Embed Size (px)
Citation preview

BRIEF REVIEW
BODY COMPOSITION AND MILITARY
PERFORMANCEdMANY THINGS TO MANY PEOPLE
KARL E. FRIEDL
Telemedicine and Advanced Technology Research Center, U.S. Army Medical Research and Materiel Command, Fort Detrick,Maryland
ABSTRACT
Friedl, KE. Body composition and military performancedMany
things to many people. J Strength Cond Res 26(7): S87–
S100, 2012dSoldiers are expected to maintain the highest
possible level of physical readiness because they must be
ready to mobilize and perform their duties anywhere in the
world at any time. The objective of Army body composition
standards is to motivate physical training and good nutrition
habits to ensure a high state of readiness. Establishment of
enforceable and rational standards to support this objective
has been challenging even at extremes of body size. Morbidly
obese individuals are clearly not suited to military service, but
very large muscular individuals may be superbly qualified for
soldier performance demands. For this reason, large individuals
are measured for body fat using a waist circumference-based
equation (female soldiers are also measured for hip circumfer-
ence). The main challenge comes in setting appropriate fat
standards to support the full range of Army requirements. Mil-
itary appearance ideals dictate the most stringent body fat
standards, whereas health risk thresholds anchor the most lib-
eral standards, and physical performance associations fall on
a spectrum between these 2 poles. Standards should not ex-
clude or penalize specialized performance capabilities such as
endurance running or power lifting across a spectrum of body
sizes and fat. The full integration of women into the military
further complicates the issue because of sexually dimorphic
characteristics that make gender-appropriate standards essen-
tial and where inappropriately stringent standards can compro-
mise both health and performance of this segment of the force.
Other associations with body composition such as stress
effects on intraabdominal fat distribution patterns and meta-
bolic implications of a fat reserve for survival in extreme environ-
ments are also relevant considerations. This is a review of
the science that underpins the U.S. Army body composition
standards.
KEY WORDS body fat, physical activity, metabolism, chronic
health, appearance
INTRODUCTION
Military and physical fitness trainers are keenlyaware that specific types of physical perfor-mance are associated with specific body sizeand composition characteristics (24). An
obvious example is the contrast between the massive mus-cularity of a power lifter and the extreme thinness andleanness of a marathon runner. Body size, body composi-tion, and military bearing (appearance) have always beenimportant to the military because of real and perceivedassociations with physical performance capabilities (28).Despite associations, there is low specific predictive valueof body size or composition to soldier performance withinthe wide range of healthy weights and adiposity (51). Nev-ertheless, it is reasonable to select against extremes of un-derweight and overweight where health and performancehas a high probability of compromise, but this still boundsa large range of body size and composition, comprisinga full spectrum of individuals that look like Vogue models,the fictional mesomorphic cartoon character “SergeantRock,” and fatter but extremely strong men. It is also rea-sonable to enforce body composition standards that drivefitness and nutrition habits, but these must be achievable byany motivated healthy soldier. These reasonably achievablestandards of size and body composition must take intoaccount factors such as genetics, developmental influences,selection, and the plasticity of the body to recent and ha-bitual physical demands and other environmental factors(e.g., nutrition, health, neurobiology, and personal habits).The more recent inclusion of women in military servicesfurther complicates the issue because of sexually dimorphiccharacteristics that make “gender-appropriate” (rather than“gender-neutral”) standards essential to optimal health andperformance of the force (29,120). This is a review of thebasis for the U.S. Army body composition standards. Thecurrent U.S. Army screening weights and body fat stand-ards are shown in Table 1.
The opinions and assertions in this article are those of the author and donot necessarily represent the official position or views of theDepartment of the Army or the Department of Defense.
Address correspondence to Karl E. Friedl, [email protected].
26(7)/S87–S100
Journal of Strength and Conditioning Research� 2012 National Strength and Conditioning Association
VOLUME 26 | SUPPLEMENT 7 | JULY 2012 | S87
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.

PURPOSE OF U.S. MILITARY OCCUPATIONAL WEIGHT
AND BODY COMPOSITION STANDARDS
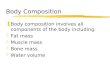
The purpose of military entry standards is to select recruitswho will be able to meet soldier standards. In turn, soldierbody composition standards are set according to therequirements of the Army, with general standards relevantto every individual regardless of their job assignment. Theserequirements include physical performance and militaryappearance and chronic health risk outcomes. Morbidobesity is negatively associated with each of these 3 broadcategories (health, performance, military appearance), butmore precise thresholds of risk at lower levels of obesity(overweight and overfat) require careful analysis and con-sideration of competing requirements (Figure 1). For exam-ple, the strongest Army women tend to carry more weightand fat and have a larger average waist circumference (WC)than do weaker women, increasing their risk for male-typehealth consequences such as cardiovascular disease (27,104).Thus, some superior performers may not have the lowesthealth risks. Imposing very strict body fat standards for anemphasis on military appearance is likely to compromisehealth and performance readiness by increasing disorderedeating habits (80,81,96) and may eliminate individuals withother critical capabilities (e.g., some of the strongest sol-diers). These are choices that have to be made, and it isimportant to clearly acknowledge the intent of the regulationthat drives the standards. For the US military, the overallobjective of enforced body composition standards is to
promote regular fitness and nutrition habits that ensurea physically capable military force that is ready to deployat any time.
ORIGIN OF THE DEPARTMENT OF DEFENSE BODY
COMPOSITION STANDARDS
Height and weight and the combination, usually in theform of the Quetelet Index, or body mass index (BMI,kilograms per meter squared), has long been used in soldierselection criteria (26). Height-weight tables were already inuse by the U.S. Army in the late 1800s, but the emphasiswas on eliminating inadequately muscled sickly or chroni-cally malnourished individuals. This focus on underweightshifted with improvements in nutrition and health overmore than a century, as reflected in an average 30-lb leanmass increase in young soldiers compared between 1864and 2000 (28). In the post-Vietnam era, overweight andobesity in career soldiers became the concern but height-weight table standards penalized large muscular individu-als. As early as 1942, the military had recognized that mus-cular football players tested by underwater weighing wouldhave failed to meet upper limits of Army height-weighttables that were in use at the time (123). Thus, weighttables were reduced to a screening tool and body compo-sition assessment was adopted as the Army Weight ControlProgram standard for the US Army. This began in the1980s, following a Department of Defense (DoD) Directivethat all military services would set body fat-based weightcontrol programs to promote fitness and prevent obesity inthe military. The recommendations came from a sympo-sium convened on June 17–19, 1980, by direction of thePresident because of a perception that the post-Vietnamera military was not maintaining adequate levels of physicalfitness (114). Body composition standards became part ofthe discussion and recommendations for improving mili-tary physical readiness. To set rational standards, therewas careful consideration of each of several outcomes re-lated to body fatdphysical strength, aerobic performance,military appearance, and chronic health. Several differenttypes of data were used in the deliberations, with the ulti-mate conclusion in the supporting research article that av-erage body fat of fit young men and women was around 15and 25%, respectively (114,119). With consideration toa normal curve distribution in body composition, this sug-gested that desirable body fat limits for active young menand women should fall around 20 and 30%, for men andwomen. Individuals above this level would have to engagein remedial training and weight loss or be separated fromthe military. Body weight or BMI only started an individualinto the process and body fat became the standard. Thereport recommended acknowledgment of an aging effecton body composition relationships to fitness, with addi-tional leeway for older service members. These recommen-ded thresholds ranged up to 37% body fat for the oldest agegroup of women (114).
TABLE 1. Body mass index thresholds andpercent body fat standards currently used bythe U.S. Army (5,74).
Age category (y)Body mass index
(kg$m22)†Relative body
fat (%)
Men,21 25.9 2021–27 26.5 2228–39 27.2 24.40z 27.5 26
Women,21 25.0 3021–27 25.3 3228–39 25.6 34.40z 26.0 36
†The Army regulation uses tabled values rounded fromthese body mass index thresholds (AR 600-9).
zThe upper limits of body mass index permitted in theDoD instruction (DODI 1308.3, DoD Physical Fitness andBody Fat Programs Procedures, November 5, 2002) are25–27.5 kg$m22 for both sexes. Permissible body fatstandards are 26–36% for women and 18–26% formen. Other military services use different age categoriesand limits within the permissible ranges.
Military Body Fat Standards
S88 Journal of Strength and Conditioning Researchthe TM
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.

Gender-appropriate, rather than gender-neutral, standardsfor body composition were established, recognizing funda-mental endocrine physiology, and human sexual dimorphism.However, in the translation between the recommendations ofthe panel (114) and the DoD Instruction, there was an ad-justment to tighten the womens’ standards. This was basedon a prevailing misperception that, in terms of physical per-formance, women were basically men with too much bodyfat, and their performance might come closer to that of themale counterparts if they were held to leaner standards.Screening weights and body fat standards were later amendedin a revision of the Army Regulation and the DoD Directiveto the original recommendations, based on data that showedhow female soldier health and performance was impaired byinappropriately stringent body fat standards (5,34,38). Thereis clearly a weight penalty for additional sex-specific fat thataffects running and marching performance (14). However,there is also a more enlightened understanding that femalephysiology has its own performance advantages, particularlyin estrogen-regulated fat metabolism (59,111,112).
BODY SIZE AND STRENGTH REQUIREMENTS
In addition to the general body fat standards applicable to allsoldiers, there are also physical standards specific to militaryoccupational specialties (MOS). Previously, these werefocused on strength requirements associated with specifictasks in the specialties such as ability to lift kettles of foodand handle fire hoses (46). These MOS-specific standardshave been revised over time and today include primarilyheight standards such as minimum heights for man portable
field artillery system crewmem-bers (6400) and maximumheights for armor crewmem-bers (7300) based on human lim-itations of engineered systems.Earlier strength requirementswere abandoned because itwas recognized that specificthresholds for individual char-acteristics or capabilities werenot defining limitations in mili-tary job specialties, especiallyconsidering the complexity ofmodern jobs and team efforts,and with changes in safety andefficiency offered by reengin-eering tasks and equipment.This represents a significantshift in common perceptionsthat massive soldiers are thebest soldiers and recognitionthat other soldier characteris-tics are at least equally impor-tant to mission success.Consistent with this thinking,
the Army research investment has been in “skin-out” tech-nologies such as exoskeletons and jet packs to provide Su-perman performance rather than attempts to produce anArmy of massive soldiers through very narrow genetic selec-tion or through genetic manipulation of myostatin or othermusculotrophic regulators (30).
A large effort to classify job strength requirements andthen classify eligible candidates by minimum strengthcapability with an upright lift test in the recruit processingcenters failed because of testing safety concerns that reducedthe rigor of the test and changed the results to job advisoryguidance rather than requirements (67,113,121). The Assis-tant Secretary of the Army for Manpower and ReserveAffairs, Ms. Sara Lister, challenged Army researchers to findany conclusive evidence that physical strength had relevanceto job selection criteria. This eventually led to a comprehen-sive study of one military job specialty (wheeled vehiclemechanics) to determine if body weight and strength meas-ures were related to injury risk. Injuries provided a morequantifiable outcome measure than “job performance” andrepresented an aspect of military job performance. Wheeledvehicle mechanics were chosen because they have one of thehighest injury rates for men and women. The results indi-cated that the leading cause of injuries was physical fitnesstraining (notably, running), rather than job-specific mechan-ical work. Although the female soldiers were smaller andweaker on average than the males, men had the highest ratesof traumatic injury and men with a higher BMI were atgreater risk for sustaining an injury than the smaller men(66). The results of this study highlight the complexity
Figure 1. Do we want “pretty” or healthy? Body fat standards are strictest if based on prevailing perceptions ofmilitary appearance and most liberal if based on estimates of health risk thresholds. Optimal body composition formany types of physical performance fall somewhere between these extremes of leanness and tolerable fatness.
Journal of Strength and Conditioning Researchthe TM
| www.nsca.com
VOLUME 26 | SUPPLEMENT 7 | JULY 2012 | S89
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
of soldier physical demands and the difficulty in assigningspecific physical strength or lean mass requirements forany MOS.
Nevertheless, many Army tasks involve a strength com-ponent, and minimum strength requirements are presumedto reduce injury rates (51,121). These strength require-ments are addressed through semiannual physical fitnesstesting (push-ups and sit-ups) (115) and minimum weightrecruitment standards. World War II data established theimportance of body size, representing lean tissue, in workcapacity and energy requirements (107). However, furtherprecision in defining absolute strength (or related leanmass) requirements have not proven feasible. Currententry standards require a minimum BMI of 19 kg$m22,based on WHO classification of the lower limit ofnormal weight; severe thinness by WHO classification is16 kg$m22, and 12 kg$m22 is approximately the lower limit
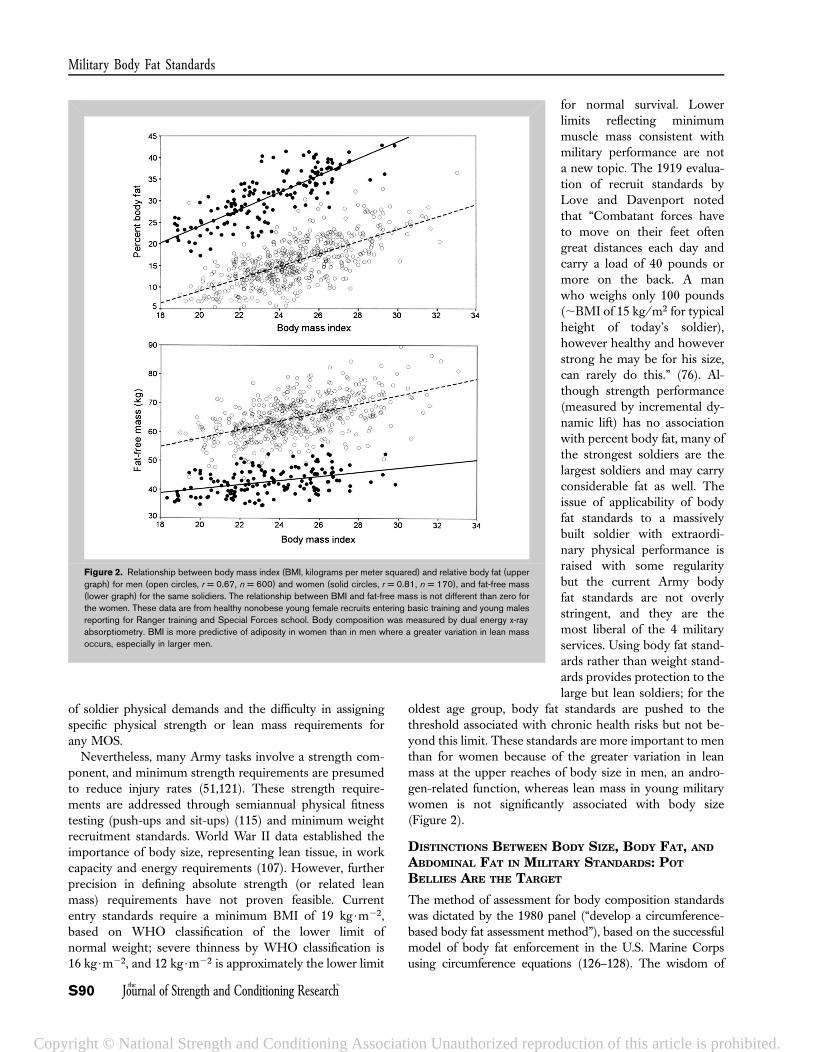
for normal survival. Lowerlimits reflecting minimummuscle mass consistent withmilitary performance are nota new topic. The 1919 evalua-tion of recruit standards byLove and Davenport notedthat “Combatant forces haveto move on their feet oftengreat distances each day andcarry a load of 40 pounds ormore on the back. A manwho weighs only 100 pounds(;BMI of 15 kg/m2 for typicalheight of today’s soldier),however healthy and howeverstrong he may be for his size,can rarely do this.” (76). Al-though strength performance(measured by incremental dy-namic lift) has no associationwith percent body fat, many ofthe strongest soldiers are thelargest soldiers and may carryconsiderable fat as well. Theissue of applicability of bodyfat standards to a massivelybuilt soldier with extraordi-nary physical performance israised with some regularitybut the current Army bodyfat standards are not overlystringent, and they are themost liberal of the 4 militaryservices. Using body fat stand-ards rather than weight stand-ards provides protection to thelarge but lean soldiers; for the
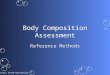
oldest age group, body fat standards are pushed to thethreshold associated with chronic health risks but not be-yond this limit. These standards are more important to menthan for women because of the greater variation in leanmass at the upper reaches of body size in men, an andro-gen-related function, whereas lean mass in young militarywomen is not significantly associated with body size(Figure 2).
DISTINCTIONS BETWEEN BODY SIZE, BODY FAT, AND
ABDOMINAL FAT IN MILITARY STANDARDS: POT
BELLIES ARE THE TARGET
The method of assessment for body composition standardswas dictated by the 1980 panel (“develop a circumference-based body fat assessment method”), based on the successfulmodel of body fat enforcement in the U.S. Marine Corpsusing circumference equations (126–128). The wisdom of
Figure 2. Relationship between body mass index (BMI, kilograms per meter squared) and relative body fat (uppergraph) for men (open circles, r = 0.67, n = 600) and women (solid circles, r = 0.81, n = 170), and fat-free mass(lower graph) for the same solidiers. The relationship between BMI and fat-free mass is not different than zero forthe women. These data are from healthy nonobese young female recruits entering basic training and young malesreporting for Ranger training and Special Forces school. Body composition was measured by dual energy x-rayabsorptiometry. BMI is more predictive of adiposity in women than in men where a greater variation in lean massoccurs, especially in larger men.
Military Body Fat Standards
S90 Journal of Strength and Conditioning Researchthe TM
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.

this panel, which had to make recommendations with limitedavailable data, has been borne out over the ensuing 3 deca-des. The move away from body size to a focus on abdominalcircumference was ahead of its time (31,62,73,103). Theinsurance industry had long been predicting mortality riskfrom girth (44), but WC has since emerged as a key markerof many undesirable body composition-related outcomes.Abdominal circumference has also proven to be a practicalmethod for widespread use by nontechnical users, and turn-ing out to be superior to sophisticated state-of-the-art scien-tific methods of body fat assessment in regards to theoutcomes of military interest. Specifically, a very accuratetotal body fat measurement is not nearly as important tothe military standard as an abdominal circumference. Thetarget of each of the outcomes of interest is intraabdominalfat. This is also one of the more labile fat depots under con-trol of the service member through exercise and nutritionalhabits. Furthermore, the circumference-based method isblind to genetic variations in subcutaneous fat distributionelsewhere on the body making it fairer and not raciallybiased (28,71).
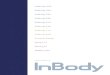
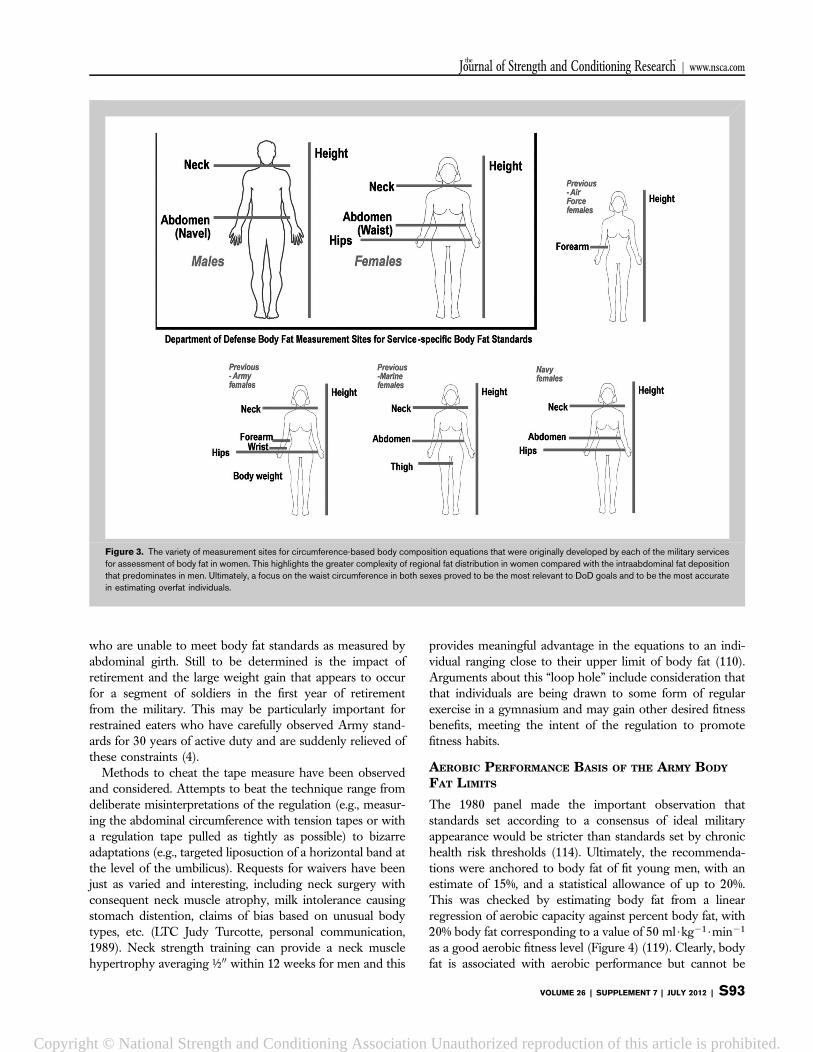
The U.S. military has a long investment in the area ofbody composition and performance. This includes earlydevelopment of some of the body composition measurementtechnologies including underwater weighing, body waterdilution, whole-body plethysmography, bioelectric imped-ance, caliper-measured skinfold thicknesses, and abdominalcircumference (Table 2). It also includes a long history ofinitiatives and studies that were driven by national securityissues. The criterion method against which the current mil-itary body fat equations were developed was underwaterweighing (53,54), but this has since been revalidated inmultiple studies using 3 and 4 compartment models usingdual-energy x-ray absorptiometry (DXA) technology andmethods of body water estimation (57,71,117). Each methodof body fat estimation is based on factors and principals thatmake comparison between methods problematic. The mostaccurate assessments in living humans come from combiningmethods that measure specific chemical compartments suchas body water, bone, fat, and everything else or additionalelemental components) (32,52). It must be reiterated thatthis greater accuracy in body fat estimation is not preferableto WC-based estimations for military body compositionstandards, for reasons discussed in the previous paragraph.The method is necessarily part of the standard and servicemembers are not permitted to shop for a method that pro-vides a lower estimate. Originally, each of the 4 militaryservices had different circumference-based circumferencemethods that gave very different assessments because ofthe differences in measurement sites, especially for womenwhere there are more choices for regional fat deposition(Figure 3) (42). Although the methods were applied consis-tently within each military service, the differences called intoquestion the scientific basis of all of the standards and led tothe adoption of a single best set of equations for men and
women, the Hodgdon equations, developed by the Navy(43,53,54). The Defense Advisory Committee on Womenin the Services demanded further investigation of the meth-odology with the goal of a single unisex equation for bodyfat prediction, but this yielded only poorer body fat predic-tion for both men and women (Hodgdon, J, unpublishedresults, 1996).
The performance of anthropometrically based equationsin longitudinal studies has not been well established (64,130).The subcutaneous fat layer could be reasonably hypothe-sized to adjust to fat loss at a slower rate than the morelabile intraabdominal fat stores; thus, skinfold thicknessmeasurements could be less sensitive to change than anabdominal circumference. The WC-based military equationsare relatively sensitive to changes in criterion-measured bodyfat for male and female soldiers during basic training andmale soldiers during Ranger training (35,36,39,98). TheArmy regulation also takes into account the variability ofthe measurement error (61% body fat), allowing for prog-ress of overfat soldiers to be recognized by monthly changesin weight or fat changes of 1% body fat or more. This isdifferent than the 63% body fat error of the estimate com-pared with criterion methods, which is assumed not to bean additional error in monthly measurements of the sameindividual (27,37). Regardless of the actual reliability of fatchanges assessed by WC (and hip circumference, forwomen), the standard is ultimately based on waist girthand not total body fat loss.
The circumference-based body fat standards have alsobeen examined for their long-term effects on the population,but these effects are difficult to separate from national trendsin weight gain. The average girth of male soldiers in their 20sincreased by at approximately 200 (5 cm) between the start ofthe Army body composition standards enforcement in 1984and a survey conducted in 2000; however, the impact of theexisting weight control standards on limiting this increasecould not be determined (28). For comparison, the WC ofmen aged 20–29 years in the U.S. population (measured atabdominal midpoint rather than the military standard of theumbilicus) also increased by approximately 200 between the1988–1994 and 1999–2000 National Health and NutritionExamination Survey survey (25). In U.S. and Finnish studies,there has been a trend for young soldiers to increase in BMIand body fat and for a decline in physical fitness levels(99,105). The older career soldiers remained unchangedand slightly below their upper limits of WC. Career soldierswere examined in a study at the U.S. Army Sergeants MajorAcademy (Fort Bliss, TX, USA) that compared circumfer-ence determined body fat and DXA measurements. Manyolder soldiers carried high total body fat as measured byDXA but maintained abdominal circumferences withinstandards for the Army body fat standards (28). This canbe explained by some combination of the effect of exerciseand nutrition habits on maintaining low abdominal girthrelative to total body fat and earlier elimination of individuals
Journal of Strength and Conditioning Researchthe TM
| www.nsca.com
VOLUME 26 | SUPPLEMENT 7 | JULY 2012 | S91
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
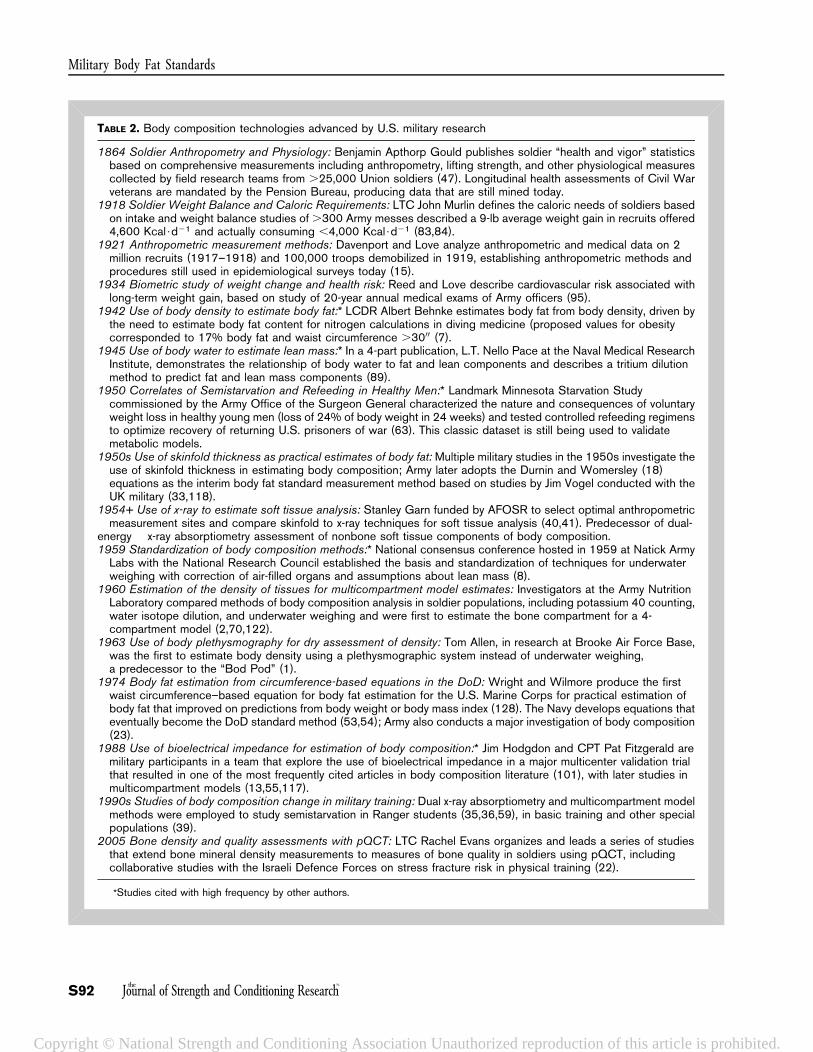
TABLE 2. Body composition technologies advanced by U.S. military research
1864 Soldier Anthropometry and Physiology: Benjamin Apthorp Gould publishes soldier “health and vigor” statisticsbased on comprehensive measurements including anthropometry, lifting strength, and other physiological measurescollected by field research teams from .25,000 Union soldiers (47). Longitudinal health assessments of Civil Warveterans are mandated by the Pension Bureau, producing data that are still mined today.
1918 Soldier Weight Balance and Caloric Requirements: LTC John Murlin defines the caloric needs of soldiers basedon intake and weight balance studies of .300 Army messes described a 9-lb average weight gain in recruits offered4,600 Kcal$d21 and actually consuming ,4,000 Kcal$d21 (83,84).
1921 Anthropometric measurement methods: Davenport and Love analyze anthropometric and medical data on 2million recruits (1917–1918) and 100,000 troops demobilized in 1919, establishing anthropometric methods andprocedures still used in epidemiological surveys today (15).
1934 Biometric study of weight change and health risk: Reed and Love describe cardiovascular risk associated withlong-term weight gain, based on study of 20-year annual medical exams of Army officers (95).
1942 Use of body density to estimate body fat:* LCDR Albert Behnke estimates body fat from body density, driven bythe need to estimate body fat content for nitrogen calculations in diving medicine (proposed values for obesitycorresponded to 17% body fat and waist circumference .3000 (7).
1945 Use of body water to estimate lean mass:* In a 4-part publication, L.T. Nello Pace at the Naval Medical ResearchInstitute, demonstrates the relationship of body water to fat and lean components and describes a tritium dilutionmethod to predict fat and lean mass components (89).
1950 Correlates of Semistarvation and Refeeding in Healthy Men:* Landmark Minnesota Starvation Studycommissioned by the Army Office of the Surgeon General characterized the nature and consequences of voluntaryweight loss in healthy young men (loss of 24% of body weight in 24 weeks) and tested controlled refeeding regimensto optimize recovery of returning U.S. prisoners of war (63). This classic dataset is still being used to validatemetabolic models.
1950s Use of skinfold thickness as practical estimates of body fat: Multiple military studies in the 1950s investigate theuse of skinfold thickness in estimating body composition; Army later adopts the Durnin and Womersley (18)equations as the interim body fat standard measurement method based on studies by Jim Vogel conducted with theUK military (33,118).
1954+ Use of x-ray to estimate soft tissue analysis: Stanley Garn funded by AFOSR to select optimal anthropometricmeasurement sites and compare skinfold to x-ray techniques for soft tissue analysis (40,41). Predecessor of dual-
energy x-ray absorptiometry assessment of nonbone soft tissue components of body composition.1959 Standardization of body composition methods:* National consensus conference hosted in 1959 at Natick ArmyLabs with the National Research Council established the basis and standardization of techniques for underwaterweighing with correction of air-filled organs and assumptions about lean mass (8).
1960 Estimation of the density of tissues for multicompartment model estimates: Investigators at the Army NutritionLaboratory compared methods of body composition analysis in soldier populations, including potassium 40 counting,water isotope dilution, and underwater weighing and were first to estimate the bone compartment for a 4-compartment model (2,70,122).
1963 Use of body plethysmography for dry assessment of density: Tom Allen, in research at Brooke Air Force Base,was the first to estimate body density using a plethysmographic system instead of underwater weighing,a predecessor to the “Bod Pod” (1).
1974 Body fat estimation from circumference-based equations in the DoD: Wright and Wilmore produce the firstwaist circumference–based equation for body fat estimation for the U.S. Marine Corps for practical estimation ofbody fat that improved on predictions from body weight or body mass index (128). The Navy develops equations thateventually become the DoD standard method (53,54); Army also conducts a major investigation of body composition(23).
1988 Use of bioelectrical impedance for estimation of body composition:* Jim Hodgdon and CPT Pat Fitzgerald aremilitary participants in a team that explore the use of bioelectrical impedance in a major multicenter validation trialthat resulted in one of the most frequently cited articles in body composition literature (101), with later studies inmulticompartment models (13,55,117).
1990s Studies of body composition change in military training: Dual x-ray absorptiometry and multicompartment modelmethods were employed to study semistarvation in Ranger students (35,36,59), in basic training and other specialpopulations (39).
2005 Bone density and quality assessments with pQCT: LTC Rachel Evans organizes and leads a series of studiesthat extend bone mineral density measurements to measures of bone quality in soldiers using pQCT, includingcollaborative studies with the Israeli Defence Forces on stress fracture risk in physical training (22).
*Studies cited with high frequency by other authors.
Military Body Fat Standards
S92 Journal of Strength and Conditioning Researchthe TM
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
who are unable to meet body fat standards as measured byabdominal girth. Still to be determined is the impact ofretirement and the large weight gain that appears to occurfor a segment of soldiers in the first year of retirementfrom the military. This may be particularly important forrestrained eaters who have carefully observed Army stand-ards for 30 years of active duty and are suddenly relieved ofthese constraints (4).
Methods to cheat the tape measure have been observedand considered. Attempts to beat the technique range fromdeliberate misinterpretations of the regulation (e.g., measur-ing the abdominal circumference with tension tapes or witha regulation tape pulled as tightly as possible) to bizarreadaptations (e.g., targeted liposuction of a horizontal band atthe level of the umbilicus). Requests for waivers have beenjust as varied and interesting, including neck surgery withconsequent neck muscle atrophy, milk intolerance causingstomach distention, claims of bias based on unusual bodytypes, etc. (LTC Judy Turcotte, personal communication,1989). Neck strength training can provide a neck musclehypertrophy averaging ½00 within 12 weeks for men and this
provides meaningful advantage in the equations to an indi-vidual ranging close to their upper limit of body fat (110).Arguments about this “loop hole” include consideration thatthat individuals are being drawn to some form of regularexercise in a gymnasium and may gain other desired fitnessbenefits, meeting the intent of the regulation to promotefitness habits.
AEROBIC PERFORMANCE BASIS OF THE ARMY BODY
FAT LIMITS
The 1980 panel made the important observation thatstandards set according to a consensus of ideal militaryappearance would be stricter than standards set by chronichealth risk thresholds (114). Ultimately, the recommenda-tions were anchored to body fat of fit young men, with anestimate of 15%, and a statistical allowance of up to 20%.This was checked by estimating body fat from a linearregression of aerobic capacity against percent body fat, with20% body fat corresponding to a value of 50 ml$kg21$min21
as a good aerobic fitness level (Figure 4) (119). Clearly, bodyfat is associated with aerobic performance but cannot be
Figure 3. The variety of measurement sites for circumference-based body composition equations that were originally developed by each of the military servicesfor assessment of body fat in women. This highlights the greater complexity of regional fat distribution in women compared with the intraabdominal fat depositionthat predominates in men. Ultimately, a focus on the waist circumference in both sexes proved to be the most relevant to DoD goals and to be the most accuratein estimating overfat individuals.
Journal of Strength and Conditioning Researchthe TM
| www.nsca.com
VOLUME 26 | SUPPLEMENT 7 | JULY 2012 | S93
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
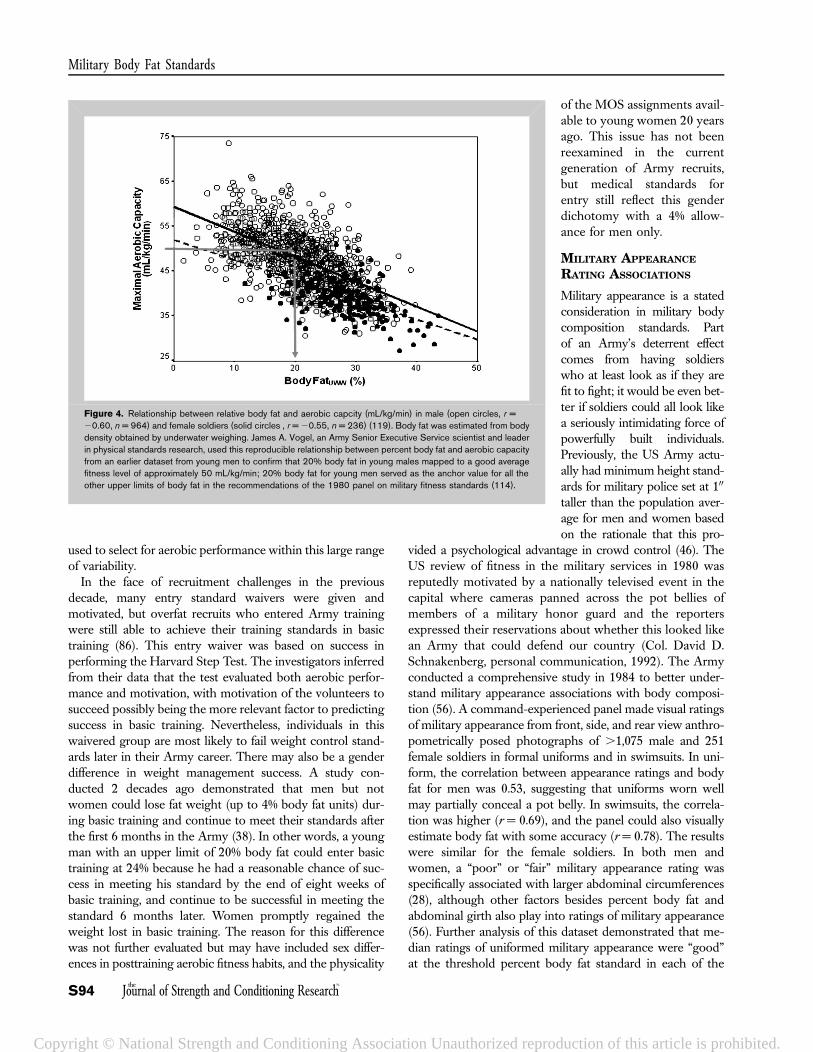
used to select for aerobic performance within this large rangeof variability.
In the face of recruitment challenges in the previousdecade, many entry standard waivers were given andmotivated, but overfat recruits who entered Army trainingwere still able to achieve their training standards in basictraining (86). This entry waiver was based on success inperforming the Harvard Step Test. The investigators inferredfrom their data that the test evaluated both aerobic perfor-mance and motivation, with motivation of the volunteers tosucceed possibly being the more relevant factor to predictingsuccess in basic training. Nevertheless, individuals in thiswaivered group are most likely to fail weight control stand-ards later in their Army career. There may also be a genderdifference in weight management success. A study con-ducted 2 decades ago demonstrated that men but notwomen could lose fat weight (up to 4% body fat units) dur-ing basic training and continue to meet their standards afterthe first 6 months in the Army (38). In other words, a youngman with an upper limit of 20% body fat could enter basictraining at 24% because he had a reasonable chance of suc-cess in meeting his standard by the end of eight weeks ofbasic training, and continue to be successful in meeting thestandard 6 months later. Women promptly regained theweight lost in basic training. The reason for this differencewas not further evaluated but may have included sex differ-ences in posttraining aerobic fitness habits, and the physicality
of the MOS assignments avail-able to young women 20 yearsago. This issue has not beenreexamined in the currentgeneration of Army recruits,but medical standards forentry still reflect this genderdichotomy with a 4% allow-ance for men only.
MILITARY APPEARANCE
RATING ASSOCIATIONS
Military appearance is a statedconsideration in military bodycomposition standards. Partof an Army’s deterrent effectcomes from having soldierswho at least look as if they arefit to fight; it would be even bet-ter if soldiers could all look likea seriously intimidating force ofpowerfully built individuals.Previously, the US Army actu-ally had minimum height stand-ards for military police set at 100
taller than the population aver-age for men and women basedon the rationale that this pro-
vided a psychological advantage in crowd control (46). TheUS review of fitness in the military services in 1980 wasreputedly motivated by a nationally televised event in thecapital where cameras panned across the pot bellies ofmembers of a military honor guard and the reportersexpressed their reservations about whether this looked likean Army that could defend our country (Col. David D.Schnakenberg, personal communication, 1992). The Armyconducted a comprehensive study in 1984 to better under-stand military appearance associations with body composi-tion (56). A command-experienced panel made visual ratingsof military appearance from front, side, and rear view anthro-pometrically posed photographs of .1,075 male and 251female soldiers in formal uniforms and in swimsuits. In uni-form, the correlation between appearance ratings and bodyfat for men was 0.53, suggesting that uniforms worn wellmay partially conceal a pot belly. In swimsuits, the correla-tion was higher (r = 0.69), and the panel could also visuallyestimate body fat with some accuracy (r = 0.78). The resultswere similar for the female soldiers. In both men andwomen, a “poor” or “fair” military appearance rating wasspecifically associated with larger abdominal circumferences(28), although other factors besides percent body fat andabdominal girth also play into ratings of military appearance(56). Further analysis of this dataset demonstrated that me-dian ratings of uniformed military appearance were “good”at the threshold percent body fat standard in each of the
Figure 4. Relationship between relative body fat and aerobic capcity (mL/kg/min) in male (open circles, r =20.60, n = 964) and female soldiers (solid circles , r = 20.55, n = 236) (119). Body fat was estimated from bodydensity obtained by underwater weighing. James A. Vogel, an Army Senior Executive Service scientist and leaderin physical standards research, used this reproducible relationship between percent body fat and aerobic capacityfrom an earlier dataset from young men to confirm that 20% body fat in young males mapped to a good averagefitness level of approximately 50 mL/kg/min; 20% body fat for young men served as the anchor value for all theother upper limits of body fat in the recommendations of the 1980 panel on military fitness standards (114).
Military Body Fat Standards
S94 Journal of Strength and Conditioning Researchthe TM
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.

Army age groups for men and women until the oldest group.The oldest soldiers had median appearance ratings of only“fair” as they approached the health-based upper limits ofbody fat allowance; thus, military appearance dictates a morestringent body fat standard than health risk thresholds (Col.Karl E. Friedl, unpublished results, 1990).
CHRONIC HEALTH RISK ASSOCIATIONS
For upper limits of body fat standards at the oldest agegroups, thresholds of 26 and 36% body fat were set froma variety of comparisons to epidemiological studies (Table 1),with the strongest data from type 2 diabetes and overweightassociations (31,90). The screening weights that triggera body fat measurement in the Army regulation are BMIof 27.5 kg$m22 (men) and 25.0 kg$m22 (women) (Table 1).The body fat thresholds correspond to WCs of 38.500 and35.000 for the typical male and female soldier, respectively(31). Thus, the most liberal Army body composition stand-ards, those applied to soldiers over age 40, map to health riskthresholds including an approximation of the NHLBI guide-lines for healthy body composition (BMI , 25 kg$m22;WC , 4000 [men] and ,3500 [women]). Screening weightsare higher than BMI 25 for Army men; soldiers are larger butleaner than the typical U.S. male because of selection andbecause of the emphasis on fitness and enforced fitness test-ing standards. If the male screening weight tables used anupper limit of BMI 25 kg$m22, more than half of the Armywould also have to be measured for body fat in every semi-annual evaluation required by the regulation. Thus, screeningweights extend up to BMI 27.5 kg$m22 for male soldiers.
There is a general perception that massively large menmust carry significant health risks no matter how their fat isdistributed. Although this may be true for factors such asosteoarthritis that are suspected of an association withbiomechanical stress from increasing mass regardless ofwhether it is from muscle or fat, it is not necessarily truefor cardiovascular and metabolic risks. Matsuzawa et al. (77)highlighted this in a very interesting analysis of fat distribu-tion and health risks in sumo wrestlers with BMI exceeding35 kg$m22. This study demonstrated large differences inCT-imaged intraabdominal fat distribution associated withmarked differences in biochemical health risk profiles.
Although BMI might effectively identify overfat womenwhere there is no statistically significant relationship betweenincreasing BMI and lean mass, there is a highly significantincrease in lean mass for men and greater variability in theiradiposity with increasing BMI (Figure 2). In any case,WC-based body fat estimation is much better associated withmale and female chronic health risks than total body fat, bodyweight, or body size (BMI) (28). Even for women, intraabdo-minal fat becomes an issue above a certain threshold ofadiposity. Kvist et al. (72) demonstrated a linear increase inintraabdominal fat with increasing adiposity in men. Inwomen, intraabdominal fat remained at a minimal level withincreasing fatness until an accumulation of 30 L (;27 kg) of
total body fat, at which point a steady increase in intraabdo-minal accumulation began. Fat deposition in other subcuta-neous sites in women, including arms, legs, buttocks, andbreast are not generally associated with health risks and insome cases may reflect an association with reduced cardio-vascular and other health risks. Intraabdominal fat (detectedby WC), on the other hand, is strongly associated withincreasing health risks in women as it is with men (31).
At present, there is no plausible rationale for a morelenient WC or body fat standard than this current U.S. Armyupper limit for men and women. A better understanding ofthe interaction between physical activity and adipose tissuephysiology (i.e., “fit fat”) could change this. A proposal tolink Army physical fitness test performance with body fatstandards, allowing a sliding scale for body fat limits in theyounger age categories (74), was carefully evaluated butultimately deemed too complicated to implement (LTGTimothy J. Maude, personal communication, 2001). Stricterstandards are conceivable for other populations character-ized by slighter body builds. In 2008, Japan adopted WClimits for men and women between age 40 and 74 years withmeasurements that trigger weight management interven-tions at 33.500 (men) and 35.400 (women) (88). Argumentshave been made for body composition standards to beadjusted to correspond to national weight gain trends asthe Army should reflect the national population from whichrecruits are drawn. Such an adjustment, or the suspension ofbody fat standards, would signal a deliberate acceptance oflower fitness and health standards. Some armies, such as thePeople’s Republic of China, have been forced to ease weightstandards for recruits to reflect population trends that reflectrecruit availability (91). The good news for recruiters inwestern Armies is that the increase in BMI in several othercountries with weight and health monitoring statisticspeaked around 2000 and appears to have leveled off. Thereason for this plateau in obesity rate is unexplained (87).
OTHER HEALTH AND PERFORMANCE ASSOCIATIONS
AND IMPACTS
A central tenet behind the military body fat standards is theuse of these standards to drive fitness and nutrition habits. Thestandards are only fair if healthy men and women canreasonably attain and maintain the standards through per-sonal habits. This is a critically important point and one thatagain points to the relevance of the abdominal circumferenceas a key component of the military standards because this isone of the most labile sites of fat deposition. Intraabdominalfat as reflected by WC is sensitive to exercise and dietarycontrol (16,17,36,50,97). Other sites of fat deposition such asthigh fat have a lower responsiveness to lipogenic factors andappear to be relatively stable and immovable (94).
Weight gain after smoking cessation has been a concernexpressed by some soldiers considering giving up cigarettes.This represents a tradeoff between 2 different types of healthrisks; however, earlier data have also suggested that smokers
Journal of Strength and Conditioning Researchthe TM
| www.nsca.com
VOLUME 26 | SUPPLEMENT 7 | JULY 2012 | S95
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.

have an altered distribution of fat storage, with a higher waistgirth (106). For some individuals, nicotine suppression oflipoprotein lipase may result in a rebound expression ofthe enzyme when they quit smoking, leading to increasedtriglyceride storage in adipose tissue (11). An existing data-base of soldier data was used to test the effect of cigarettesmoking on WC, skinfold thickness, overall fatness, aerobicperformance, and lifting strength; aerobic fitness was signif-icantly lower in smokers (COL Daniels, W, unpublishedresults, 1994), but it was also noted that smokers were leaner(;3% body fat) in each age group compared with non-smokers (COL Friedl, KE, unpublished results, 2003).
Intraabdominal fat distribution is commonly cited asa physiological marker of chronic psychological stress,particularly the influence of a chronic activation of thehypothalamic-pituitary-adrenal axis (100). This is supportedby experiments with animals where abdominal fat is specif-ically reduced by administration of RU486, a drug thatblocks the effects of adrenal stress hormones on adipocytes(6). Trauma spectrum disorder related to current combatdeployments may also be a critical factor in weight gain fromdisordered eating and other behavioral changes observed insome soldiers (61). Certain drugs such as protease inhibitors(e.g., indinavir) also have specific effects on increasingintraabdominal fat distribution (82). In men, the role oftestosterone and dihydrotestosterone has been well inves-tigated and aging-related reductions in testosterone in menare associated with an increased intraabdominal fat distri-bution (78,79). This effect has also been demonstrated inshorter term studies with artificial reduction of testosterone(125). Fat is mobilized from all stores (intraabdominal, sub-cutaneous, intermuscular), especially in intermuscular fatdepots, in men with high dose testosterone administration,along with increases in lean mass (125). Androgen effects inwomen have been well studied for conditions such as poly-cystic ovary syndrome and associated overweight and up-per body fat (“android”) distribution. Androgenicityincreases male-type health risks and fat distribution andalso increases male-type strength and training responses(3,68,69,21,102,116).
Important in utero effects were discovered through anobservation that a cohort of overweight Dutch Army con-scripts were sons of women who had been chronicallymalnourished in early pregnancy during the wartime blockadeof northern Holland, referred to as the Dutch “Hungerwinter”(93). This effect of semistarvation during early pregnancy hassince been further studied in animals, with a postpartumalteration in brain appetite centers that result in a chronichyperphagia and excessive fat weight gain. It has since beenconfirmed in other human disasters such as the Biafran war(60). This points to another potential harm from overly strin-gent female body composition standards that may causeexcessive dietary restriction during pregnancy. Ironically,proud young female soldiers seeking to minimize gestationalweight gain are more likely to produce obese offspring.
Weight management and physical fitness habits areinterrelated and, somewhere in this interrelationship, arebenefits to the brain. This is seen repeatedly in epidemiolog-ical studies of general health such as illness rates and BMIassociations (48) and aerobic exercise and pain perception andother symptom complaints (45). Other findings are highlight-ing the importance of weight management and fitness habitsto long-term health associations with neurodegenerative dis-eases such as Alzheimer’s and Parkinson’s disease (12,65).Thus, as jobs become more technical and cognitively de-manding but possibly less physically demanding, the valueof fitness and nutrition habits continue to be important (75).
OTHER INFLUENCESdHOW MUCH FAT IS USEFUL?
Body size has been a factor in logistical considerations, withlarge soldiers having higher metabolic requirements thansmaller soldiers do. This is the basis of the Military DietaryReference Intakes for male and female soldiers (2,300 vs.3,250 kcal). It has been impractical to produce a “pink ration”with adequate nutrients but lower energy content for womenbut there has been a better effort to educate and inform (e.g.,with ration labeling) so that women can make more appro-priate food choices from the nearly 4,000 Kcal$d21 opera-tional rations (29). Even in World War I, there wasconsideration to providing different rations for groups ofmale soldiers organized into units by different Europeanethnic origins, based on the perception that some groupsrequired more calories than others (67).
Clearly, more fat is advantageous in a starvation situation.This gives female soldiers a survival advantage over malesoldiers, both because of larger sex-specific fat stores and alsobecause of more efficient fat metabolism. A greater proportionof Russian women survived the Siege of Stalingrad than didmen (9). In high stress military training with no food fora week, women were more efficient in fat energy metabolismthan were the men (59). In an extended semistarvation, sol-diers nearing the limits of accessible fat reserves sacrificeincreasing amounts of lean mass and sacrifice strength perfor-mance; the more extreme fat losses begin to affect fat pads onthe soles of the feet making even walking painful (36).
The adaptive role of fat in sensitivity, performance, andsurvival in the cold has been well studied and modeled bythermal physiologists, with low body fat individuals atsignificantly disadvantage (10,92,129). Distance cold waterswimmers have high insulative fat levels while Ama pearldivers, known for their extended endurance dives in coldwater, appear to have metabolic adaptations rather thanhigher insulative fat (58). The role of brown adipose tissuein thermogenesis and lifetime weight maintenance and glu-cose disposal makes this a potential intervention target ofinterest to military medical research.
FUTURE DIRECTIONS
The important research to be done in military weightcontrol programs is on how to provide effective assistance
Military Body Fat Standards
S96 Journal of Strength and Conditioning Researchthe TM
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.

to soldiers who are motivated to meet and maintain stand-ards. Training service members and their family members inhow to choose and prepare satisfying but healthy meals isone piece of the intervention. Teaching soldiers sensibleapproaches to physical activity without incurring significantinjuries, including overuse injuries, is another. Today’s sol-diers use everyday technologies such as smartphones andexpect to receive information and training through thesetechnologies. Sophisticated metabolic models can now bebrought to bear behind simple inputs and outputs for smartfood and exercise choices (49). With the Pennington Bio-medical Research Center, the Army has developed an inter-net-based program that provides such choices (108,109,124).This is part of the weight management intervention in a cur-rent statewide randomized control trial with the LouisianaArmy National Guard (85). Smartphone technologies canprovide biomonitoring feedback to individuals through mea-sured activity patterns and other sensing. For example, theNokia Activity Monitor in the Nokia S60 phone has anaccelerometer that can capture daily voluntary activity dis-played for the user for days and months of activity patterns.A wide array of technology opportunities exist as high-lighted in a recent special workshop on this topic betweenTATRC and the National Science Foundation (19,20), withmany of these currently being tested in related health andweight management applications.
CONCLUSIONS
The Army body fat standards and screening weights havenot substantially changed since 1983. Constant reevaluationof the standards with new data has reaffirmed that theseupper limits are about right in terms of key outcomes(physical performance, military appearance, and chronichealth risk) and fairness. Military body composition stand-ards are not intended to predict performance; they areintended to motivate fitness and nutrition habits thatpromote individual physical readiness. Regular physicalactivity, good nutrition, and weight management provideextensive health and performance benefits including physicaland mental performance and resistance to disease. Excessivefat, particularly intraabdominal fat, is associated withincreased health risk and poor military appearance (the“pot belly”). This distribution of body fat is particularly sus-ceptible to environmental influences such as exercise anddietary control but is also affected by stress hormones andother metabolic factors. Fat-free mass is an important com-ponent associated with strength and work capacity. Mini-mum levels of fat-free mass, accurately reflected in bodyweight of very light weight individuals, are important toinjury prevention, especially in tasks that require strength.The BMI and WC thresholds related to these standardsapproximate emerging data on health, performance, andappearance. Current research gaps center on effective weightmanagement interventions to help soldiers achieve and sus-tain good nutrition and fitness habits throughout their lives.
REFERENCES
1. Allen, TH. Measurement of human body fat. A quantitativemethod suitable for use by aviation medical officers. Aerosp Med 34:907–909, 1963.
2. Allen, TH, Welch, BE, Trujillo, TT, and Roberts, JE. Fat, water andtissue solids of the whole body less its bone mineral. J Appl Physiol14: 1009–1012, 1959.
3. Andersson, B, Xu, X, Rebuffe-Scrive, M, Terning, K,Krotkiewski, M, and Bjorntorp, P. The effects of exercise trainingon body composition and metabolism in men and women. Int JObes 15: 75–81, 1991.
4. Bathalon, GP, Hays, NP, McCrory, MA, Vinken, AG, Tucker, KL,Greenberg, AS, Castaneda, C, and Roberts, SB. The energyexpenditure of postmenopausal women classified as restrained orunrestrained eaters. Eur J Clin Nutr 55: 1059–1067, 2001.
5. Bathalon, GP, McGraw, SM, Sharp, MA, Williamson, DA,Young, AJ, and Friedl, KE. The effect of proposed improvements tothe Army Weight Control Program on female soldiers. Mil Med171: 800–806, 2006.
6. Beebe, KL, Block, T, Debattista, C, Blasey, C, and Belanoff, JK. Theefficacy of mifepristone in the reduction and prevention of olanzapine-induced weight gain in rats. Behav Brain Res 171: 225–229, 2006.
7. Behnke, AR, Feen, BG, and Welham, WC. The specific gravity ofhealthy men. Body weight/volume as an index of obesity. JAMA118: 495–497, 1942.
8. Brozek, J and Henschel, A, eds. Techniques for Measuring BodyComposition. Washington, DC: National Academy of Sciences, 1961.
9. Brozek, J, Wells, S, and Keys, A. Medical aspects of semistarvation inLeningrad (Siege 1941–1942). Am Rev Sov Med 4: 70–86, 1946.
10. Buskirk, ER, Thompson, RH, and Whedon, GD. Metabolicresponse to cold air in men and women in relation to total body fatcontent. J Appl Physiol 18: 603–612, 1963.
11. Carney, RM and Goldberg, AP. Weight gain after cessation ofcigarette smoking. A possible role for adipose-tissue lipoproteinlipase. N Engl J Med 310: 614–616, 1984.
12. Chen, H, Zhang, SM, Schwarzschild, MA, Hernan, MA, andAscherio, A. Physical activity and the risk of Parkinson disease.Neurology 64: 664–669, 2005.
13. Chumlea, WC, Guo, SS, Kuczmarski, RJ, Flegal, KM, Johnson, CL,Heymsfield, SB, Lukaski, HC, Friedl, KE, and Hubbard, VS. Bodycomposition estimates from NHANES III bioelectrical impedancedata. Int J Obes Relat Metab Disord 26: 1596–1609, 2002.
14. Cureton, KJ. Effects of experimental alterations in excess weight onphysiological responses to exercise and physical performance. In:Body Composition and Physical Performance: Applications for theMilitary Services. Marriott, BM and Grumstrup-Scott, J, eds.Washington, DC: National Academy Press, 1992. pp. 71–88.
15. Davenport, CB and Love, AG. The Medical Department of the UnitedStates Army in the World War (Vol. 15). Statistics; Part 1, ArmyAnthropology. Washington, DC: U.S. Government Printing Office, 1921.
16. Despres, JP, Bouchard, C, Tremblay, A, Savard, R, andMarcotte, M. Effects of aerobic training on fat distribution in malesubjects. Med Sci Sports Exerc 17: 113–118, 1985.
17. Despres, JP, Pouliot, MC, Moorjani, S, Nadeau, A, Tremblay, A,Lupien, PJ, Theriault, G, and Bouchard, C. Loss of abdominal fatand metabolic response to exercise training in obese women. Am JPhysiol 261: E159–E167, 1991.
18. Durnin, JVGA and Womersely, J. Body fat assessed from total bodydensity and its estimation from skinfold thickness: Measurements on481 men and women aged 16 to 72 years. Br J Nutr 32: 77–97, 1974.
19. Ershow, AG, Friedl, KE, Peterson, CM, Riley, WT, Rizzo, AS, andWansink, B. Symposium: Virtual reality technologies for researchand education in obesity and diabetesdSponsored by the NationalInstitutes of Health and Department of Defense. J Diabetes SciTechnol 5: 212–344, 2011.
Journal of Strength and Conditioning Researchthe TM
| www.nsca.com
VOLUME 26 | SUPPLEMENT 7 | JULY 2012 | S97
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
20. Ershow, AG, Ortega, A, Baldwin, JT, and Hill, JO. Engineeringapproaches to energy balance and obesity: Opportunities for novelcollaborations and researchdReport of a Joint National ScienceFoundation and National Institutes of Health Workshop. J DiabetesSci Technol 1: 96–105, 2007.
21. Evans, DJ, Hoffmann, RG, Kalkhoff, RK, and Kissebah, AH.Relationship of androgenic activity to body fat topography, fat cellmorphology, and metabolic aberrations in premenopausal women.J Clin Endocrinol Metab 57: 304–310, 1983.
22. Evans, RK, Negus, C, Antczak, AJ, Yanovich, R, Israeli, E, andMoran, DS. Sex differences in parameters of bone strength in newrecruits: Beyond bone density. Med Sci Sports Exerc 40: S645–S653,2008.
23. Fitzgerald, PI, Vogel, JA, Daniels, WL, Dziados, JE, Teves, MA,Mello, RP, and Reich, PJ. The Body Composition Project: A SummaryReport and Descriptive Data. Technical Report No. T5–87. Natick, MA:U.S. Army Research Institute of Environmental Medicine, 1987.
24. Fleck, SJ. Body composition of elite American athletes. Am J SportsMed 11: 393–403, 1983.
25. Ford, ES, Mokdad, AH, and Giles, WH. Trends in waistcircumference among U.S. adults. Obes Res 11: 1223–1231, 2003.
26. Friedl, KE. Body composition and military performance: Origins ofthe army standards. In: Body Composition and Physical Performance:Applications for the Military Services. B.M. Marriott andJ. Grumstrup-Scott, eds. Washington, DC: National AcademyPress, 1992. pp. 31–55.
27. Friedl, KE. Military application of body composition assessmenttechnologies. In: Emerging Technologies for Nutrition Research:Potential for Assessing Military Performance Capability. S. Carlson-Newberry and R. Costello, eds. Washington, DC: NationalAcademy Press, 1997. pp. 81–126.
28. Friedl, KE. Can you be large and not obese? The distinctionbetween body weight, body fat, and abdominal fat in occupationalstandards. Diab Technol Ther 6: 732–749, 2004.
29. Friedl, KE. Biomedical research on health and performance ofmilitary women: Accomplishments of the 1994 Defense Women’sHealth Research Program (DWHRP). J Women’s Health 14: 764–802, 2005.
30. Friedl, KE. Overview of the HFM-181 symposium programme:Medical technology repurposed to enhance human performance.In:Workshop on Human Performance Enhancement for NATO MilitaryOperations (Science, Technology, and Ethics). Technical Report RTO-HFM/WS-181. Neuilly-sur-Seine Cedex, France: Research andTechnological Organization, North Atlantic Treaty Organization,2009. pp. 1.1–1.20.
31. Friedl, KE. Waist circumference threshold values for type 2diabetes risk. J Diabetes Sci Technol 3: 761–769, 2009.
32. Friedl, KE, DeLuca, JP, Marchitelli, LJ, and Vogel, JA. Reliability ofbody-fat estimations from a four-compartment model usingdensity, body water, and bone mineral measurements. Am J ClinNutr 55: 764–770, 1992.
33. Friedl, KE, DeWinne, CM, and Taylor, RL. The use of the Durnin-Womersley generalized equations for body fat estimation and theirimpact on the Army Weight Control Program. Mil Med 152: 150–155, 1987.
34. Friedl, KE, Marchitelli, LJ, Sherman, DE, and Tulley, R. Nutritionalassessment of cadets at the U.S. Military Academy: Part 1.Anthropometric and Biochemical Measures. Technical Report No.T4–91, November 1990. Natick, MA: US Army Res Institute ofEnvironmental Medicine, 45 pp. AD-A231918, 1991.
35. Friedl, KE, Moore, RJ, Hoyt, RW, Marchitelli, LJ,Martiniez-Lopez, LE, and Askew, EW. Endocrine markers ofsemistarvation in healthy lean men in a multistressor environment.J Appl Physiol 88: 1820–1830, 2000.
36. Friedl, KE, Moore, RJ, Martinez-Lopez, LE, Vogel, JA, Askew, EW,Marchitelli, LJ, Hoyt, R, and Gordon, CC. Lower limits of body fatin healthy active men. J Appl Physiol 77: 933–940, 1994.
37. Friedl, KE and Vogel, JA. Validity of percent body fat predicted bycircumferences: Classification of men for weight controlregulations. Mil Med 162: 194–200, 1997.
38. Friedl, KE, Vogel, JA, Bovee, MW, and Jones, BH. Assessment ofBody Weight Standards in Male and Female Army Recruits. TechnicalReport T15–90. Natick, MA: US Army Research Institute ofEnvironmental Medicine, 1990.
39. Friedl, KE, Westphal, KA, Marchitelli, LJ, Patton, JF,Chumlea, WC, and Guo, S. Evaluation of changes in bodycomposition in young women after a physical training program.Am J Clin Nutr 73: 268–275, 2001.
40. Garn, SM. Fat patterning and fat intercorrelations in the adultmale. Hum Biol 26: 59–69, 1954.
41. Garn, SM. Comparison of pinch-caliper and x-ray measurementsof skin plus subcutaneous fat. Science 124: 178–179, 1956.
42. Garn, SM. Fat weight and fat placement in the female. Science 125:1091–1092, 1957.
43. General Accounting Office. Improved Guidance and Oversight areNeeded to Ensure Validity and Equity of fitness standards. GAO/NSAID-99–9, October 1998.
44. Girth and death. Stat Bull Metropolitan Life Insurance Co 18: 2–5,1937.
45. Glass, JM, Lyden, AK, Petzke, F, Stein, P, Whalen, G, Ambrose, K,Chrousos, G, and Clauw, DJ. The effect of brief exercise cessationon pain, fatigue, and mood symptom development in healthy, fitindividuals. J Psychosom Res 57: 391–398, 2004.
46. Gordon, CC and Friedl, KE. Anthropometry in the U.S. ArmedForces. In: Anthropometry: The Individual and the Population.S.J. Ulijaszek and C.G.N. Mascie-Taylor, eds. Cambridge, MA:Cambridge University Press, 1994. pp. 178–210.
47. Gould, BA. Investigations in the Military and Anthropological Statisticsof American Soldiers. New York, NY: H.O. Houghton and Co, 1869.
48. Hakkinen, A, Rinne, M, Vasankari, T, Santtila, M, Hakkinen, K, andKyrolainen, H. Association of physical fitness with health-relatedquality of life in Finnish young men. Health Qual Life Outcomes 8:1–8, 2010.
49. Hall, KD. Computational model of in vivo human energymetabolism during semistarvation and refeeding. Am J PhysiolEndocrinol Metab 291: E23–E37, 2006.
50. Han, TS, Richmond, P, Avenell, A, and Lean, MEJ. Waistcircumference reduction and cardiovascular benefits duringweight loss in women. Int J Obes Relat Metab Disorder 21:127–134, 1997.
51. Harman, EA and Frykman, PN. The relationship of body size andcomposition to the performance of physically demandingmilitary tasks. In: Body Composition and Physical Performance:Applications for the Military Services. B.M. Marriott andJ. Grumstrup-Scott, eds. Washington, DC: National AcademyPress, 1992. pp. 105–118.
52. Heymsfield, SB, Waki, M, Kehayias, J, Lichtman, S, Dilmanian, FA,Kamen, Y, Wang, J, and Pierson, RN. Chemical and elementalanalysis of humans in vivo using improved body compositionmodels. Am J Physiol 261: E190–E198, 1991.
53. Hodgdon, JA and Beckett, MB. Prediction of Percent Body Fat for USNavy Men from Body Circumferences and Height. Report No. 84-11.San Diego, CA: Naval Health Research Center, 1984.
54. Hodgdon, JA and Beckett, MB. Prediction of Percent Body Fat for USNavy Women from Body Circumferences and Height. Report No. 84-29.San Diego, CA: Naval Health Research Center, 1984.
55. Hodgdon, JA and Fitzgerald, PI. Validity of impedance predictionsat various levels of fatness. Hum Biol 59: 281–298, 1987.
Military Body Fat Standards
S98 Journal of Strength and Conditioning Researchthe TM
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
56. Hodgdon, JA, Fitzgerald, PI, and Vogel, JA. Relationships BetweenBody Fat and Appearance Ratings of U.S. Soldiers. TechnicalReport No. T12–90. US Army Research Institute of EnvironmentalMedicine, Natick, MA and Naval Health Research Center, SanDiego, CA, 1990.
57. Hodgdon, JA and Friedl, KE. Development of the DoD BodyComposition Estimation Equations. Technical Document 99–2B. SanDiego, CA: Naval Health Research Center, 1999.
58. Hong, SK. Pattern of cold adaptation in women divers of Korea(ama). Fed Proc 32: 1614–1622, 1973.
59. Hoyt, RW, Opstad, PK, Haugen, AH, Delany, JP, Cymerman, A,and Friedl, KE. Negative energy balance in male and femalerangers: Effects of 7 days of sustained exercise and fooddeprivation. Am J Clin Nutr 83: 1068–1075, 2006.
60. Hult, M, Tornhammar, P, Ueda, P, Chima, C, Bonamy, AK,Ozumba, B, and Norman, M. Hypertension, diabetes andoverweight: Looming legacies of the Biafran famine. PLoS One 5:313582, 2010.
61. Jacobson, IG, Smith, TC, Smith, B, Keel, PK, Amoroso, PJ, Wells, TS,Bathalon, GP, Boyko, EJ, and Ryan, MAK. Disordered eating andweight changes after deployment: Longitudinal assessment of a largeUS military cohort. Am J Epidemiol 169: 415–427, 2009.
62. Janssen, I, Katzmarzyk, PT, and Ross, R. Waist circumference andnot body mass index explains obesity-related health risk. Am J ClinNutr 79: 379–384, 2004.
63. Keys, A, Brozek, J, Henschel, A, Mickelsen, O, and Taylor, HL. TheBiology of Human Starvation. Vols. 1 and 2. Minneapolis, MN:University of Minnesota Press, 1950.
64. King, MA and Katch, FI. Changes in body density, fatfolds andgirths at 2.3 kg increments of weight loss. Hum Biol 58: 709–718,1986.
65. Kivipelto, M, Ngandu, T, Fratiglioni, L, Viitanen, M, Kareholt, I,Winblad, B, Helkala, EL, Tuomilehto, J, Soininen, H, andNissinen, A. Obesity and vascular risk factors at midlife and the riskof dementia and Alzheimer disease. Arch Neurol 62: 1556–1560, 2005.
66. Knapik, JJ, Jones, SB, Darakjy, S, Hauret, KG, Bullock, SH,Sharp, MA, and Jones, BH. Injury rates and injury risk factors amongU.S. Army wheel vehicle mechanics. Mil Med 172: 988–996, 2007.
67. Knapik, JJ and Sharp, MA. Task-specific and generalized physicaltraining for improving manual-material handling capability. Int JIndustrial Ergonomics 22: 149–160, 1998.
68. Krotkiewski, M and Bjorntorp, P. Muscle tissue in obesity withdifferent distribution of adipose tissue. Effects of physical training.Int J Obes 10: 331–341, 1986.
69. Krotkiewski, M, Bjorntorp, P, Sjostrom, L, and Smith, U. Impactof obesity on metabolism in men and women. Importance ofregional adipose tissue distribution. J Clin Invest 72: 1150–1162, 1983.
70. Krzywicki, HJ and Chinn, KSK. Body composition of a militarypopulation, Fort Carson, 1963. Am J Clin Nutr 20: 708–715, 1967.
71. Kujawa, KI, Loan, MV, Conway, JM, Stewart, WL, andHodgdon, JA. Validity of Navy circumference body fat equation inwomen of African-American, Asian, Hispanic and Filipina descent.Med Sci Sports Exerc 34: S238, 2002.
72. Kvist, H, Chowdhury, B, Grangard, U, Tylen, U, and Sjostrom, L.Total and visceral adipose-tissue volumes derived frommeasurements with computed tomography in adult men andwomen: Predictive equations. Am J Clin Nutr 48: 1351–1361, 1988.
73. Lemieux, S, Prud’homme, D, Bouchard, C, Tremblay, A, andDespres, JP. Sex differences in the relation of visceral adipose tissueaccumulation to total body fatness. Am J Clin Nutr 58: 463–467, 1993.
74. Leu, JR and Friedl, KE. Body fat standards and individual physicalreadiness in a randomized Army sample: Screening weights,methods of fat assessment, and linkage to physical fitness. Mil Med167: 994–1000, 2002.
75. Leyk, D, Ruther, T, Wunderlich, M, Sievert, A, Essfeld, D, Witzki, A,Erley, O, Kuchmeister, G, Piekarski, C, and Lollgen, H. Physicalperformance in middle age and old age: Good news for oursedentary and aging society. Dtsch Arztebl Int 107: 809–816, 2010.
76. Love, AG and Davenport, CB. Physical Examination of the FirstMillion Draft Recruits: Methods and Results. Bulletin No. 11. U.S.Army Medical Department. Washington, DC: GovernmentPrinting Office, 1919. p. 17.
77. Matsuzawa, Y, Fujioka, S, Tokunaga, K, and Tarui, S. Classificationof obesity with respect to morbidity. Proc Soc Exp Biol Med 200:197–201, 1992.
78. Marin, P, Holmang, S, Jonsson, L, Sjostrom, L, Kvist, H, Holm, G,Lindstedt, G, and Bjorntorp, P. The effects of testosteronetreatment on body composition and metabolism in middle-agedobese men. Int J Obes 16: 991–997, 1992.
79. Marin, P, Oden, B, and Bjorntorp, P. Assimilation and mobilizationof triglycerides in subcutaneous abdominal and femoral adiposetissue in vivo in men: Effects of androgens. J Clin Endocrinol Metab80: 239–243, 1995.
80. McNulty, PA. Prevalence and contributing factors of eatingdisorder behaviors in a population of female Navy nurses. Mil Med162: 703–706, 1997.
81. McNulty, PA. Prevalence and contributing factors of eatingdisorder behaviors in active duty service women in the Army,Navy, Air Force, and Marines. Mil Med 166: 53–58, 2001.
82. Miller, KD, Jones, E, Yanovski, JA, Shankar, R, Feuerstein, I, andFalloon, J. Visceral abdominal fat accumulation associated with useof indinavir. Lancet 351: 871–875, 1998.
83. Murlin, JR. Some problems of nutrition in the Army. Science 47:495–508, 1918.
84. Murlin, JR and Hildebrandt, FM. Average food consumption in thetraining camps of the United States Army. Am J Physiol 49: 531–556, 1919.
85. Newton, RL Jr, Han, H, Stewart, TM, Ryan, DH, andWilliamson, DA.Efficacy of a pilot internet-based weight management program(H.E.A.L.T.H.) and longitudinal physical fitness data in Army Reservesoldiers. J Diabetes Sci Technol 5: 1255–1262, 2011.
86. Niebuhr, DW, Scott, CT, Li, Y, Bedno, SA, Han, W, andPowers, TE. Preaccession fitness and body composition as predictorsof attrition in U.S. Army recruits. Mil Med 174: 695–701, 2009.
87. Ogden, CL, Carroll, MD, Kit, BK, and Flegal, KM. Prevalenceof obesity and trends in body mass index among us childrenand adolescents, 1999–2010. JAMA doi:10.1001/jama.2012.40, 2012.
88. Onishi, N. Japan, seeking trim waists, measures millions. New YorkTimes June 13, 2008. Available at: http://www.nytimes.com/2008/06/13/world/asia/13fat.html. Accessed June 2, 2012.
89. Pace, N and Rathbun, EN. Studies on body composition. III. Thebody water and chemically combined nitrogen content in relationto fat content. J Biol Chem 158: 685–691, 1945.
90. Paris, RM, Bedno, SA, Krauss, MR, Keep, LW, and Rubertone, MV.Weighing in on type 2 diabetes in the military. Diabetes Care 24:1894–1898, 2001.
91. Pingting, X. China relaxes tattoo, weight rules for army recruits. ChinaDaily 2, 2011. Available at: http://www.chinadaily.com.cn/usa/china/2011-11/02/content_14023791.htm. Accessed June 2, 2012.
92. Prisby, R, Glickman-Weiss, EL, Nelson, AG, and Caine, N.Thermal and metabolic responses of high and low fat women tocold water immersion. Aviat Space Environ Med 70: 887–891, 1999.
93. Ravelli, GP, Stein, ZA, and Susser, MW. Obesity in young menafter famine exposure in utero and early infancy. N Engl J Med 295:349–353, 1976.
94. Rebuffe-Scrive, M, Enk, L, Crona, N, Lonnroth, P,Abrahamsson, L, Smith, U, and Bjorntorp, P. Regional humanadipose tissue metabolism during the menstrual cycle, pregnancy,and lactation. J Clin Invest 75: 1973–1976, 1985.
Journal of Strength and Conditioning Researchthe TM
| www.nsca.com
VOLUME 26 | SUPPLEMENT 7 | JULY 2012 | S99
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
95. Reed, LJ and Love, AG. Biometric studies on US Army officers:Somatological norms, correlations, and changes with age. Hum Biol4: 509–524, 1932.
96. Rose, MS, Moore, R, Mahnke, E, Christensen, E, and Askew, EW.Weight Reduction Techniques Adopted When Weight Standards areEnforced. Technical Report No. T4-93. Natick, MA: Army ResearchInstitute of Environmental Medicine, 2002.
97. Ross, R and Rissanen, J. Mobilization of visceral and subcutaneousadipose tissue in response to energy restriction and exercise. Am JClin Nutr 60: 695–703, 1994.
98. Santtila, M, Hakkinen, K, Karavirta, L, and Kyrolainen, H. Changesin cardiovascular performance during an 8-week military basictraining period combined with added endurance or strengthtraining. Mil Med 173: 1173–1179, 2008.
99. Santtila, M, Kyrolainen, H, Vasankari, T, Tiainen, S, Palvalin, K, andHakkinen, A. Physical fitness profiles in young Finnish men duringthe years 1975–2004. Med Sci Sports Exerc 38: 1990–1994, 2006.
100. Seeman, TE, McEwen, BS, Rowe, JW, and Singer, BH. Allostaticload as a marker of cumulative biological risk: MacArthur studies ofsuccessful aging. Proc Natl Acad Sci U S A 98: 4770–4775, 2001.
101. Segal, KR, Van Loan, M, Fitzgerald, PI, Hodgdon, JA, and VanItallie, TB. Lean body mass estimation by bioelectrical impedanceanalysis: A four-site cross-validation study. Am J Clin Nutr 47:7–14, 1988.
102. Seidell, JC, Cigolini, M, Charzewska, J, Ellsinger, BM, DiBiase, G,Bjorntrop, P, Hautvast, JGAJ, Contaldo, F, Szostak, V, andScuro, LA. Androgenicity in relation to body fat distribution andmetabolism in 38-year-old womendThe European fat distributionstudy. J Clin Epidemiol 43: 21–34, 1990.
103. Seidell, JC, Kahn, HS, Williamson, DF, Lissner, L, and Valdez, R.Report from a Centers for Disease Control and Preventionworkshop on use of adult anthropometry for public health andprimary health care. Am J Clin Nutr 73: 123–126, 2001.
104. Sharp, MA, Nindl, BC, Westphal, KA, and Friedl, KE. The physicalperformance of woman Army basic trainees who pass and fail theArmy body weight and %BF standards. In: Advances in IndustrialErgonomics and Safety VI. Agedzadeh, E, ed. Washington, DC:Taylor and Francis, 1994. pp. 743–750.
105. Sharp, MA, Patton, JF, Knapik, JJ, Hauret, K, Mello, RP, Ito, M, andFrykman, PN. Comparison of the physical fitness of men andwomen entering the U.S. Army: 1978–1998. Med Sci Sports Exerc34: 356–363, 2002.
106. Shimoka, H, Muller, DC, and Andres, R. Studies in the distribution ofbody fat. III. Effects of cigarette smoking. JAMA 261: 1169–1173, 1989.
107. Spurr, GB. Physical work performance under conditions ofprolonged hypocaloria. In: Predicting Decrements in MilitaryPerformance Due to Inadequate Nutrition. Washington, DC: NationalAcademy Press, 1986. pp. 99–135.
108. Stewart, T, Han, H, Allen, RH, Bathalon, G, Ryan, DH,Newton, RL Jr, and Williamson, DA. H.E.A.L.T.H.: Efficacy of aninternet/population-based behavioral weight managementprogram for the U.S. Army. J Diabetes Sci Technol 5: 178–187, 2011.
109. Stewart, T, May, S, Allen, HR, Bathalon, GP, Lavergne, G,Sigrist, L, Ryan, D, and Williamson, DA. Development of aninternet/population-based weight management Program for the U.S. Army. J Diabetes Sci Technol 2: 116–126, 2008.
110. Taylor, MK, Hodgdon, JA, Griswold, L, Miller, A, Roberts, DE, andEscamilla, RF. Cervical resistance training: Effects on isometric anddynamic strength. Aviat Space Environ Med 77: 1131–1135, 2006.
111. Tarnopolsky, LJ, MacDougall, JD, Atkinson, SA, Tarnopolsky, MA,and Sutton, JR. Gender differences in substrate for enduranceexercise. J Appl Physiol 68: 302–308, 1990.
112. Tarnopolsky, MA. Sex difference in exercise metabolism and therole of 17-beta estradiol. Med Sci Sports Exerc 40: 648–654, 2008.
113. Teves, MA, Wright, JE, and Vogel, A. Performance on SelectedCandidate Screening Test Procedures Before and After Army Basic and
Advanced Individual Training. Technical Report T13/85. Natick, MA:USARIEM, 1985. ADA162805.
114. US Department of Defense, Office of the Assistant Secretary ofDefense for Manpower, Reserve Affairs and Logistics. Study of theMilitary Services Physical Fitness. Washington, DC. April 3, 1981.
115. US Department of Defense; Joint Technical Coordinating Group 5(Military Operational Medicine Research Program). SummaryReport. Research Workshop on Physical Fitness Standards andMeasurements Within the Military Services. August 31 toSeptember 2, 1999. Washington, DC. 20 pp. Available at: http://www.momrp.org/publications/PhysFitStds_Bklt_Web.pdf.Accessed June 2, 2012.
116. Vague, J. The degree of masculine differentiation of obesities: Afactor determining predisposition to diabetes, atherosclerosis, goutand uric calculous disease. Am J Clin Nutr 4: 20–34, 1956.
117. Van Loan, M, Hodgdon, JA, and Kujawa, K. Body Composition inMilitary or Military Eligible Women. Final Report. Presidio of SanFrancisco, CA: Western Human Nutrition Research Center, 2001.19 pp. AD A400125.
118. Vogel, JA, Crowdy, JP, Amor, AF, and Worsley, DE. Changes inaerobic fitness and body fat during army recruit training. Eur JAppl Physiol 40: 37–43, 1978.
119. Vogel, JA and Friedl, KE. Army data: Body composition andphysical capacity. In: Body Composition and Physical Performance:Applications for the Military Services. Marriott, BM and Grumstrup-Scott, J, eds. Washington, DC: National Academy Press, 1992. pp.89–103.
120. Vogel, JA and Friedl, KE. Body fat assessment in women: Specialconsiderations. Sports Med 13: 245–269, 1992.
121. Vogel, JA, Wright, JE, Patton, JF III, Dawson, J, andEscherback, MP. A system for establishing occupationally-relatedgender-free physical fitness standards. Technical Report T5/80.Natick, MA: US Army Res Inst Environ Med, 1980. ADA094518.
122. Ward, GM, Krzywicki, HJ, Rahman, DP, Quaas, RL, Nelson, RA,and Consolazio, CF. Relationship of anthropometricmeasurements to body fat as determined by densitometry,potassium-40, and body water. Am J Clin Nutr 28: 162–169, 1975.
123. Welham, WC and Behnke, AR. The specific gravity of healthymen. Body weight divided by volume and other physicalcharacteristics of exceptional athletes and of naval personnel.JAMA 118: 498–501, 1942.
124. Williamson, DA, Bathalon, GP, Sigrist, LD, Allen, HR, Friedl, KE,Young, AJ, Martin, CK, Stewart, TM, Burrell, L, Han, H,Hubbard, VS, and Ryan, D. Military services fitness database:Development of a computerized physical fitness and weightmanagement database for the U.S. army. Mil Med 174: 1–8, 2009.
125. Woodhouse, LJ, Gupta, N, Bhasin, M, Singh, AB, Ross, R,Phillips, J, and Bhasin, S. Dose-dependent effects of testosterone onregional adipose tissue distribution in healthy young men. J ClinEndocrinol Metab 89: 718–726, 2004.
126. Wright, HF, Dotson, CO, and Davis, PO. An investigation ofassessment techniques for body composition of women Marines.US Navy Med 71: 15–26, 1980.
127. Wright, HF, Dotson, CO, and Davis, PO. A simple technique formeasurement of percent body fat in man. US Navy Med 72: 23–27,1981.
128. Wright, HF and Wilmore, JH. Estimation of relative body fat andlean body weight in a United States Marine Corps population.Aerosp Med 45: 301–306, 1974.
129. Xu, X, Castellani, JW, Santee, W, and Kolka, M. Thermal responsesfor men with different fat compositions during immersion in coldwater at two depths: Prediction versus observation. Eur J ApplPhysiol 100: 79–88. 2007.
130. Zwiren, L, Skinner, JS, and Buskirk, ER. Use of body density andvarious skinfold equations for estimating small reductions in bodyfatness. J Sports Med Phys Fitness 13: 213–218, 1973.
Military Body Fat Standards
S100 Journal of Strength and Conditioning Researchthe TM
Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.