Embed Size (px)
Citation preview
Treatment of Glenoid and Humeral Head
Bone Defects in Shoulder Instability
Nikolaos TzanakakisOrthopedic Surgeon
2nd Orthopedic Dept.Center for Shoulder Arthroscopy
IASO General HospitalAthens, Greece
Background
There is a well-recognized association between osseous defects of the glenoid or humerus and shoulder dislocation, which often leads to recurrent instability.
Boileau P., J Bone Joint Surg Am. 2006 Aug;88(8):1755-63. Lynch JR., J Shoulder Elbow Surg. 2009 Mar-Apr;18(2):317-28.
Burkhart SS., Instr Course Lect. 2009;58:323-36.
www.shoulder.gr
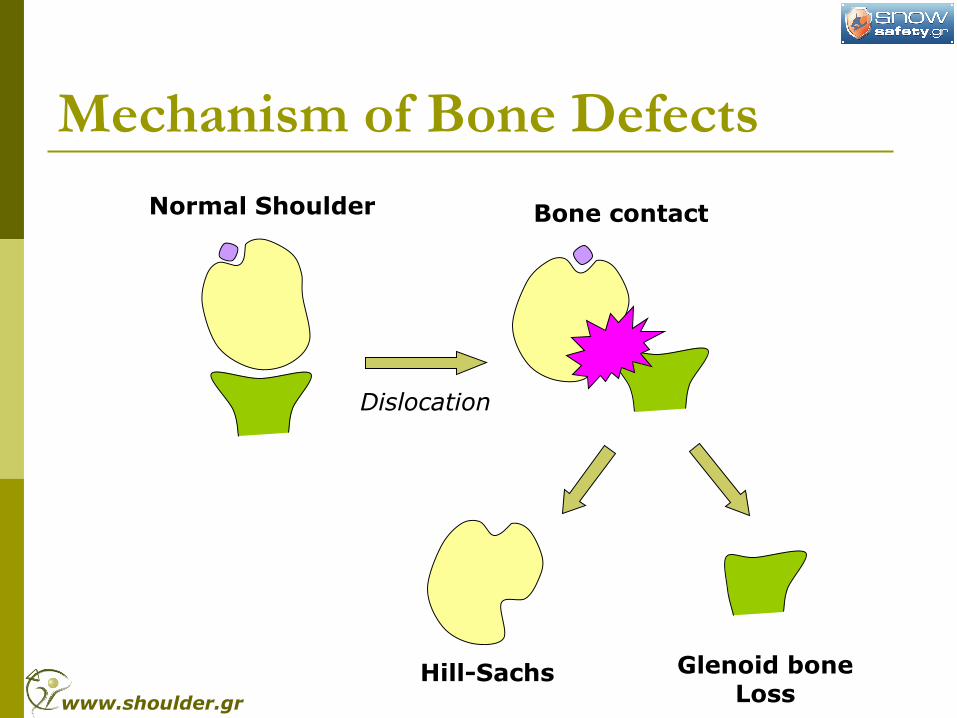
Mechanism of Bone Defects
Hill-Sachs Glenoid bone Loss
Normal Shoulder Bone contact
Dislocation
www.shoulder.gr
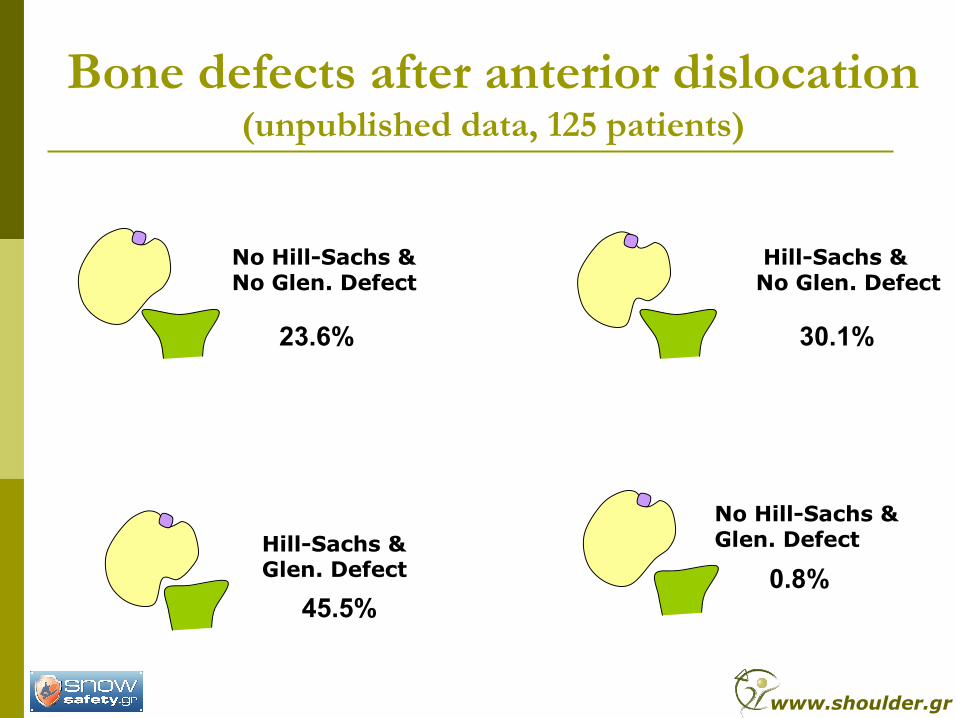
Bone defects after anterior dislocation (unpublished data, 125 patients)
Hill-Sachs & Glen. Defect
Hill-Sachs & No Glen. Defect
No Hill-Sachs & No Glen. Defect
No Hill-Sachs & Glen. Defect
23.6%
45.5%
30.1%
0.8%
www.shoulder.gr
Bone Defects Frequency Hill-Sachs: 65-71% first dislocation
Hill-Sachs: 93% recurrent dislocations
Glenoid bone loss: 5-56% traumatic instability
Possitive correlation between Number of dislocations and depth/extend of the lesions
Lynch JR, J Shoulder Elbow Surg (2009) 18, 317-328
www.shoulder.gr
Humeral Head Bone Defect
(Hill-Sachs Lesion)
www.shoulder.gr
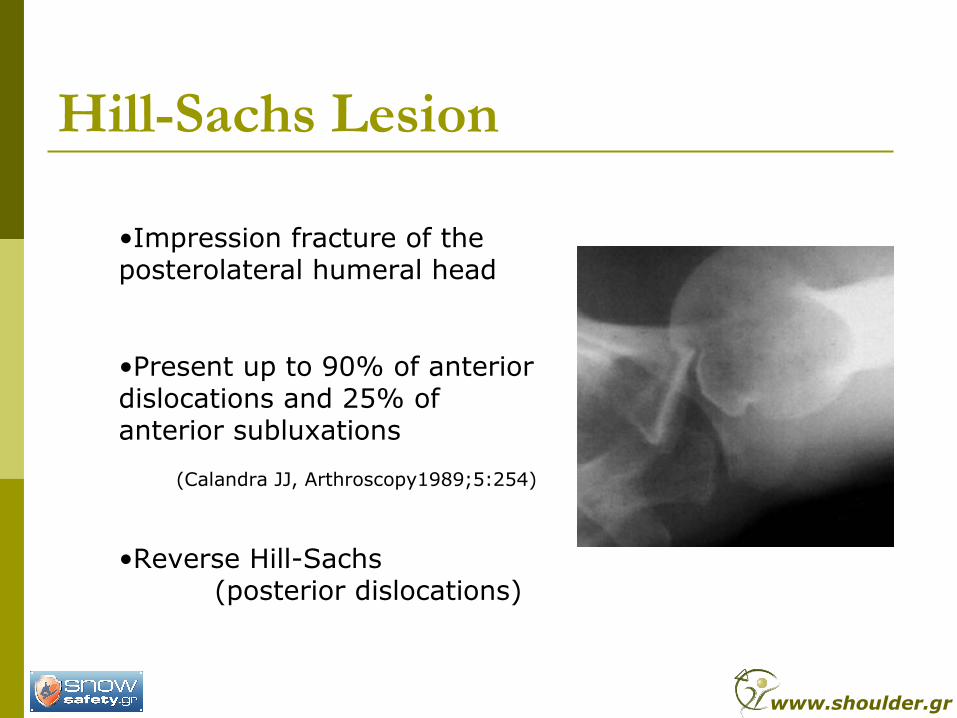
Hill-Sachs Lesion
•Impression fracture of the posterolateral humeral head
•Present up to 90% of anterior dislocations and 25% of anterior subluxations
(Calandra JJ, Arthroscopy1989;5:254)
•Reverse Hill-Sachs (posterior dislocations)
www.shoulder.gr
Hill-Sachs Arthroscopic Grading
Grade I: defect in the articular surface down to subchondral bone
Grade II: includes the subchondral bone
Grade III: large subchondral defect
Calandra et. Al, 1989
www.shoulder.gr
Hill-Sachs Grading MINOR: Less than 20% of head
MODERATE: 20-40% of head
SEVERE: Greater than 40% of head
www.shoulder.gr
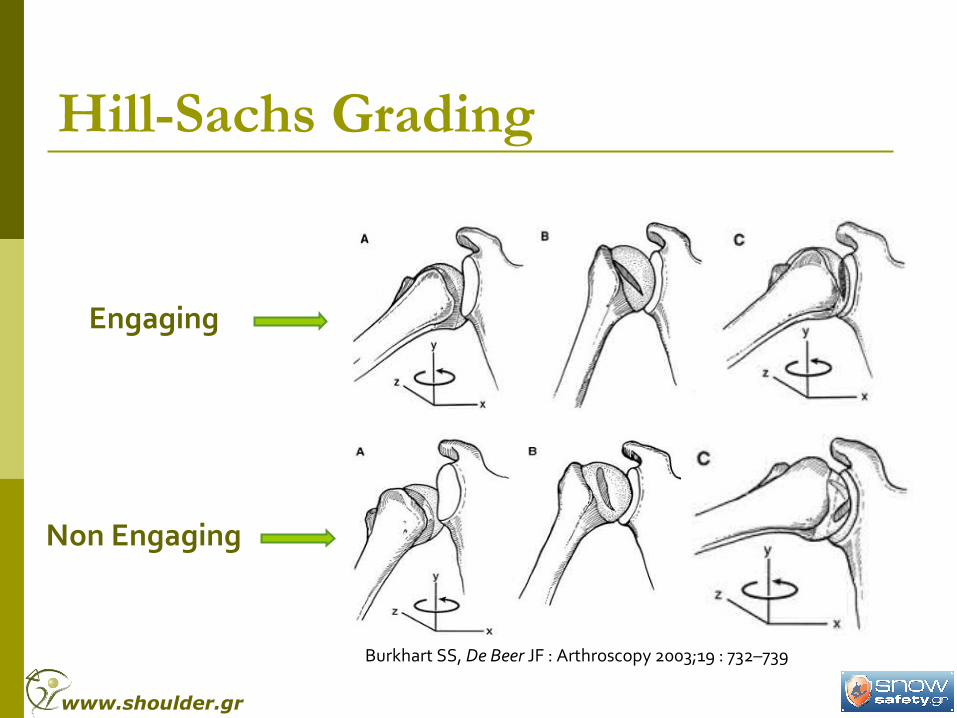
Hill-Sachs Grading
Engaging
Non Engaging
Burkhart SS, De Beer JF : Arthroscopy 2003;19 : 732–739
www.shoulder.gr
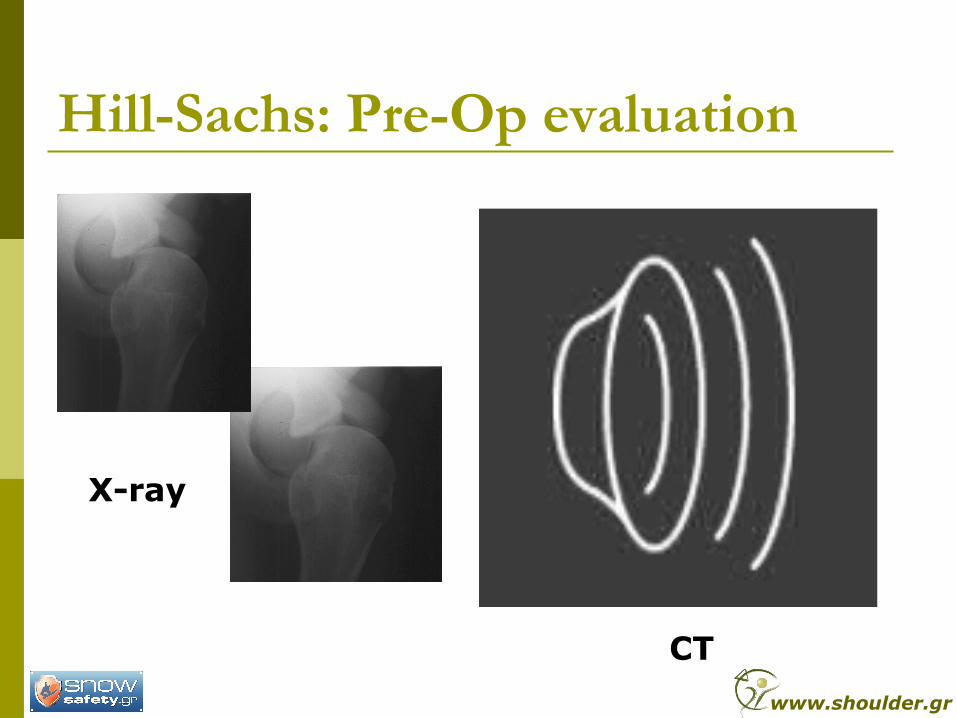
Hill-Sachs: Pre-Op evaluation
X-ray
CT
www.shoulder.gr
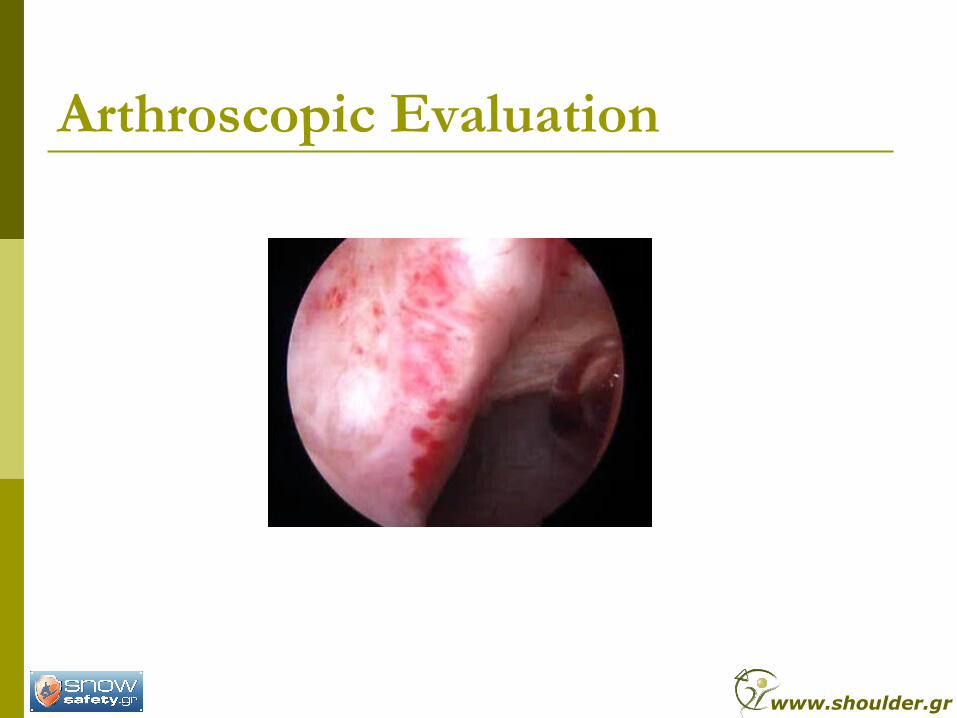
Arthroscopic Evaluation
www.shoulder.gr
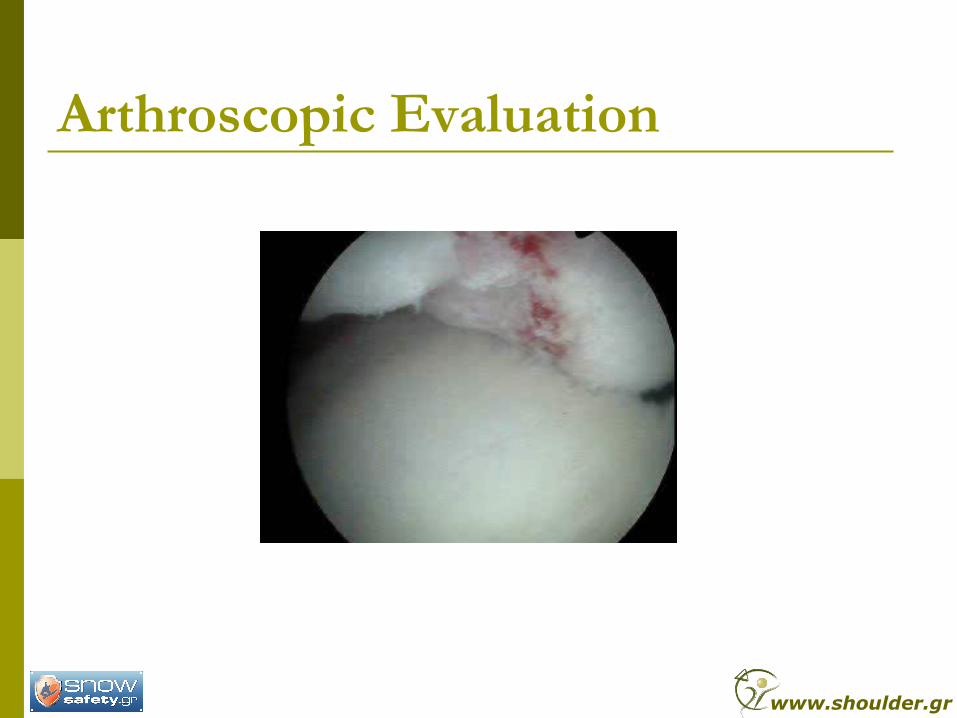
Arthroscopic Evaluation
www.shoulder.gr
Guidelines for Hill-Sachs Treatment Most Hill-Sachs lesions are small and don’t
require treatment
Each lesion should be evaluated during surgery
Treatment Required for:
- Lesions found to be engaging in a normal ROM
- Lesions representing >30%-40% of the articular surface
Center for Shoulder Arthroscopy
IASO GENERAL Hospital
Treatment Options for Hill-Sachs
Humeral rotation osteotomy (Weber BG, JBJS 1984;66A:1443)
Hemiarthroplasty / TSA for patients >50y/o (Flatow E, JSES 1993;12:1, 29)
Humeral head grafting(Gerber C, JBJS 1996;78A:376)
Remplissage (Wolf EM, Arthroscopy 2004;20(suppl1) :e14)
www.shoulder.gr
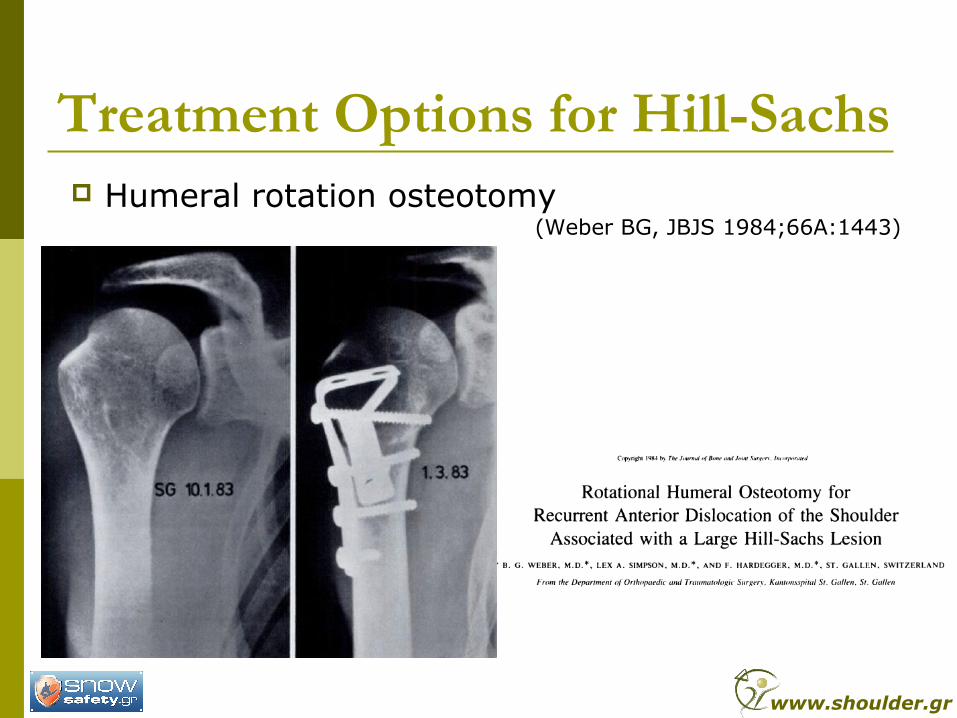
Treatment Options for Hill-Sachs Humeral rotation osteotomy
(Weber BG, JBJS 1984;66A:1443)
www.shoulder.gr
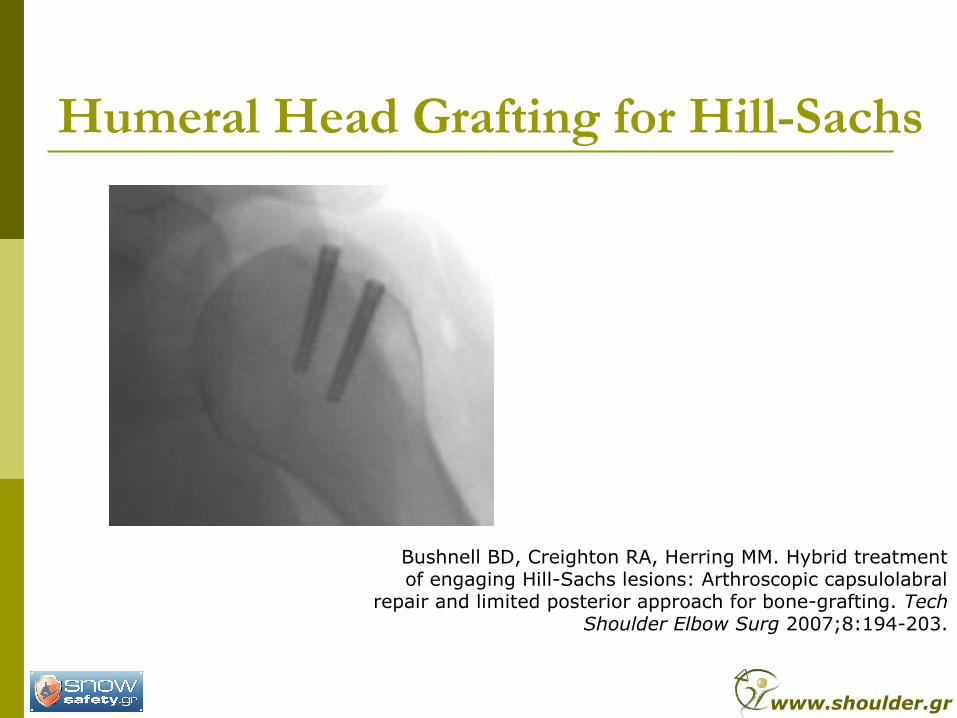
Humeral Head Grafting for Hill-Sachs
Bushnell BD, Creighton RA, Herring MM. Hybrid treatmentof engaging Hill-Sachs lesions: Arthroscopic capsulolabral
repair and limited posterior approach for bone-grafting. TechShoulder Elbow Surg 2007;8:194-203.
www.shoulder.gr
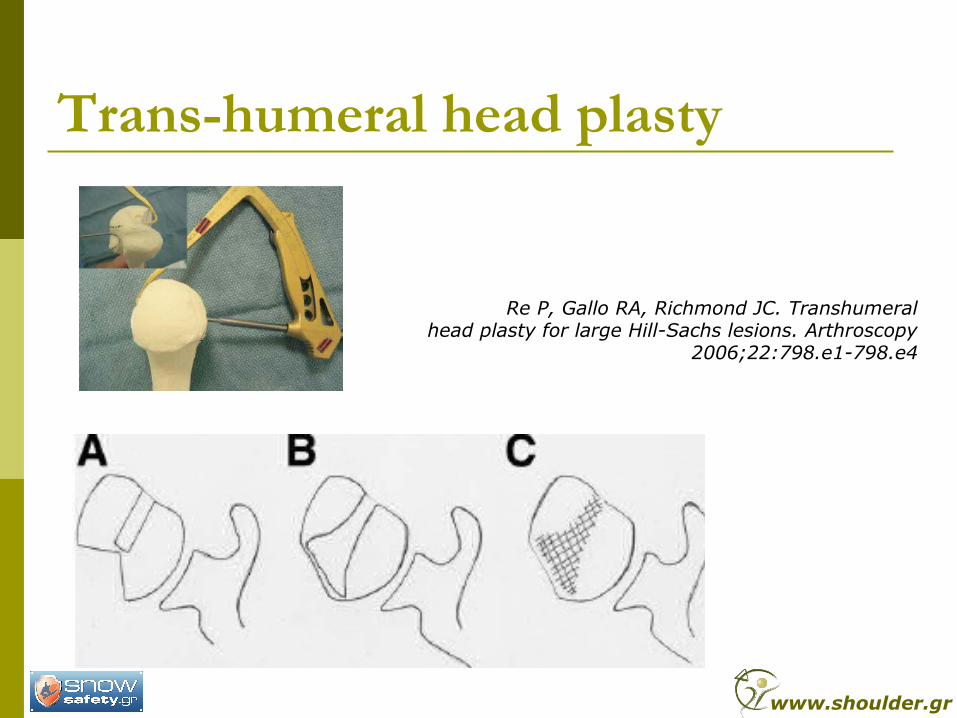
Trans-humeral head plasty
Re P, Gallo RA, Richmond JC. Transhumeralhead plasty for large Hill-Sachs lesions. Arthroscopy
2006;22:798.e1-798.e4
www.shoulder.gr
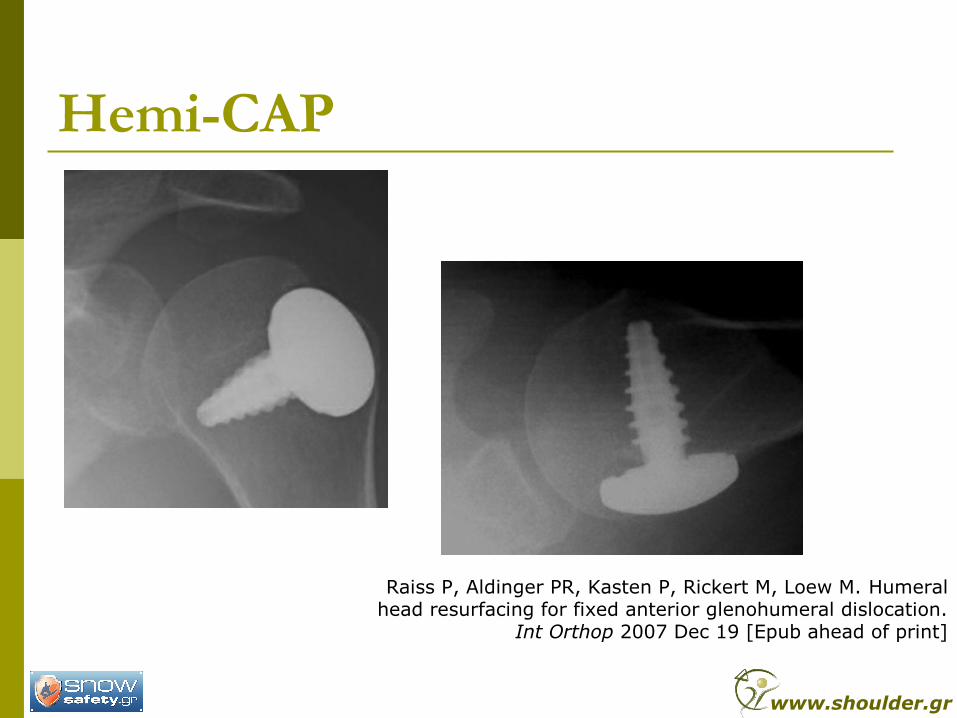
Hemi-CAP
Raiss P, Aldinger PR, Kasten P, Rickert M, Loew M. Humeralhead resurfacing for fixed anterior glenohumeral dislocation.
Int Orthop 2007 Dec 19 [Epub ahead of print]
www.shoulder.gr
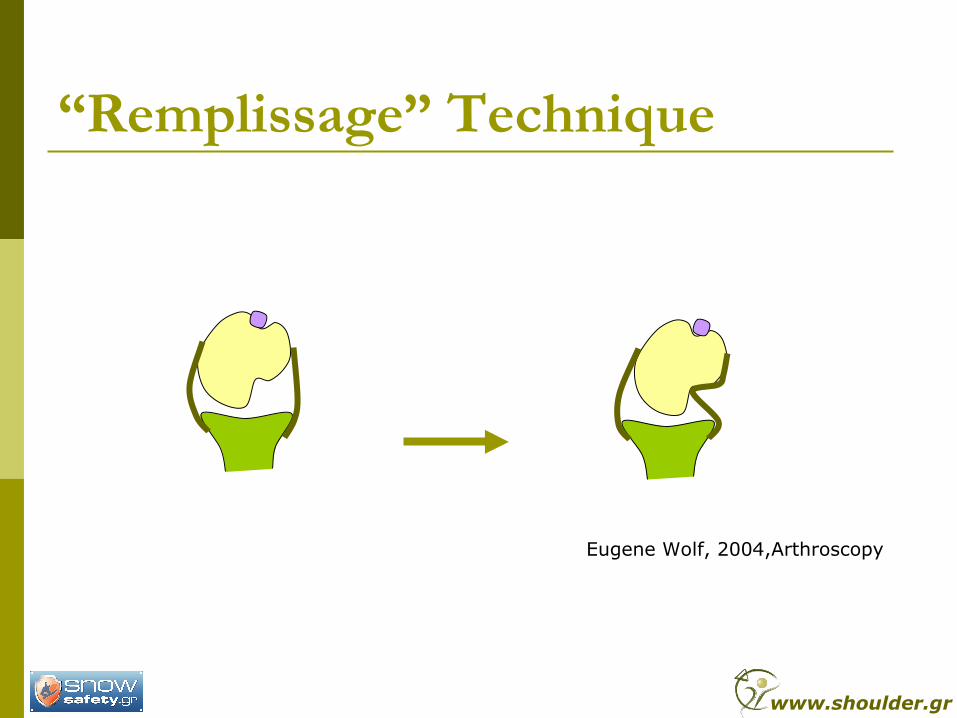
“Remplissage” Technique
Eugene Wolf, 2004,Arthroscopy
www.shoulder.gr
Arthroscopic Remplissage
www.shoulder.gr
Glenoid Bone Defects
www.shoulder.gr
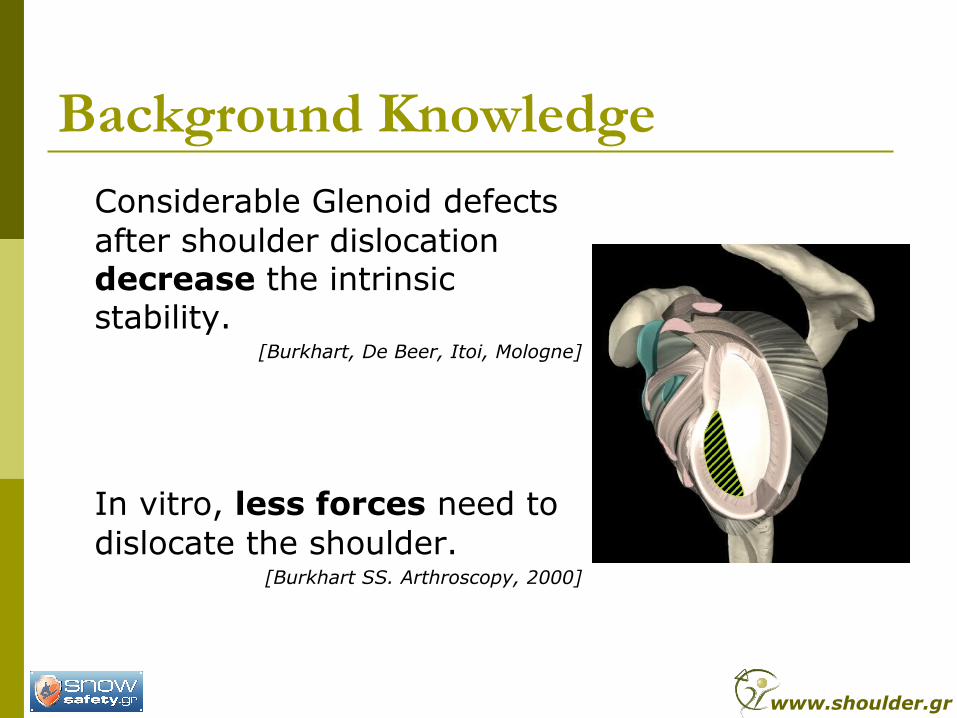
Background KnowledgeConsiderable Glenoid defects after shoulder dislocation decrease the intrinsic stability.
[Burkhart, De Beer, Itoi, Mologne]
In vitro, less forces need to dislocate the shoulder.
[Burkhart SS. Arthroscopy, 2000]
www.shoulder.gr
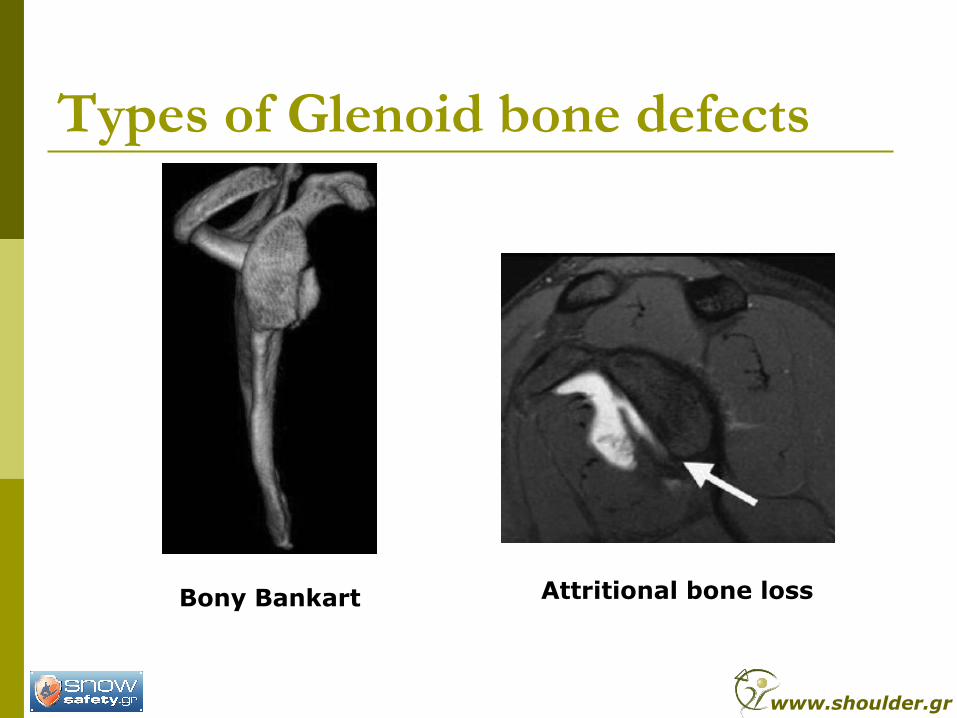
Types of Glenoid bone defects
Bony Bankart Attritional bone loss
www.shoulder.gr
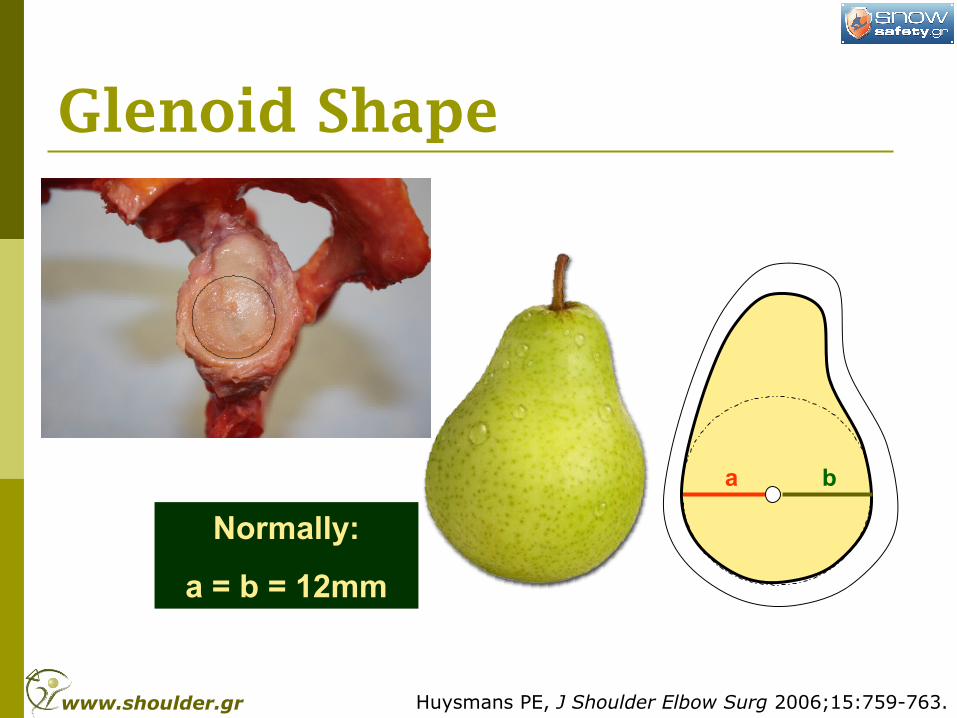
Glenoid Shape
a b
Normally:
a = b = 12mm
Huysmans PE, J Shoulder Elbow Surg 2006;15:759-763.www.shoulder.gr
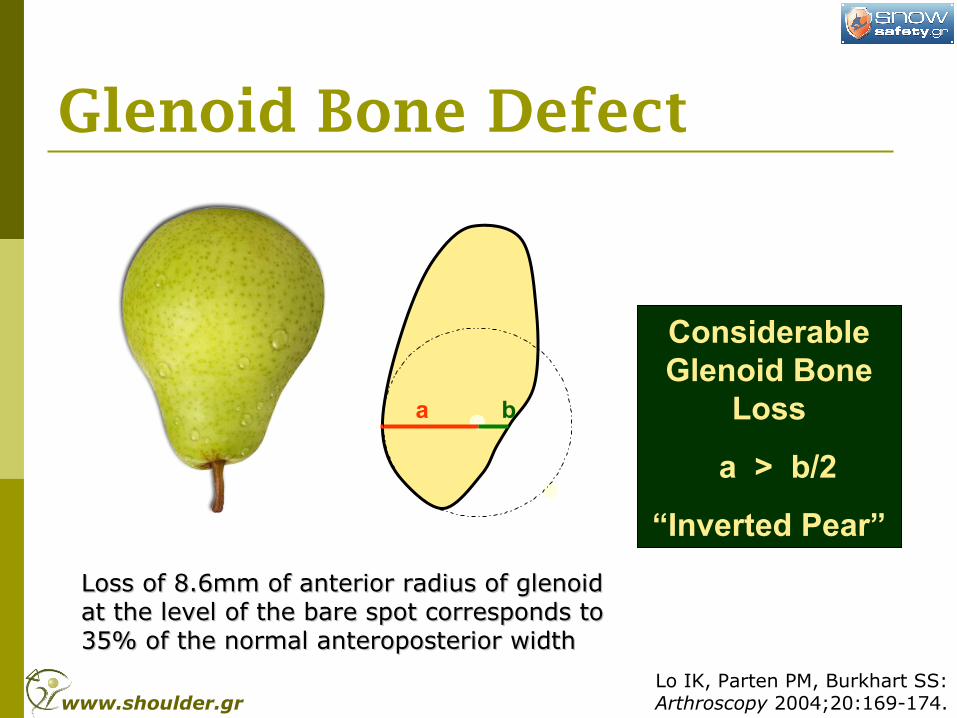
Glenoid Bone Defect
Considerable Glenoid Bone
Loss
a > b/2
“Inverted Pear”
a b
Loss of 8.6mm of anterior radius of glenoid Loss of 8.6mm of anterior radius of glenoid at the level of the bare spot corresponds to at the level of the bare spot corresponds to 35% of the normal anteroposterior width35% of the normal anteroposterior width
Lo IK, Parten PM, Burkhart SS:Arthroscopy 2004;20:169-174.www.shoulder.gr
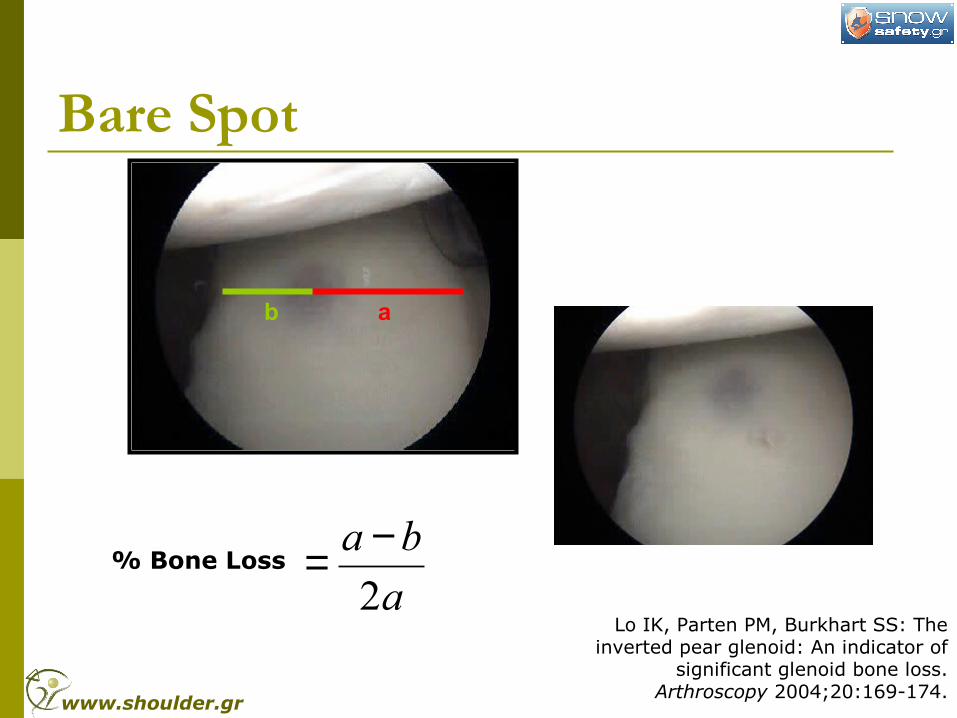
Bare Spot
b a
% Bone Loss
Lo IK, Parten PM, Burkhart SS: Theinverted pear glenoid: An indicator of
significant glenoid bone loss.Arthroscopy 2004;20:169-174.
a
ba
2
−=
www.shoulder.gr
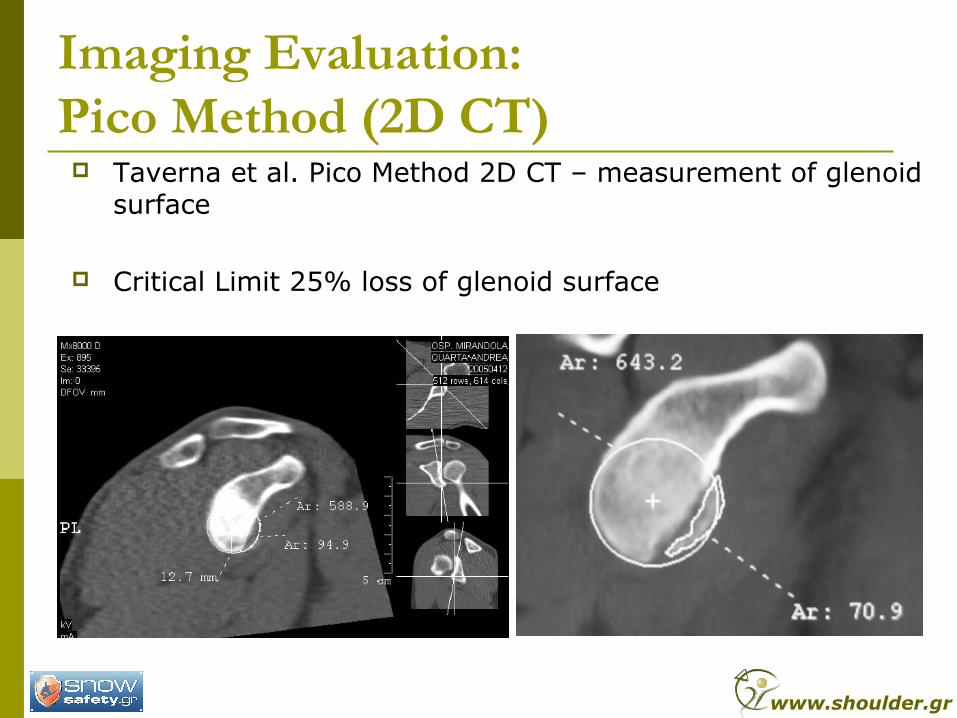
Imaging Evaluation:Pico Method (2D CT) Taverna et al. Pico Method 2D CT – measurement of glenoid
surface
Critical Limit 25% loss of glenoid surface
www.shoulder.gr
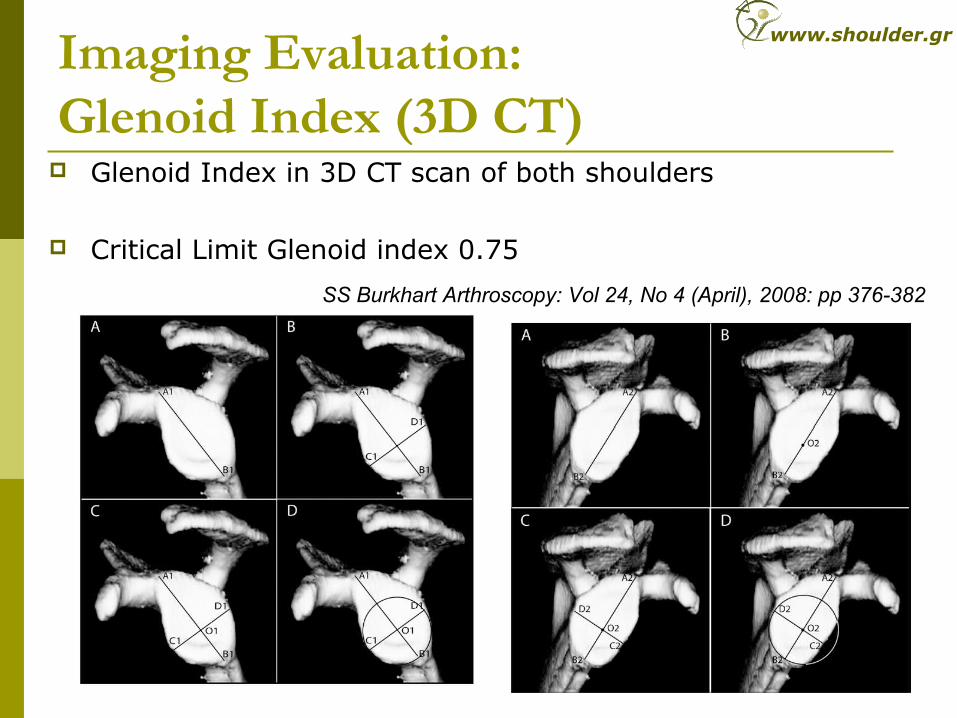
Imaging Evaluation:Glenoid Index (3D CT)
Glenoid Index in 3D CT scan of both shoulders
Critical Limit Glenoid index 0.75
SS Burkhart Arthroscopy: Vol 24, No 4 (April), 2008: pp 376-382
www.shoulder.gr
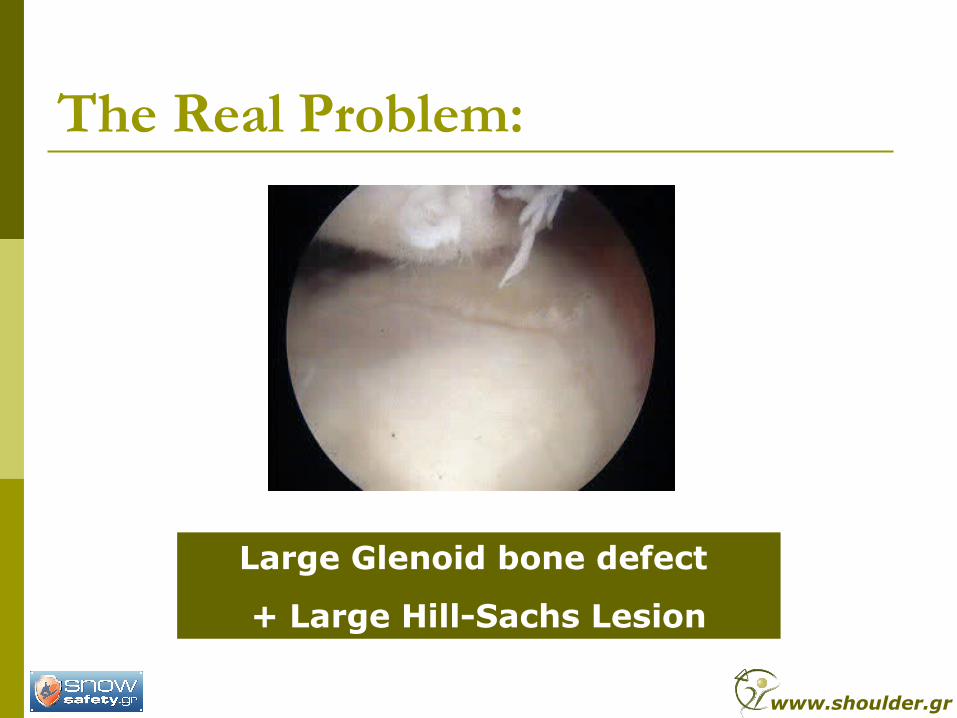
The Real Problem:
Large Glenoid bone defect
+ Large Hill-Sachs Lesion
www.shoulder.gr
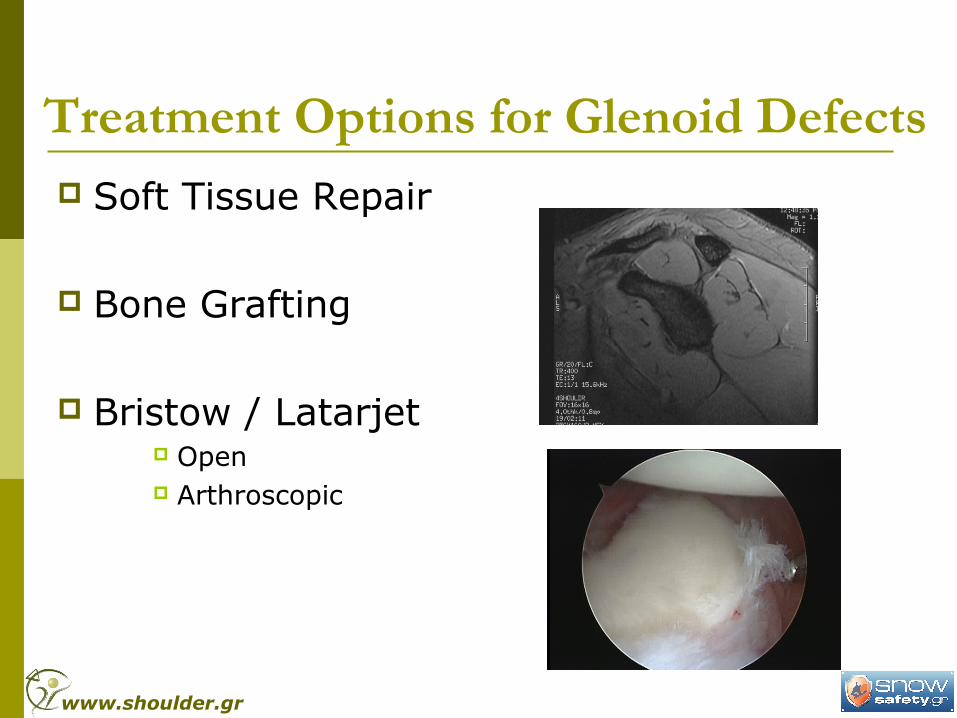
Treatment Options for Glenoid Defects Soft Tissue Repair
Bone Grafting
Bristow / Latarjet Open Arthroscopic
www.shoulder.gr
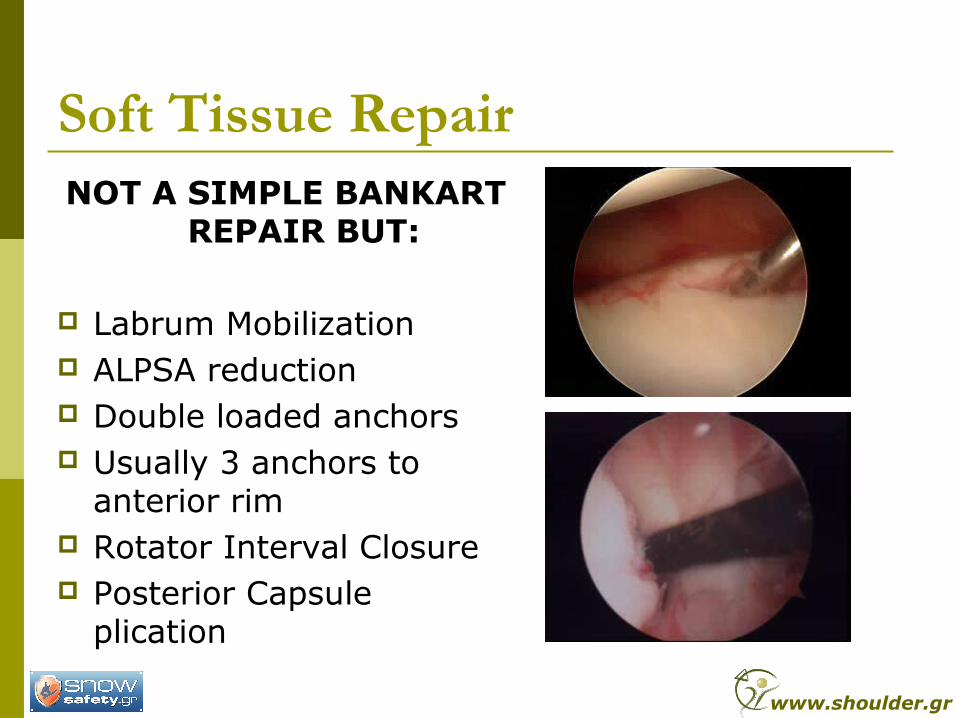
Soft Tissue Repair NOT A SIMPLE BANKART
REPAIR BUT:
Labrum Mobilization ALPSA reduction Double loaded anchors Usually 3 anchors to
anterior rim Rotator Interval Closure Posterior Capsule
plication
www.shoulder.gr
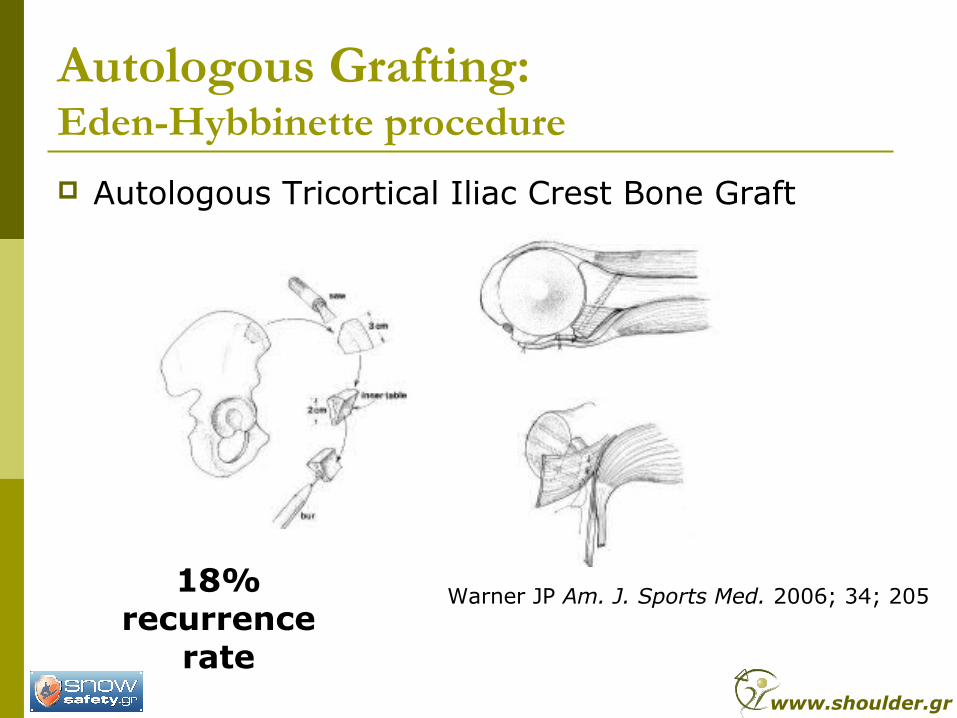
Autologous Grafting:Eden-Hybbinette procedure
Autologous Tricortical Iliac Crest Bone Graft
Warner JP Am. J. Sports Med. 2006; 34; 20518% recurrence
ratewww.shoulder.gr
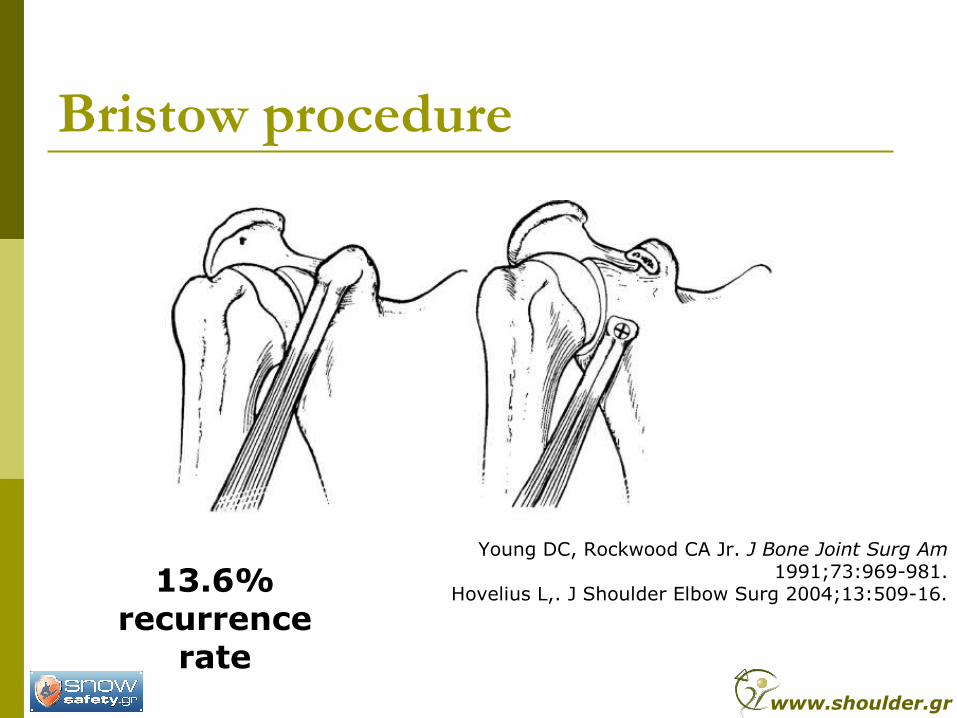
Bristow procedure
Young DC, Rockwood CA Jr. J Bone Joint Surg Am1991;73:969-981.
Hovelius L,. J Shoulder Elbow Surg 2004;13:509-16.13.6% recurrence
ratewww.shoulder.gr
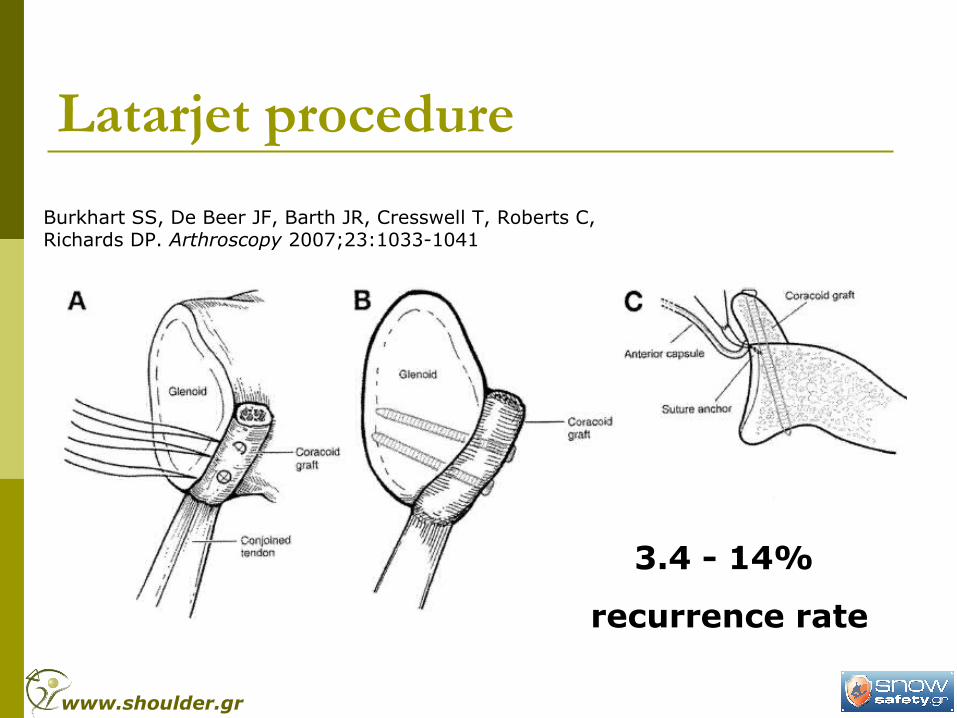
Latarjet procedure
Burkhart SS, De Beer JF, Barth JR, Cresswell T, Roberts C,Richards DP. Arthroscopy 2007;23:1033-1041
3.4 - 14%
recurrence rate
www.shoulder.gr
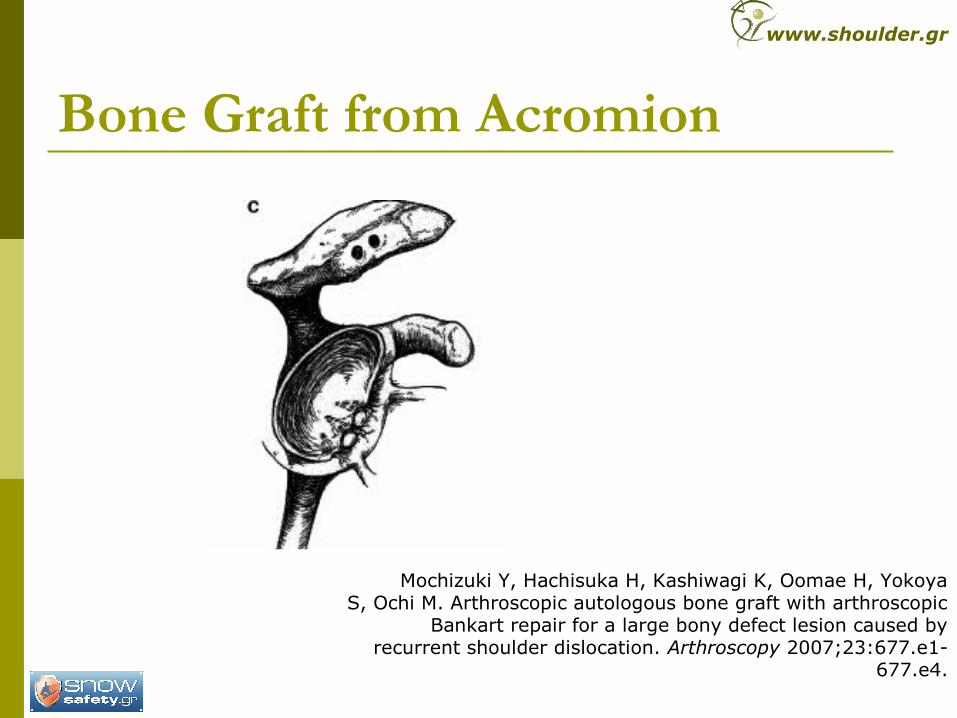
Bone Graft from Acromion
Mochizuki Y, Hachisuka H, Kashiwagi K, Oomae H, YokoyaS, Ochi M. Arthroscopic autologous bone graft with arthroscopic
Bankart repair for a large bony defect lesion caused byrecurrent shoulder dislocation. Arthroscopy 2007;23:677.e1-
677.e4.
www.shoulder.gr
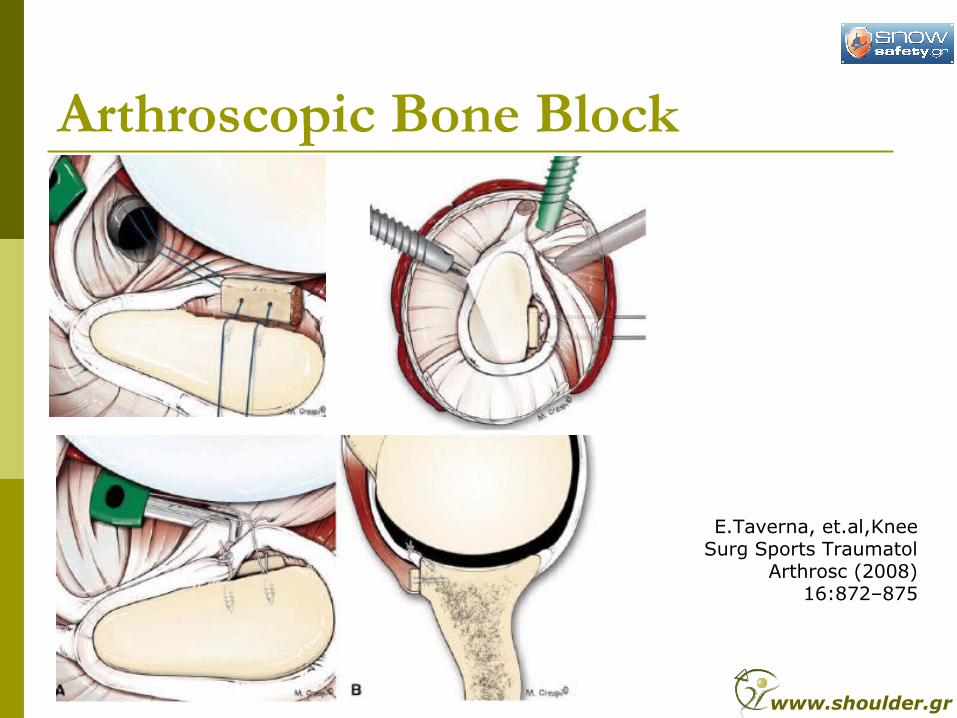
Arthroscopic Bone Block
E.Taverna, et.al,Knee Surg Sports Traumatol
Arthrosc (2008) 16:872–875
www.shoulder.gr
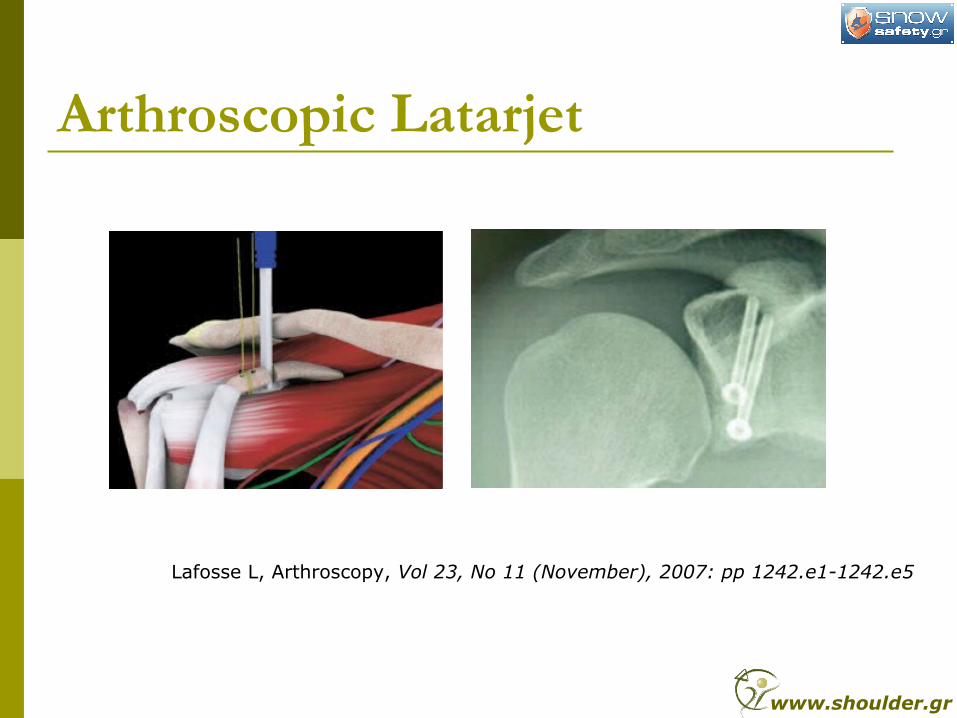
Arthroscopic Latarjet
Lafosse L, Arthroscopy, Vol 23, No 11 (November), 2007: pp 1242.e1-1242.e5
www.shoulder.gr
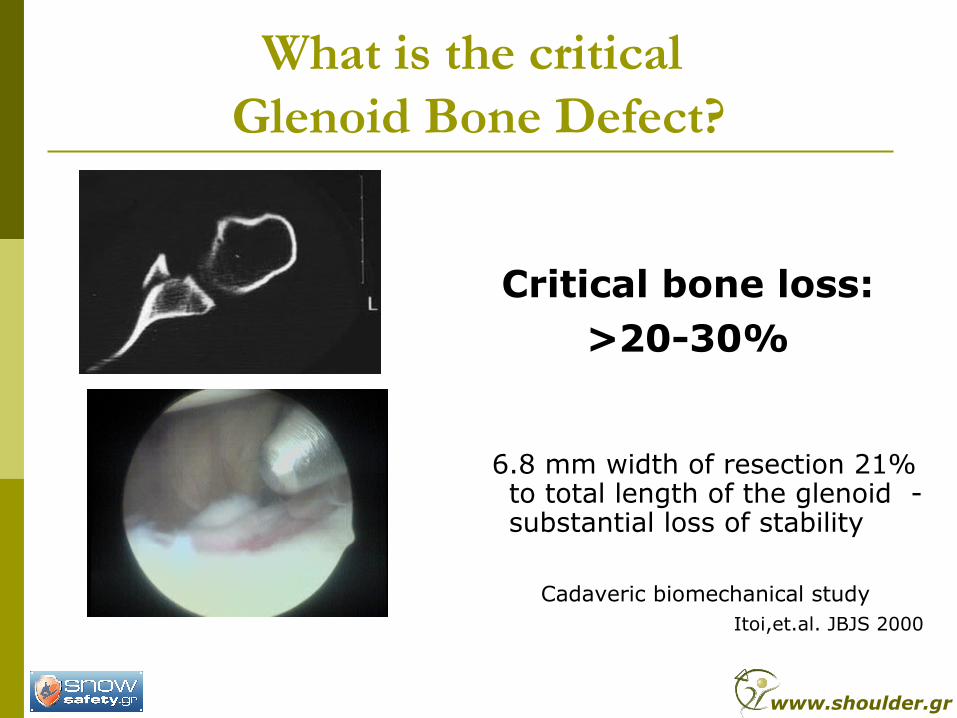
What is the critical Glenoid Bone Defect?
Critical bone loss:>20-30%
6.8 mm width of resection 21% to total length of the glenoid - substantial loss of stability
Cadaveric biomechanical study
Itoi,et.al. JBJS 2000
www.shoulder.gr
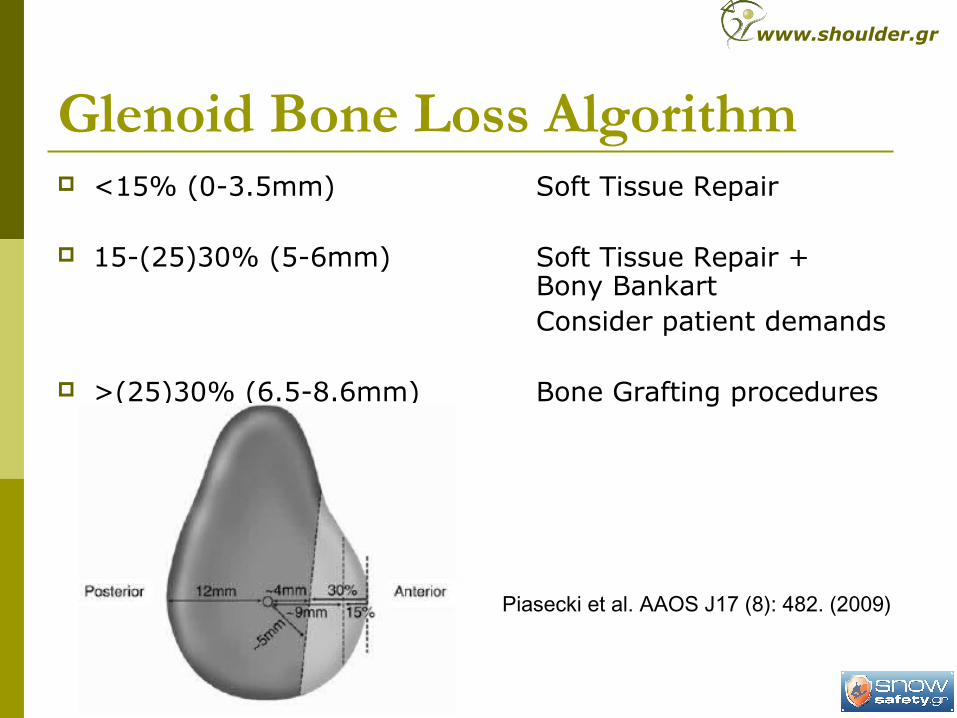
Glenoid Bone Loss Algorithm <15% (0-3.5mm) Soft Tissue Repair
15-(25)30% (5-6mm) Soft Tissue Repair + Bony BankartConsider patient demands
>(25)30% (6.5-8.6mm) Bone Grafting procedures
Piasecki et al. AAOS J17 (8): 482. (2009)
www.shoulder.gr
Our Technique
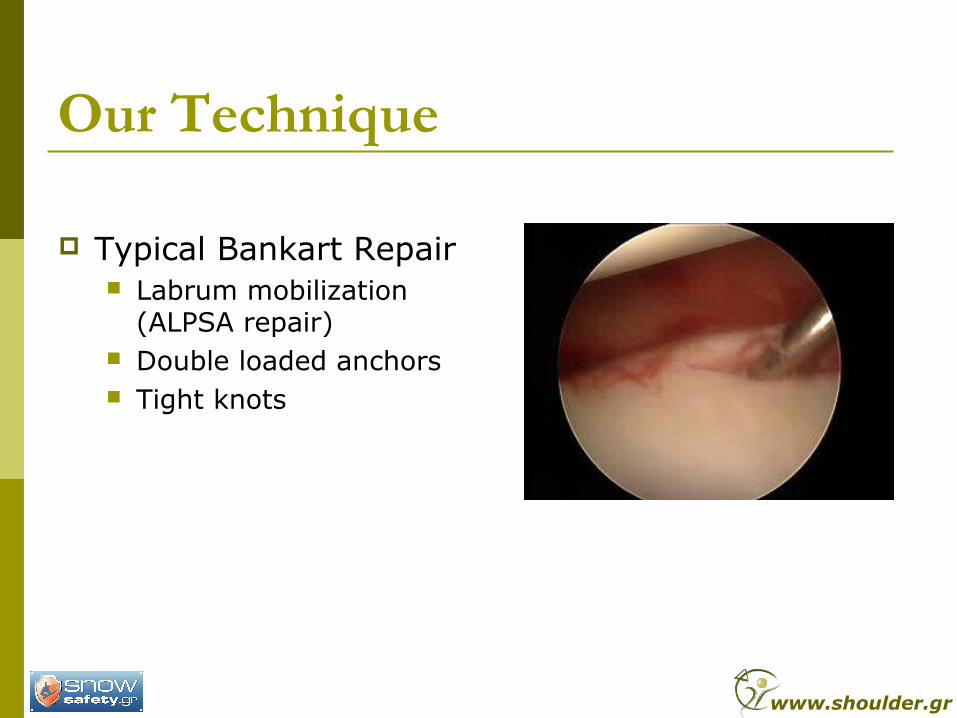
Typical Bankart Repair Labrum mobilization
(ALPSA repair) Double loaded anchors Tight knots
www.shoulder.gr
Our Technique
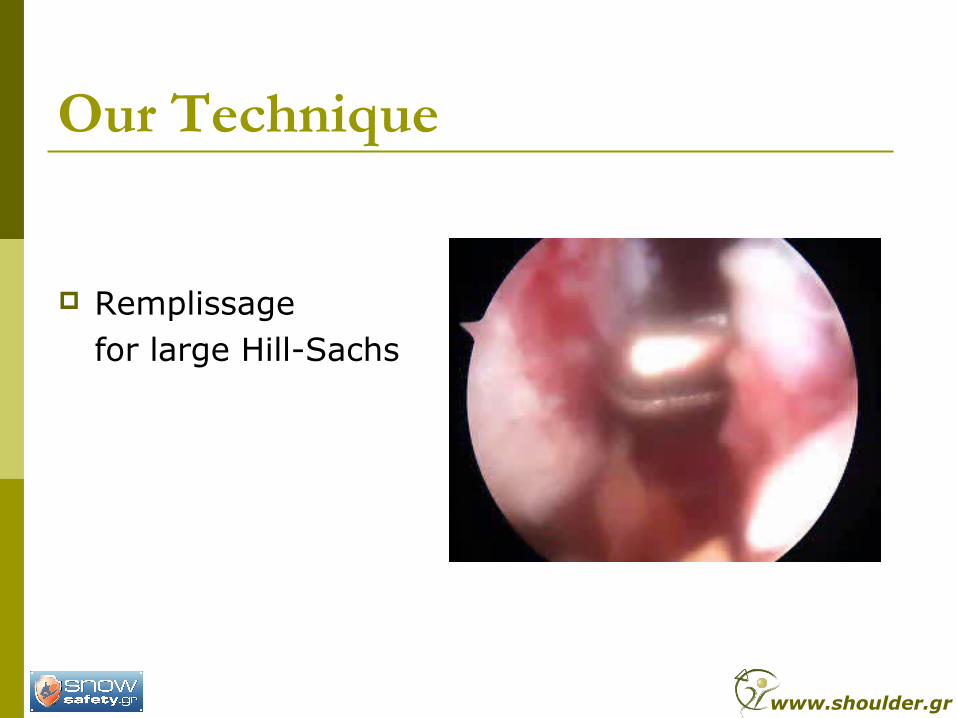
Remplissage for large Hill-Sachs
www.shoulder.gr
Our Technique
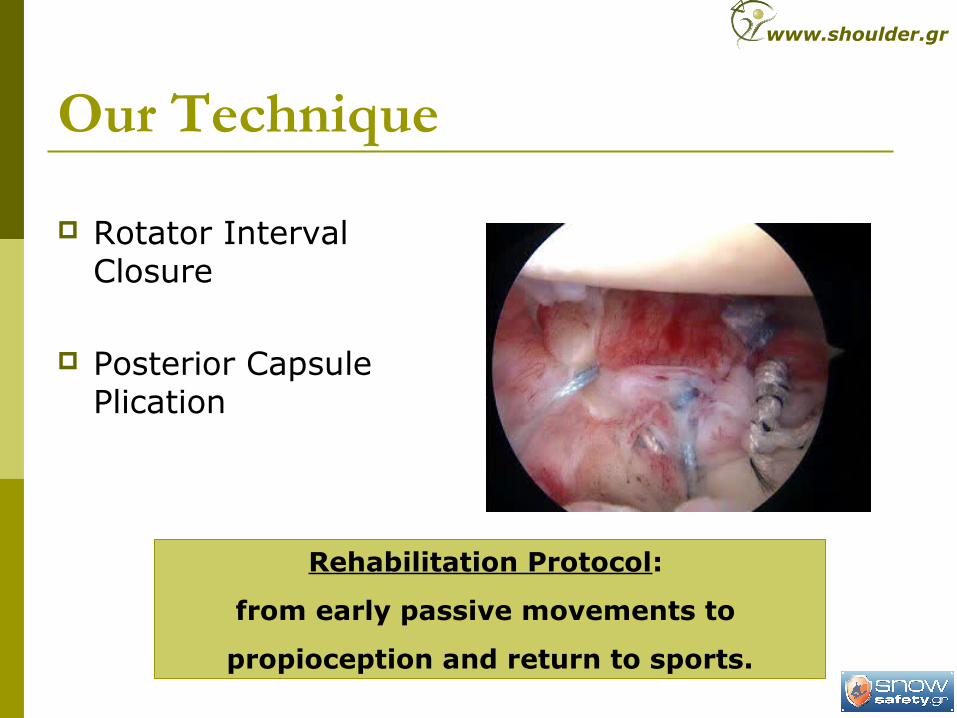
Rotator Interval Closure
Posterior Capsule Plication
Rehabilitation Protocol:
from early passive movements to
propioception and return to sports.
www.shoulder.gr
Our Results Period: 1999-2004
116 patients with anterior shoulder instability
Arthroscopic Treatment
At least 5 years follow-up (range 5-9.75 years)
Hill-Sachs 78/116 67.2% Glenoid defect 36/116 31.0% Invetred pear 8/116 6.8%
www.shoulder.gr
Our Results Recurrence rate: 7/116 6.03%
(2 MVA, 2 Sports, 1 Fall, 1 No Comply, 1 Minor Trauma)6/7 re-operated arthroscopicaly – No recurrence yet
Rowe-Zarins: Pre-Op 33 (15-80),Post-Op:95 (80-100)
Satisfaction 109/116 Very Satisfied 93.9% 6/116 Satisfied 5.2% 1/116 Did not answer 0.9%
Return to work: 116/116 100% Return to sports: 45/116 38.8%
www.shoulder.gr
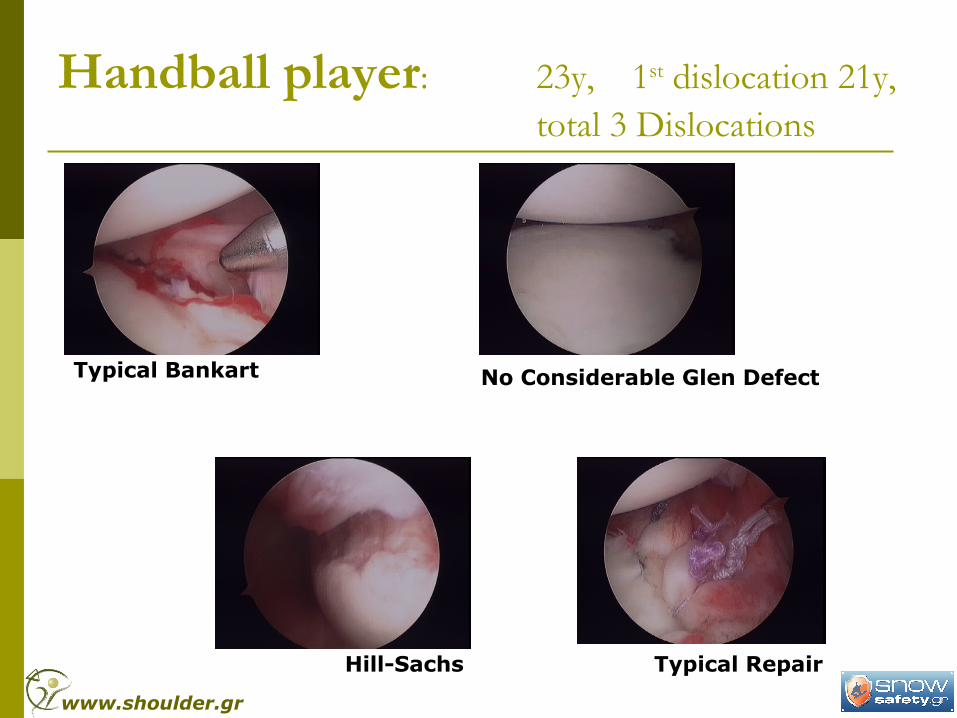
Handball player: 23y, 1st dislocation 21y, total 3 Dislocations
Typical Bankart No Considerable Glen Defect
Hill-Sachs Typical Repair
www.shoulder.gr
Typical Rehabilitation Program
…full return to sports 9 months later
…but 15 months after the operation….
Handball player: 23y, 1st dislocation 21y, Left shoulder, Total 3 Dislocations
www.shoulder.gr
Handball player: 23y, 1st dislocation 21y, Left shoulder, Total 3 Dislocations
www.shoulder.gr

Handball player: 25y, 15 months after first Bankart Repair
www.shoulder.gr
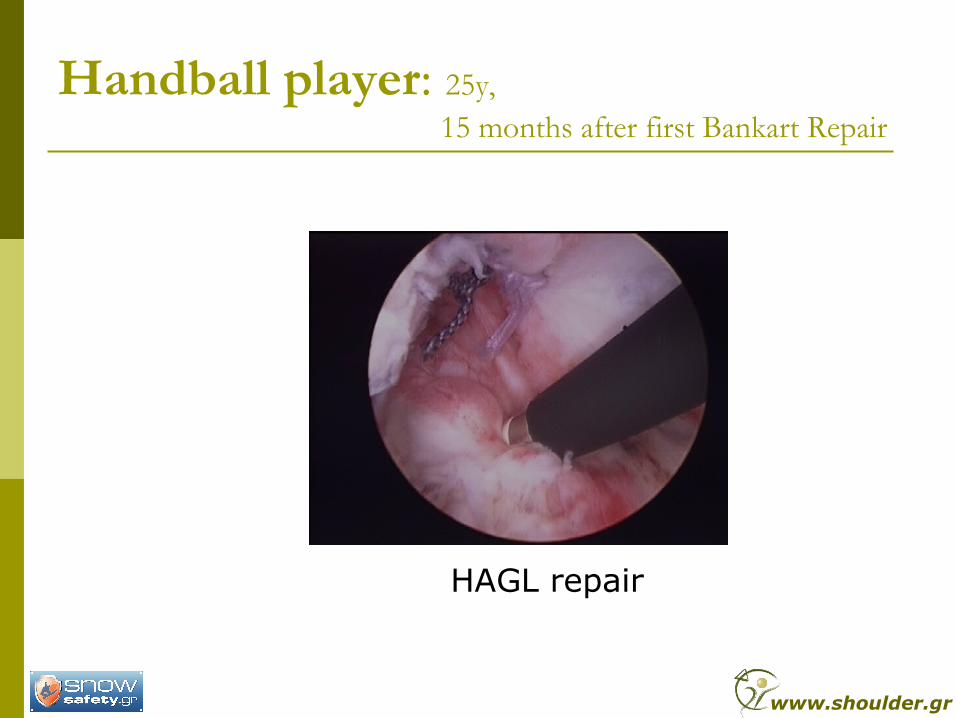
HAGL repair
Handball player: 25y, 15 months after first Bankart Repair
www.shoulder.gr
Conclusions Humeral Head bone loss (Hill-Sachs)
Graft reconstruction Prosthetic replacement Remplissage
Glenoid bone loss Soft Tissue Repair (more than a simple Bankart
repair) Bone Grafting (many methods) Bristow or Laterjet
Open Arthroscopic
www.shoulder.gr

Thank you for your attention
www.shoulder.gr