revision implant survivorship, failures of the different devices alternatively used, any complication of the revision or of the devices used. An advanced PubMed search was performed of the revision knee arthroplasty literature. The search terms ‘‘revision knee arthroplasty OR replacement”, “revision total knee”, “bone loss OR defect”, ‘‘augment’’, “wedge”, “stem”, ‘‘tantalum cones’’, “sleeve”, “allograft”, and “bone graft-ing” were used. Furthermore, the reference lists of retrieved publications were checked manually for additional studies that potentially met the inclusion criteria but had not been found by the electronic search. Two investigators (M.v. and S.C.) independently reviewed the literature to identify rel-evant articles for this review. The reviewers independently applied the criteria described above and below to the full text of these articles to select articles for inclusion in this review. An article was included if it represented a signifi-cant study in which the outcome of the bone loss manage-ment within revision TKA was reported. Studies involving the treatment options for type 2 and/or 3 AORI bone defects in revision TKA were included. Review articles, expert opinions, surgical techniques, and abstracts from scientific meetings were excluded. Duplicates were excluded, as well as studies with less than 2 years of follow-up, finally result-ing in 19 articles for the revision TKA. no relevant ran-domized or comparative studies were found, so that only Level Iv, therapeutic case-series studies were included in this review.
Results
The results of previous studies of revision TKA using dif-ferent devices to manage type 2 and 3 AORI bone defects are summarized in Table 1. Two authors (M.v. and S.C.) extracted information from 19 revision TKA studies inde-pendently. Informations extracted included study design, number of knee revisions, bone loss treatment option, aver-age follow-up, percentage of implant survivorship, and
complications. non-progressive radiolucent lines around implant or devices used for the management of bone loss were not reported, not influencing clinical and functional results in any study.
The use of allografts has shown higher incidence of complications, and lower survivorship of the knee revisions (Table 1). naim et al. [29] prospectively studied 11 patients with large tibial defects treated with impaction bone graft-ing. none of the patients required secondary procedures or further revisions. All radiographs showed incorporation and remodeling of the graft. The only complication was a superficial dysesthesia around the operative scar. However, mean follow-up was only 2 years. Steens et al. [36] retro-spectively analyzed 34 revision TKAs performed using impaction grafting. The average follow-up was 4 years. In five knees, there were no clear radiographic signs of incorporation of the graft. Five other patients had compli-cations due to aseptic loosening of their prostheses with radiographic failure of the graft, leading to a periprosthetic fracture in two cases. Lotke et al. [37] prospectively stud-ied the results of 48 consecutive revision TKAs with sub-stantial bone loss treated with impaction allograft. Average follow-up was 3.8 years. There were six complications: two periprosthetic fractures, two deep infections, and two patel-lar clunk syndromes.
Concerning the use of structural allografts in revi-sion TKA, ghazavi et al. [38] reported only 67 % survi-vorship at 5 years in 30 patients. Backstein et al. [39] had one of the largest cohorts with 61 patients. The survival rate at 5.4 years was 85.2 %, but the infection rate was 6.5 %. Clatworthy et al. [40] prospectively followed 52 revision TKAs with 66 structural grafts. Five knees had graft resorption, resulting in implant loosening. Four knee replacements failed because of infection, and two knees had nonunion between the host bone and the allograft. The survival rate of the allografts was 72 % at 10 years. Bau-man et al. [41] reviewed 65 revisions in which large bone defects were managed with bulk allografts. They reported a 10-year revision survivorship of 76 %. Sixteen patients (22.8 %) had failed reconstructions: eight failures of the 16 were secondary to allograft failure, three were secondary to failure of a component not supported by allograft, and five were secondary to infection.
Modular metal and tantalum augmentation has provided more stable and durable knee reconstructions, with a lower incidence of complications (Table 1). Historically, Rand [21] reviewed 28 knees in 25 patients reporting good or excellent results in 100 % of patients using metal augmen-tation in revision TKA. In 22 knees with modular metal wedges to augment tibial bone stock deficiency, Brand et al. [42] reported no failures and no loosening of tibial components after a mean of 3 years. no patient underwent re-revision surgery. Haas et al. [43] reported an 8-year

Arch Orthop Trauma Surg
1 3
Tabl
e 1
The
res
ults
of
prev
ious
stu
dies
of
revi
sion
TK
A u
sing
dif
fere
nt d
evic
es to
man
age
type
2 a
nd 3
AO
RI
bone
def
ects
Ref
eren
ces
Stud
y ty
peR
evis
ions
Tre
atm
ent o
ptio
nA
vera
ge F
u (
year
s)Im
plan
t sur
vivo
rshi
p (%
)C
ompl
icat
ions
nai
m a
nd T
oms
[29]
Pros
pect
ive
case
-ser
ies
11Im
pact
ion
graf
ting
210
0D
yses
thes
ia a
roun
d th
e op
erat
ive
scar
Stee
ns e
t al.
[36]
Ret
rosp
ectiv
e ca
se-s
erie
s34
Impa
ctio
n gr
aftin
g4
85A
sept
ic lo
osen
ing
with
fai
lure
of
the
graf
t (14
.7 %
), p
erip
rost
hetic
fra
ctur
e (5
.9 %
)
Lot
ke e
t al.
[37]
Pros
pect
ive
case
-ser
ies
48Im
pact
ion
graf
ting
3.8
88In
fect
ion
(4.2
%),
per
ipro
sthe
tic f
ract
ure
(4.2
%),
pat
ella
r cl
unk
synd
rom
e (4
.2 %
)
gha
zavi
et a
l. [3
8]R
etro
spec
tive
case
-ser
ies
30St
ruct
ural
allo
graf
ts5
67In
fect
ion
(10
%),
loos
enin
g of
the
tibia
l com
pone
nt (
6.6
%),
fra
ctur
e of
the
graf
t (3.
3 %
), n
onun
ion
at th
e al
logr
aft–
host
junc
tion
(3.3
%)
Bac
kste
in e
t al.
[39]
Ret
rosp
ectiv
e ca
se-s
erie
s61
Stru
ctur
al a
llogr
afts
5.4
85.2
Infe
ctio
n (6
.5 %
)
Cla
twor
thy
et a
l. [4
0]Pr
ospe
ctiv
e ca
se-s
erie
s52
Stru
ctur
al a
llogr
afts
1072
Infe
ctio
n (7
.7 %
), n
onun
ion
at th
e al
logr
aft–
host
junc
tion
(3.9
%)
Bau
man
et a
l. [4
1]R
etro
spec
tive
case
-ser
ies
65B
ulk
allo
graf
ts10
76A
llogr
aft f
ailu
re (
12 %
), f
ailu
re o
f a
com
pone
nt n
ot s
uppo
rted
by
allo
graf
t (4
.6 %
), in
fect
ion
(7.7
%)
Ran
d [2
1]R
etro
spec
tive
case
-ser
ies
28M
etal
wed
ges
2.3
100
non
e
Bra
nd e
t al.
[42]
Pros
pect
ive
case
-ser
ies
22M
odul
ar m
etal
wed
ges
310
0n
one
Haa
s et
al.
[43]
Ret
rosp
ectiv
e ca
se-s
erie
s67
Mod
ular
met
al w
edge
s an
d au
gmen
ts
pres
s-fit
mod
ular
ste
ms
893
non
e
Wer
le e
t al.
[44]
Ret
rosp
ectiv
e ca
se-s
erie
s5
Lar
ge (
30 m
m)
met
al d
ista
l fem
oral
au
gmen
ts3.
110
0n
one
Pate
l et a
l. [4
5]Pr
ospe
ctiv
e ca
se-s
erie
s79
Mod
ular
met
al a
ugm
ents
792
Ase
ptic
loos
enin
g (7
.6 %
), in
fect
ion
(2.5
%)
Woo
d et
al.
[46]
Ret
rosp
ectiv
e ca
se-s
erie
s13
5M
etal
aug
men
tatio
n an
d pr
ess-
fit
mod
ular
ste
ms
587
Ase
ptic
loos
enin
g (1
.4 %
), in
fect
ion
(1.4
%)
Pann
i et a
l. [3
5]Pr
ospe
ctiv
e ca
se-s
erie
s38
Met
al a
ugm
ents
, por
ous
tant
alum
co
nes
and
pres
s-fit
mod
ular
ste
ms
792
Inst
abili
ty (
2.6
%),
infe
ctio
n (5
.2 %
)
Men
eghi
ni e
t al.
[47]
Pros
pect
ive
case
-ser
ies
15Po
rous
tant
alum
con
es2.
810
0n
one
How
ard
et a
l. [3
1]Pr
ospe
ctiv
e ca
se-s
erie
s24
Poro
us ta
ntal
um c
ones
2.7
100
non
e
Lac
hiew
icz
et a
l. [3
2]R
etro
spec
tive
case
-ser
ies
27Po
rous
tant
alum
con
es a
nd p
ress
-fit
mod
ular
ste
ms
3.3
92A
sept
ic lo
osen
ing
(3.7
%),
infe
ctio
n (3
.7 %
), f
emor
al s
haft
fra
ctur
e (3
.7 %
)
Rao
et a
l. [3
]Pr
ospe
ctiv
e ca
se-s
erie
s26
Poro
us ta
ntal
um c
ones
and
pre
ss-fi
t m
odul
ar s
tem
s3
100
non
e
Ale
xand
er e
t al.
[1]
Ret
rosp
ectiv
e ca
se-s
erie
s30
Poro
us ti
tani
um ti
bial
sle
eves
2.7
97In
fect
ion
(3.3
%),
inst
abili
ty (
3.3
%)

Arch Orthop Trauma Surg
1 3
survivorship of 92 % on 67 revisions for aseptic indica-tions, performed with use of metal wedges and augments, and not-cemented stems. Werle et al. [44] assessed the use of large metal distal femoral augments to compensate for severe bone deficiencies in revision TKA. Clinical and functional scores significantly improved after implanta-tion of femoral components with 30-mm distal femoral augments. There was no radiographic evidence of loosen-ing, and no implants had been revised at mean 37-month follow-up. Patel et al. [45] described the results of type 2 bone defects treated with modular metal augments in 79 revision TKAs. The survival of the components was 92 % at 11 years. The presence of non-progressive radiolucent lines around the augment in 14 % of knees was not associ-ated with poorer knee scores, range of movement, survival of the component, or type of insert used. Wood et al. [46] described the results of 135 revision TKAs performed for both septic and aseptic failures. The Kaplan–Meier sur-vival rate after 12 years was 87 % using press-fit modular stems and metal augmentation. Panni et al. [35] recently reported on 38 knee revisions, satisfactorily managed with metal augments, tantalum cones and stem extension. no allograft was used. The median follow-up was of 7 years, therefore supporting the hypothesis that modular augmen-tation could provide stable and durable revision total knee arthroplasties. All metal augments and all tantalum cones appeared well fixed radiographically at the final follow-up, with no evidence of complications related to the modular augmentation. In particular, on the immediate postoperative radiographs, all nine porous cones appeared to be closely apposed to the adjacent host bone of the proximal tibial and distal femoral metaphysis.
Meneghini et al. [47] reported on porous tantalum cones for the management of large tibial bone loss at 15 revision TKAs. Patients were followed for an average of 34 months. At the last follow-up, all 15 cones showed evidence of osse-ointegration with reactive osseous trabeculation at points of contact with the tibia. There was no evidence of loosening or migration of any of these tibial reconstructions at final follow-up. Howard et al. [31] reported on tantalum cones for the treatment of severe femoral type 3 bone loss at 24 knee revisions. The patients were followed for an average of 33 months. All femoral cones appeared well fixed radio-graphically. Lachiewicz et al. [32] retrospectively reviewed 27 patients who had 33 tantalum cones implanted during 27 revision TKAs performed for infection, aseptic loosening, and wear osteolysis. The maximum follow-up was 7 years. One knee with two cones was removed for infection. All but one cone showed osseointegration. Clinical and func-tional scores significantly improved at final follow-up. Recently, Rao et al. [3] reported the results of 26 revision TKAs using 29 trabecular metal cones. Patients were fol-lowed for a mean of 36 months (24–49). no radiolucent
lines suggestive of loosening were seen around the trabecu-lar metal cones, and by 1 year all the radiographs showed good osteointegration. There was no evidence of any col-lapse or implant migration. no complication was reported.
Alexander et al. [1] retrospectively reviewed 30 revision TKAs, performed using a porous titanium tibial sleeve. The mean follow-up was 2.7 years. Six patients had a repeat operation though none were sleeve related. Only an implant was revised. All radiographs at final follow-up showed well-fixed components with osseous ingrowth. Seven patients had end-of-stem pain, four of which resolved.
Discussion
The main finding of this review was that modular metal and tantalum augmentation showed to provide more stable and durable revision TKAs compared to allografts, limited by complications as infection, fracture and resorption. The clinical literature to support the impaction bone allograft technique is still weak. Since 2006, impaction grafting has been used for contained and uncontained large defects in primary and revision TKA. This option has shown good versatility in short follow-ups, although being time con-suming and technically demanding [29]. Moreover, compli-cations as infection and graft failure have been frequently reported [36], which could limit the long-term success of this procedure.
Structural allografts have been primarily used for mas-sive, type 2 and 3 defects [48–50]. Concerns exist about the long-term results of structural allografts due to their possi-ble complications, namely, graft nonunion, collapse, resorp-tion and infection [40, 51]. Structural allografts remain a relative cost-effectiveness option that may be reserved for patients with lesser functional demand to decrease the risk of collapse or fracture of allograft before its complete incor-poration into host bone [30, 49]. Structural allografts could be suitable in younger patients who present high rates of union while restoring bone stock for future revisions. Older patients who need immediate ability to weight bear and mobilize are not good candidates to allograft reconstruction. The use of structural allografts could be limited in septic revision since a higher risk of periprosthetic infection has been reported when using allografts [30, 33, 40, 49]. Since allografts need a well-vascularized metaphyseal host bone to obtain a proper incorporation and remodeling and avoid early resorption, the use of allografts could be limited in large uncontained metaphyseal defects [33]. Moreover, graft disincorporation and resorption could depend on the sterili-zation process, which may compromise tissue biology and biomechanics of allografts [49]. Finally, oversized allografts could be complicated by altered vascularization leading to graft fracture or early resorption [24, 48].

Arch Orthop Trauma Surg
1 3
Modular augmentation (metal and tantalum) may signifi-cantly reduce the need for allografting, whose complications appear to limit the long-term success of the revision TKAs. The major concerns with structural allografts are graft resorption, mechanical failure and infection, along with the considerable time and surgical skill required to obtain good host–allograft interface [33]. Metal augmentation and tanta-lum cones may simplify the knee joint reconstruction, mak-ing it more reproducible due to their extensive modularity associated to quick and easy use. Moreover, modular aug-mentation may considerably shorten operative times with a potential decrease of complications, above all infection [32]. The coefficient of friction of porous tantalum is high, allowing for a good primary implant stability and, therefore, for immediate postoperative weight-bearing. The potential for osteointegration of porous tantalum could favor its use in younger patients with higher functional demand [31, 32]. Data also suggest that tantalum surfaces increase host white blood cell activation and lower bacterial fixation, possibly decreasing the risk of infection and therefore being suitable in septic revisions [32]. Finally, modular augments and tan-talum cones, with their excellent biomechanical properties, could provide a well-functioning and durable knee joint reconstruction also in the presence of severe large bone defects, both in young and older patients [49]. Although the clinical results using the metal augments are excellent, con-cerns could exist about the use of augments relate to poten-tial mid-term bone loss and fretting, or dissociation of the modular components. Bone loss could occur because the use of augments does not involve restoration of bone stock, and may require further resection of bone to accommodate the component. use of the tantalum cones in the setting of revision knee arthroplasty could be potentially associated with all the usual complications that can occur in these dif-ficult cases, including mechanical failure of the cones or the prosthesis, aseptic loosening, instability and infection. Metal augments such as tantalum cones may require fur-ther bone resection too, needed to get an optimized fit of the cone. Finally, the cost of these devices may limit their availability and use in many countries which might not even have access to all these new technologies [32, 33].
Recently, porous-coated metaphyseal sleeves have been introduced to address these situations and have shown a promising early outcome. Porous sleeves have been intro-duced, in alternative to the tantalum cones, for the manage-ment of severe metaphyseal bone defects, demonstrating osseous ingrowth and presenting minimal complications, and providing stable construct with biologic fixation [1]. The popularity of the porous sleeves and tantalum cones has been driven by the efficiency of obtaining align-ment while managing the defect and by the opportunity to achieve non-cemented metaphyseal fixation. However, both metaphyseal sleeves and cones incorporate with host bone
and are attached to the prosthesis by a mechanical interface or cement, so that concerns persist regarding stress shield-ing and difficulty of removal [2, 33].
Conclusions
The management of bone defects is a crucial aspect of revi-sion TKA. Bone loss can hinder the correct positioning and alignment of the prosthetic components, and can prevent the achievement of a stable bone–implant interface. Knee surgeon should know all possible causes of periprosthetic bone loss and all techniques available to manage it during a knee joint reconstruction.
The best management of severe type 2 and 3 bone defects following TKA is still debating. Although time consuming and technically high demanding, the use of allografts remains a good and cost-effectiveness solution for patients with a quite long life expectancy and lower functional demand. The risk of graft failure, resorption and infection limit the use of allografts for contained type 2 or asymmetrical type 3 defects in aseptic revisions.
Modular metal and tantalum augmentation could reduce the need for bone allografting, whose limitations and com-plications appear to limit the long-term success of rTKAs. Metal augments, tantalum cones and porous sleeves (dif-ferent in shape and size) could help the surgeon to man-age any type of bone loss, contained or uncontained type 2 and 3 defects, providing stable and durable knee joint reconstruction. The potential for osteointegration of tan-talum cone and porous sleeves makes these devices suit-able for the use in younger patients with high functional demand. Moreover, the primary stability and excellent biomechanical properties of modular metal augmentation allow immediate mobilization and full weight bearing in older patients. Finally, the decreased infection rate and the association with antibiotic bone cement of the modu-lar augmentation make it selective in septic knee revisions. The major concerns of metal augmentation are certainly represented by elevated costs and difficult removal at re-revision.
Conflict of interest none.
References
1. Alexander ge, Bernasek TL, Crank RL, Haidukewych gJ (2013) Cementless metaphyseal sleeves used for large tibial defects in revision total knee arthroplasty. J Arthroplast 28:604–607
2. Huten D (2013) Femorotibial bone loss during revision total knee arthroplasty. Orthop Traumatol Surg Res 99(1 Suppl):S22–S33
3. Rao BM, Kamal TT, vafaye J, Moss M (2013) Tantalum cones for major osteolysis in revision knee replacement. Bone Joint J 95:1069–1074

Arch Orthop Trauma Surg
1 3
4. Dalury DF, Pomeroy DL, gorab RS, Adams MJ (2013) Why are total knee arthroplasties being revised? J Arthroplast 28(8 Suppl):120–121
5. Kasahara y, Majima T, Kimura S, nishiike O, uchida J (2013) What are the causes of revision total knee arthroplasty in Japan? Clin Orthop Relat Res 471:1533–1538
6. gallo J, goodman SB, Konttinen yT, Wimmer MA, Holinka M (2013) Osteolysis around total knee arthroplasty: a review of pathogenetic mechanisms. Acta Biomater 9:8046–8058
7. Wiggers eC, Johnson W, Tucci M, Benghuzzi H (2011) Biochem-ical and morphological changes associated with macrophages and osteoclasts when challenged with infection—biomed 2011. Biomed Sci Instrum 47:183–188
8. Chen J, Cui y, Li X, Miao X, Wen Z, Xue y, Tian J (2013) Risk factors for deep infection after total knee arthroplasty: a meta-analysis. Arch Orthop Trauma Surg 133:675–687
9. goldvasser D, Marchie A, Bragdon LK, Bragdon CR, Weiden-hielm L, Malchau H (2013) Incidence of osteolysis in total knee arthroplasty: comparison between radiographic and retrieval analysis. J Arthroplast 28:201–206
10. Kendrick BJ, Simpson DJ, Kaptein BL, valstar eR, gill HS, Murray DW, Price AJ (2011) Polyethylene wear of mobile-bear-ing unicompartmental knee replacement at 20 years. J Bone Joint Surg 93:470–475
11. Zeng y, Shen B, yang J, Zhou ZK, Kang PD, Pei FX (2013) Is there reduced polyethylene wear and longer survival when using a mobile-bearing design in total knee replacement? A meta-anal-ysis of randomised and non-randomised controlled trials. Bone Joint J 95:1057–1063
12. Lachiewicz PF, geyer MR (2011) The use of highly cross-linked polyethylene in total knee arthroplasty. J Am Acad Orthop Surg 19:143–151
13. Schiavone Panni A, vasso M, Cerciello S, Maccauro g (2011) Metallosis following knee arthroplasty: a histological and immunohistochemical study. Int J Immunopathol Pharmacol 24:711–719
14. Citak M, gessmann J, Fehmer T, Russe O, Schildhauer TA, Seybold D (2011) Two-stage revision of infected total knee arthroplasty using a distraction spacer. Technol Health Care 19:167–171
15. Johnson AJ, Sayeed SA, naziri Q, Khanuja HS, Mont MA (2012) Minimizing dynamic knee spacer complications in infected revi-sion arthroplasty. Clin Orthop Relat Res 470:220–227
16. Romanò CL, gala L, Logoluso n, Romanò D, Drago L (2012) Two-stage revision of septic knee prosthesis with articulating knee spacers yields better infection eradication rate than one-stage or two-stage revision with static spacers. Knee Surg Sports Traumatol Arthrosc 20:2445–2453
17. nettrour JF, Polikandriotis JA, Bernasek TL, gustke KA, Lyons ST (2013) Articulating spacers for the treatment of infected total knee arthroplasty: effect of antibiotic combinations and concen-trations. Orthopedics 36:19–24
18. Rogers BA, Middleton FR, Shearwood-Porter n, Kinch S, Roques A, Bradley nW, Browne M (2011) Does cyclical load-ing affect the elution of antibiotics from articulating cement knee spacers? J Bone Joint Surg 93:914–920
19. Silvestre A, Almeida F, Renovell P, Morante e, López R (2013) Revision of infected total knee arthroplasty: two-stage reimplan-tation using an antibiotic-impregnated static spacer. Clin Orthop Surg 5:180–187
20. engh gA, Ammeen D (1998) Classification and preopera-tive radiographic evaluation: knee. Orthop Clin north Am 29:205–217
21. Rand JA (1991) Bone deficiency in total knee arthroplasty: use of metal wedge augmentation. Clin Orthop Relat Res 271:63–71
22. Daines BK, Dennis DA (2013) Management of bone defects in revision total knee arthroplasty. Instr Course Lect 62:341–348
23. gudnason A, Milbrink J, Hailer nP (2011) Implant survival and outcome after rotating-hinge total knee revision arthro-plasty: a minimum 6-year follow-up. Arch Orthop Trauma Surg 131:1601–1607
24. Kuchinad RA, garbedian S, Rogers BA, Backstein D, Safir O, gross Ae (2011) The use of structural allograft in primary and revision knee arthroplasty with bone loss. Adv Orthop. doi:10.4061/2011/578952
25. Schmitz HC, Klauser W, Citak M, Al-Khateeb H, gehrke T, Ken-doff D (2013) Three-year follow up utilizing tantal cones in revi-sion total knee arthroplasty. J Arthroplast 28:1556–1560
26. vasso M, Beaufils P, Schiavone Panni A (2013) Constraint choice in revision knee arthroplasty. Int Orthop 37:1279–1284
27. Hanna SA, Aston WJ, de Roeck nJ, gough-Palmer A, Powles DP (2011) Cementless revision TKA with bone grafting of osse-ous defects restores bone stock with a low revision rate at 4 to 10 years. Clin Orthop Relat Res 469:3164–3171
28. Hongvilai S, Tanavalee A (2012) Review article: management of bone loss in revision knee arthroplasty. J Med Assoc Thai 95(Suppl 10):S230–S237
29. naim S, Toms AD (2013) Impaction bone grafting for tibial defects in knee replacement surgery. Results at two years. Acta Orthop Belg 79:205–210
30. Hilgen v, Citak M, vettorazzi e, Haasper C, Day K, Amling M, gehrke T, gebauer M (2013) 10-year results following impaction bone grafting of major bone defects in 29 rotational and hinged knee revision arthroplasties: a follow-up of a previous report. Acta Orthop 84:387–391
31. Howard JL, Kudera J, Lewallen Dg, Hanssen AD (2011) early results of the use of tantalum femoral cones for revision total knee arthroplasty. J Bone Joint Surg Am 93:478–484
32. Lachiewicz PF, Bolognesi MP, Henderson RA, Soileau eS, vail TP (2012) Can tantalum cones provide fixation in complex revi-sion knee arthroplasty? Clin Orthop Relat Res 470:199–204
33. Haidukewych gJ, Hanssen A, Jones RD (2011) Metaphyseal fixation in revision total knee arthroplasty: indications and tech-niques. J Am Acad Orthop Surg 19:311–318
34. Beckmann J, Lüring C, Springorum R, Köck FX, grifka J, Tin-gart M (2011) Fixation of revision TKA: a review of the litera-ture. Knee Surg Sports Traumatol Arthrosc 19:872–879
35. Panni AS, vasso M, Cerciello S (2012) Modular augmentation in revision total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-012-2258-1
36. Steens W, Loehr JF, Wodtke J, Katzer A (2008) Morselized bone grafting in revision arthroplasty of the knee: a retrospec-tive analysis of 34 reconstructions after 2–9 years. Acta Orthop 79:683–688
37. Lotke PA, Carolan gF, Puri n (2006) Impaction grafting for bone defects in revision total knee arthroplasty. Clin Orthop Relat Res 446:99–103
38. ghazavi MT, Stockley I, yee g, Davis A, gross Ae (1997) Reconstruction of massive bone defects with allograft in revision total knee arthroplasty. J Bone Joint Surg Am 79:17–25
39. Backstein D, Safir O, gross A (2006) Management of bone loss: structural grafts in revision total knee arthroplasty. Clin Orthop Relat Res 446:104–112
40. Clatworthy Mg, Ballance J, Brick gW, Chandler HP, gross Ae (2011) The use of structural allograft for uncontained defects in revision total knee arthroplasty: a minimum five-year review. J Bone Joint Surg Am 83:404–411
41. Bauman RD, Lewallen Dg, Hanssen AD (2009) Limitations of structural allograft in revision total knee arthroplasty. Clin Orthop Relat Res 467:818–824

Arch Orthop Trauma Surg
1 3
42. Brand Mg, Daley RJ, ewald FC, Scott RD (1989) Tibial tray augmentation with modular metal wedges for tibial bone stock deficiency. Clin Orthop Relat Res 248:71–79
43. Haas SB, Insall Jn, Montgomery W 3rd, Windsor Re (1995) Revision total knee arthroplasty with use of modular compo-nents with stems inserted without cement. J Bone Joint Surg Am 77:1700–1707
44. Werle JR, goodman SB, Imrie Sn (2002) Revision total knee arthroplasty using large distal femoral augments for severe metaphyseal bone deficiency: a preliminary study. Orthopedics 25:325–327
45. Patel Jv, Masonis JL, guerin J, Bourne RB, Rorabeck CH (2004) The fate of augments to treat type-2 bone defects in revision knee arthroplasty. J Bone Joint Surg 86:195–199
46. Wood gC, naudie DD, MacDonald SJ, McCalden RW, Bourne RB (2009) Results of press-fit stems in revision knee arthroplas-ties. Clin Orthop Relat Res 467:810–817
47. Meneghini RM, Lewallen Dg, Hansesen AD (2008) use of porous tantalum metaphyseal cones for severe tibial bone loss during revi-sion total knee replacement. J Bone Joint Surg Am 90:78–84
48. Malhotra R, garg B, Kumar v (2011) Dual massive skeletal allograft in revision total knee arthroplasty. Indian J Orthop 45:368–371
49. Qiu yy, yan CH, Chiu Ky, ng Fy (2012) Review article: treat-ments for bone loss in revision total knee arthroplasty. J Orthop Surg 20:78–86
50. Wang JW, Hsu CH, Huang CC, Lin PC, Chen WS (2013) Reconstruction using femoral head allograft in revision total knee replacement: an experience in Asian patients. Bone Joint J 95-B:643–648
51. Richards CJ, garbuz DS, Pugh L, Masri BA (2011) Revision total knee arthroplasty: clinical outcome comparison with and without the use of femoral head structural allograft. J Arthroplast 26:1299–1304