Embed Size (px)
Citation preview
Blounts Disease
By Dr Harsimranjeet Singh Sidhu
Chairperson- Dr Rupa Kumar C.S
History
• Erlacher was the first to describe tibia vara and internal tibial torsion- 1922.
• Blount- 1937- His Article prompted the diagnosis of this disorder
• Langenskiold in 1952 came up with classification for this disorder
Dr Blount Description
• “an osteocondrosis similar to Coxa Plana and Madelung deformity but located at the medial side of the proximal tibialepiphysis”
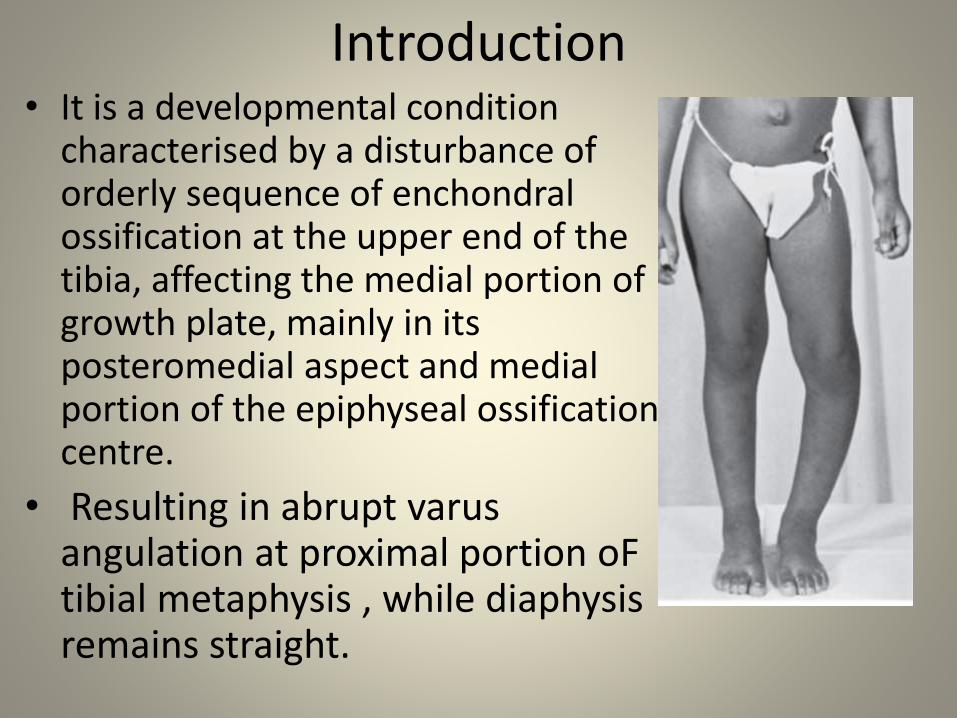
Introduction• It is a developmental condition
characterised by a disturbance of orderly sequence of enchondralossification at the upper end of the tibia, affecting the medial portion of growth plate, mainly in its posteromedial aspect and medial portion of the epiphyseal ossification centre.
• Resulting in abrupt varusangulation at proximal portion oFtibial metaphysis , while diaphysisremains straight.
Etiology- What Causes It.
• Current concept – tibia vara is an acquired disease of proximal tibial metaphysis of unknown cause.
• Enchondral ossification is most likely altered.
Suggested causative factors
• Infection
• Trauma
• Osteonecrosis
• Latent form of rickets
ALTHOUGH NONE HAVE BEEN PROVED
Combination of developmental and hereditary factors is most likely the cause
• The Relationship of early walking and obesity with Blount disease has been clearly documented.
• Rarely seen in non ambulatory children.
ETIOLOGY contd
• Familial occurance reported by several authors…..but as noted by Langenskiold and Riska, because radiographic features of infantile tibia vara have never been seen in patients younger than 1 year and rarely before 2 years..this condition should be consider congenital one.
PATHOLOGYHistologic evaluation of affected growth plates and
corresponding part of metaphysis shows :-
1. Islands of densely packed cartilage cells displaying greater hypertrophy than expected from their position in growth plate.
2. Island of nearly acellular cartilage.
3. exceptionally large clusters of capillary vessels.
Pathophysiology
• The physeal cell collumns become irregular and disordered in arrangement and normal endochondral ossification is disrupted , both in the medial aspect of metaphysis and in corresponding part of physis.
• Varus deformity progresses as long as ossification is defective and growth continues laterally on lateral part of physis.
• In later stages , an actual bony bridge may tether the medial growth , and the medial tibialplateau may apear deficient posteromedialy.
• Ligamentous laxity on lateral side of knee frequently develops in a neglected or recurrent deformity .
Classification
• Blount distinguished it as :-
Infantile-
Less than 8 years of age
bilateral in 60 %
Adolescent :-
more than 8 years to skeletal fusion.
with a cause- black, obese.
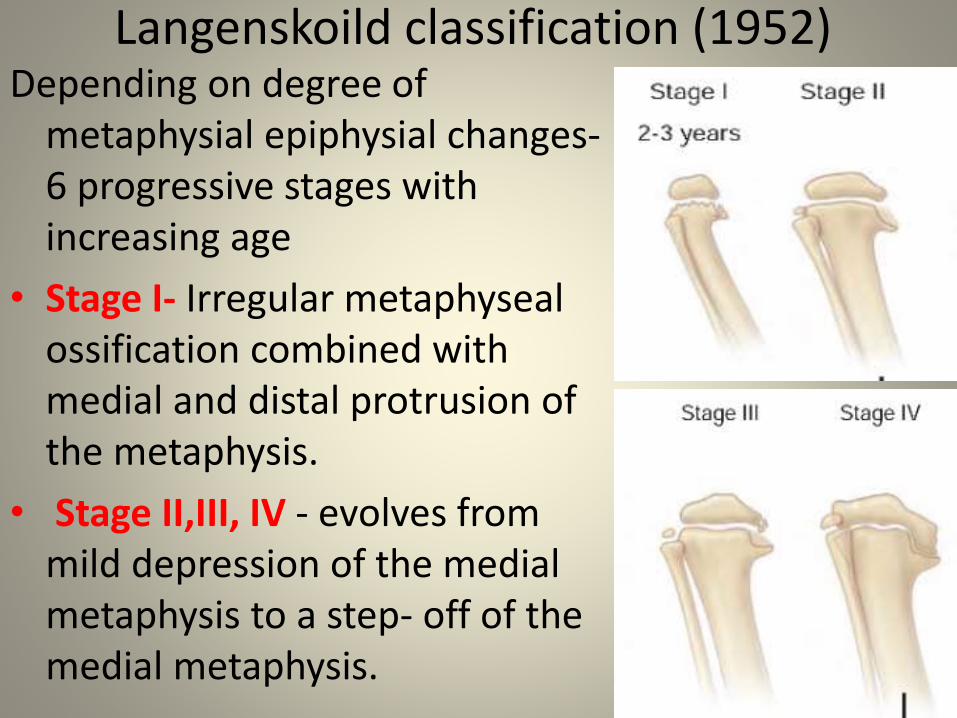
Langenskoild classification (1952)Depending on degree of
metaphysial epiphysial changes-6 progressive stages with increasing age
• Stage I- Irregular metaphysealossification combined with medial and distal protrusion of the metaphysis.
• Stage II,III, IV - evolves from mild depression of the medial metaphysis to a step- off of the medial metaphysis.
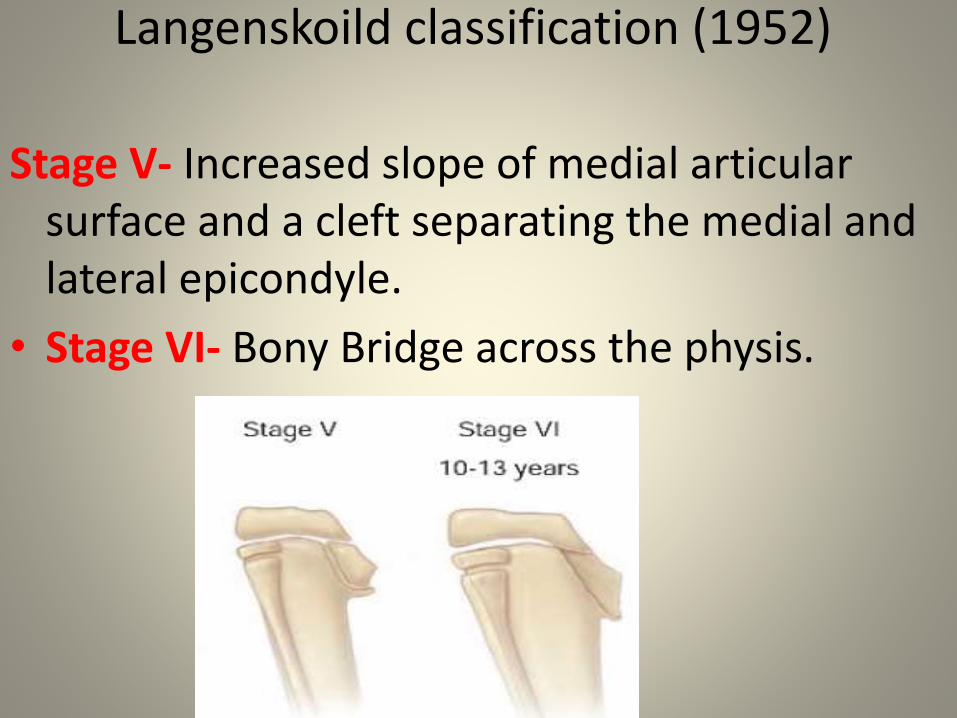
Langenskoild classification (1952)
Stage V- Increased slope of medial articularsurface and a cleft separating the medial and lateral epicondyle.
• Stage VI- Bony Bridge across the physis.
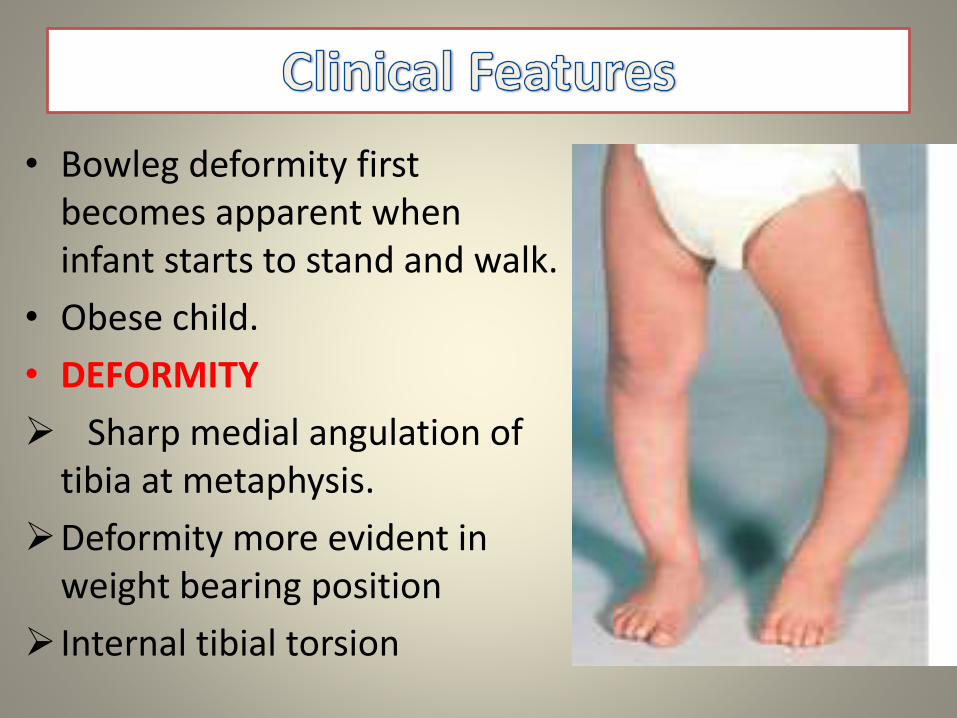
• Bowleg deformity first becomes apparent when infant starts to stand and walk.
• Obese child.
• DEFORMITY
Sharp medial angulation of tibia at metaphysis.
Deformity more evident in weight bearing position
Internal tibial torsion
Clinical Picture
• To compensate for the tibial varus , the medial femoral condyle hypertrophies.
• Over the medial aspect of epiphyseometaphysealjunction , a bony , hard , non tender prominence is palpable( reffered as BEAK on xrays )
• In long standing neglected cases –
slight flexion deformity is added to varus deformity.
collateral ligaments become lax- joint unstable.
medial tibial condyle becomes severely depressed and OA develops within medial compartment of knee.
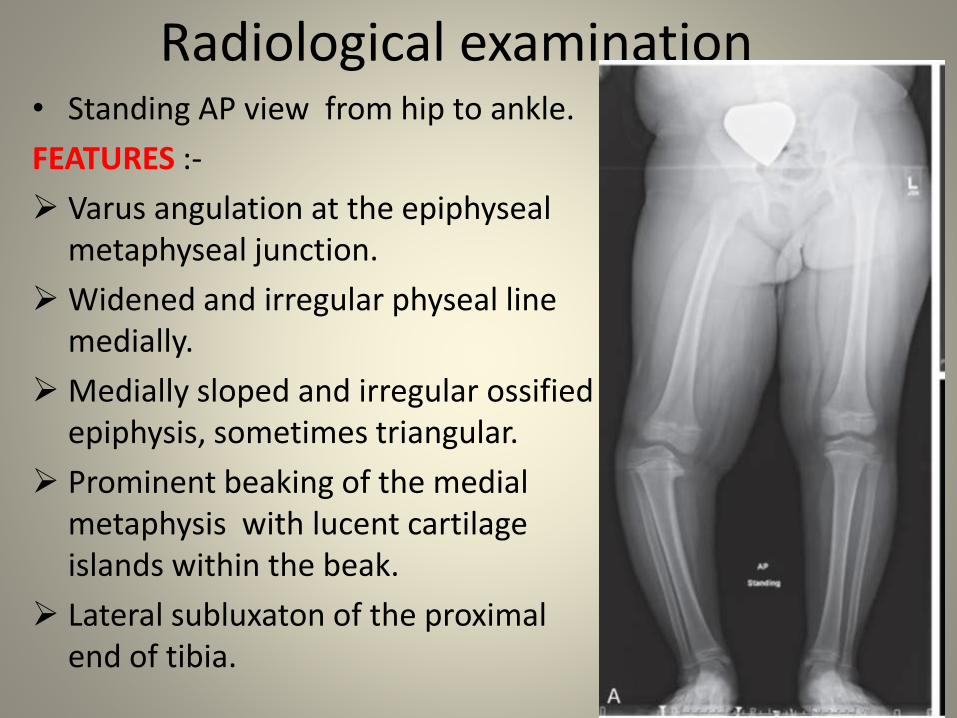
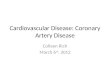
Radiological examination• Standing AP view from hip to ankle.
FEATURES :-
Varus angulation at the epiphysealmetaphyseal junction.
Widened and irregular physeal line medially.
Medially sloped and irregular ossified epiphysis, sometimes triangular.
Prominent beaking of the medial metaphysis with lucent cartilage islands within the beak.
Lateral subluxaton of the proximal end of tibia.
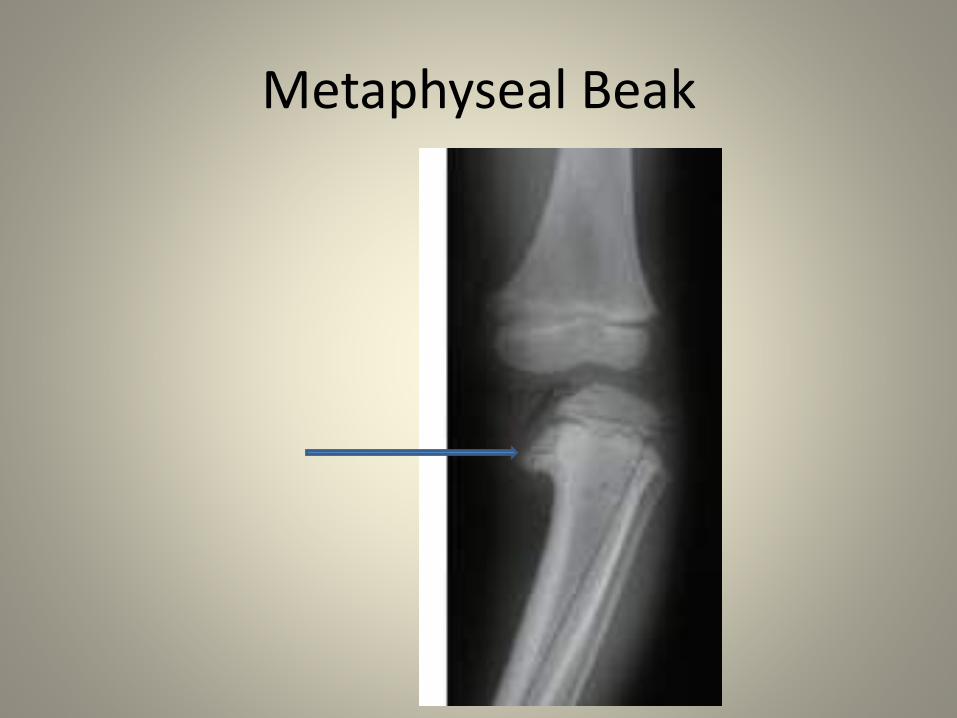
Metaphyseal Beak
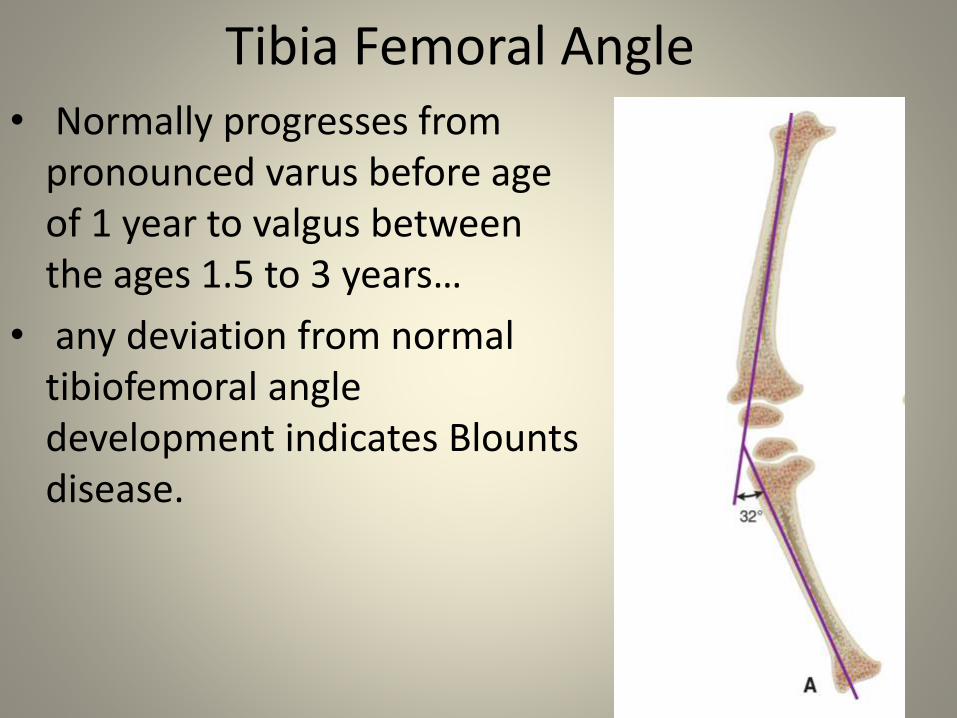
Tibia Femoral Angle• Normally progresses from
pronounced varus before age of 1 year to valgus between the ages 1.5 to 3 years…
• any deviation from normal tibiofemoral angle development indicates Blountsdisease.
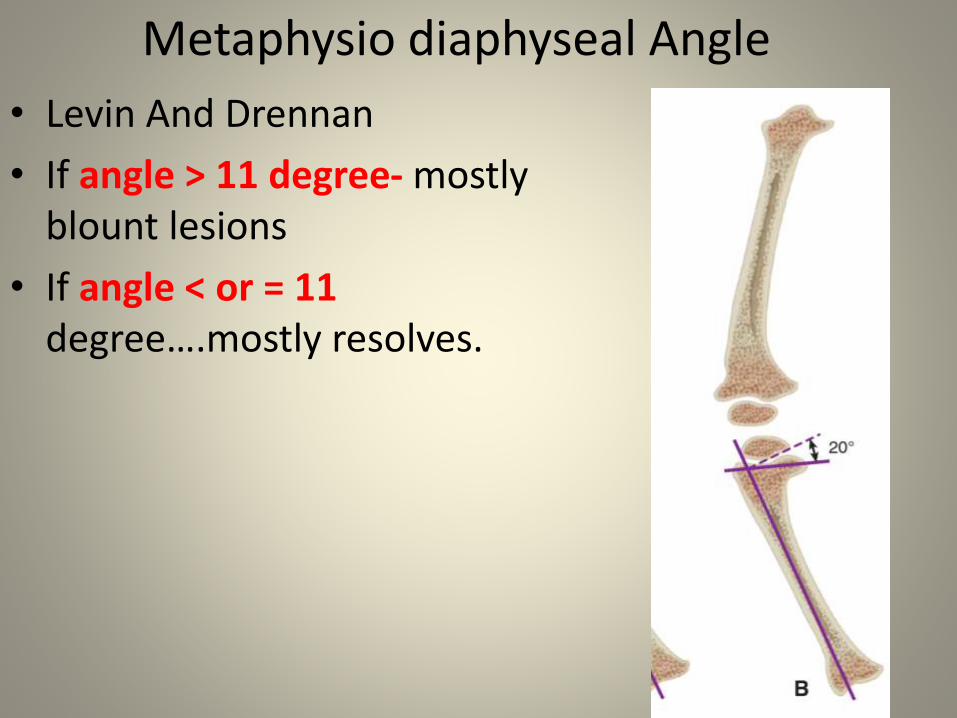
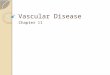
Metaphysio diaphyseal Angle
• Levin And Drennan
• If angle > 11 degree- mostly blount lesions
• If angle < or = 11 degree….mostly resolves.
Further Work Up
• No specific blood markers.
• TESTS to rule out Rickets, ViTamin D deficiency
• Ct scan is indicated to detect physeal bar in children above 5 years of age.
Diffrential Diagnosis
• Physiologic Genu Varum
• Skeletal dysplasias
• Metabolic diseases ( renal osteodystrophy, vit d resistant rickets )
• post traumatic deformity
• Post infective sequelae
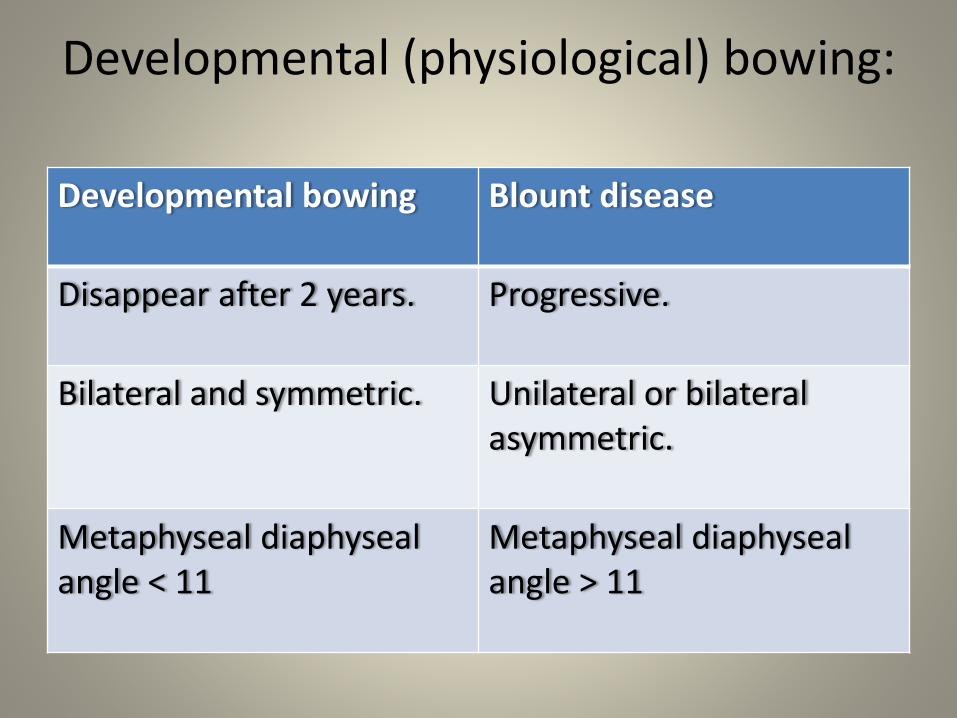
Developmental (physiological) bowing:
Developmental bowing Blount disease
Disappear after 2 years. Progressive.
Bilateral and symmetric. Unilateral or bilateral asymmetric.
Metaphyseal diaphysealangle < 11
Metaphyseal diaphysealangle > 11
TREATMENT
• Treatment choices and prognosis greatly depends upon on the age of the patient and radiographic stage of the disease
ORTHOTICS• INDICATIONS
Child younger than 3 years of age
Lesions not greater than langenskiold stage 1 and 2.
Especially if unilateral involvement.
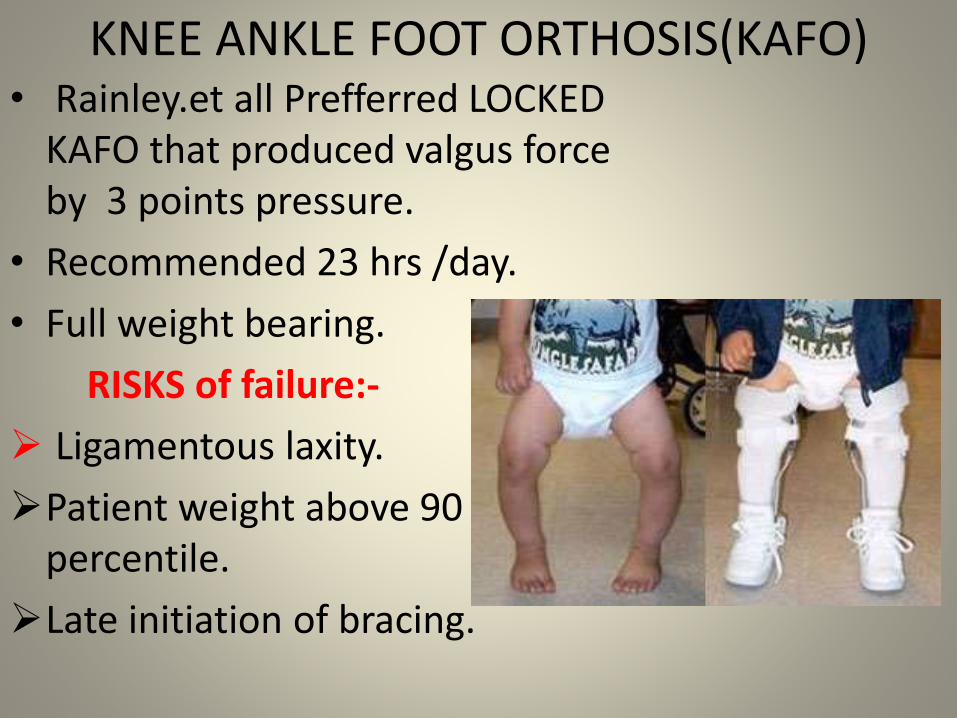
KNEE ANKLE FOOT ORTHOSIS(KAFO)• Rainley.et all Prefferred LOCKED
KAFO that produced valgus force by 3 points pressure.
• Recommended 23 hrs /day.
• Full weight bearing.
RISKS of failure:-
Ligamentous laxity.
Patient weight above 90 percentile.
Late initiation of bracing.
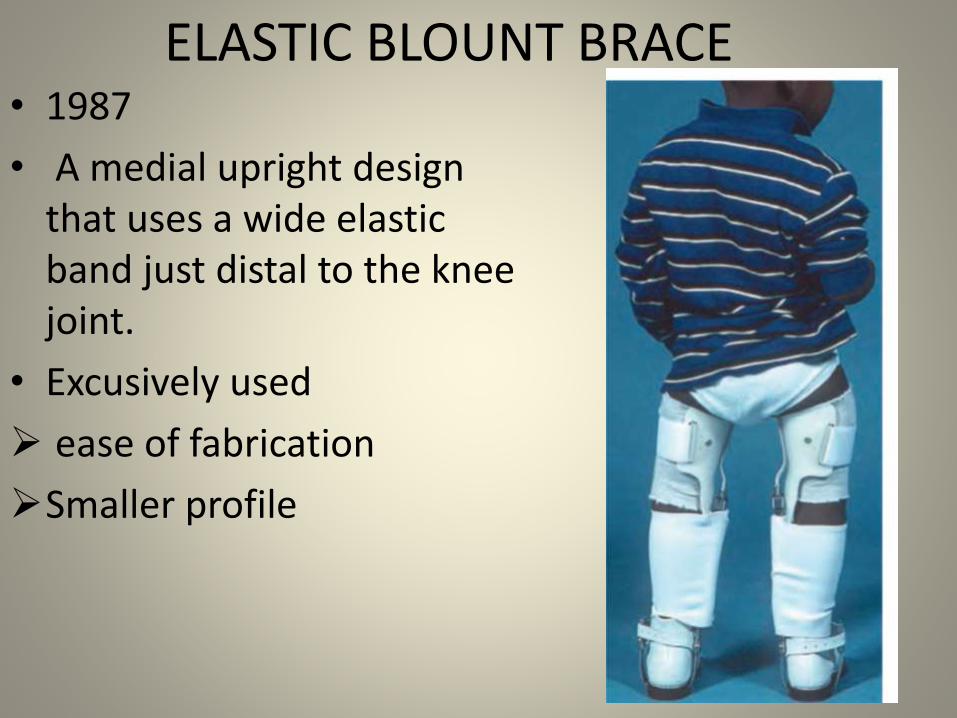
ELASTIC BLOUNT BRACE• 1987
• A medial upright design that uses a wide elastic band just distal to the knee joint.
• Excusively used
ease of fabrication
Smaller profile
Corrective Osteotomy Options
METAPHYSEAL
EPIPHYSEAL- METAPHYSEAL
INTRA EPIPHYSEAL
Rx – CORRECTIVE OSTEOTOMY• In children older than 9 years with more severe
involvement , osteotomy alone , with bony bar resection , or with epiphysiodesis of lateral tibialand fibular physis is indicated.
• For older Children in whom bracing and tibialosteotomy have failed to prevent progressive deformity , Ingram , Siffert and others have suggested an intraepiphyseal osteotomy to correct severe joint instability and a valgus metaphysealosteotomy to correct the varus angulation
CORRECTIVE OSTEOTOMY Rx
• Schoenecker et al- elevation of medial tibialplateau along with metaphyseaal wedge osteotomy
• Gregosiewics – Double elevating osteotomies; intraepiphyseal and metaphyseal.
• Zeyer – hemicondylar tibial osteotomy through the epiphysis into the tibial intercondylar notch.
• Bell, Coogan- Recommended illizarov technique.
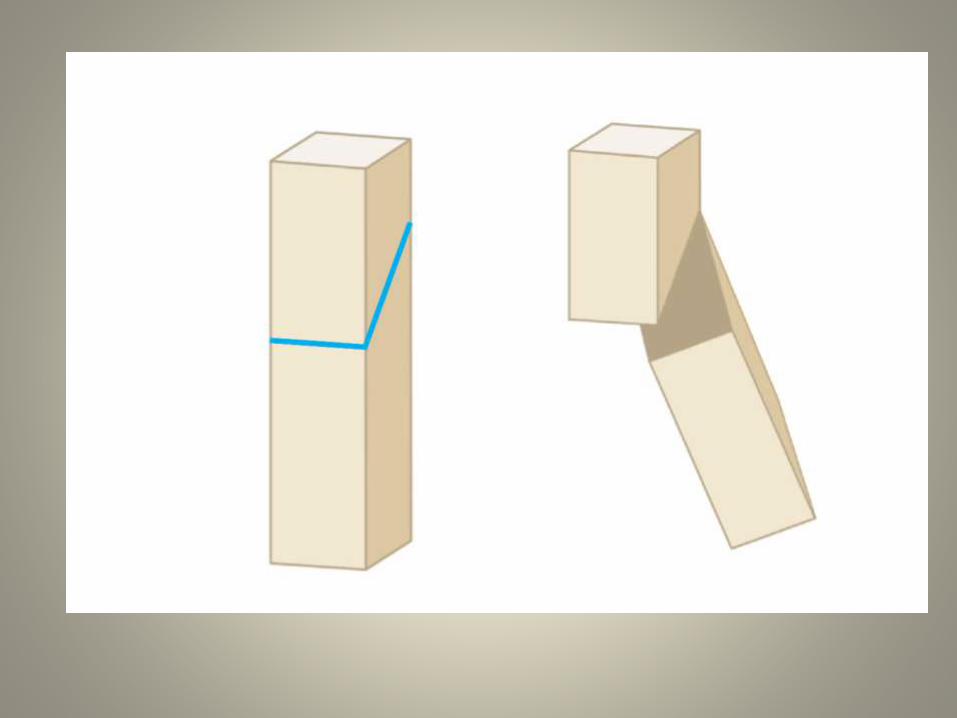
Metaphyseal oblique osteotomy
• George .T.Rab
• Advantage-
• single plane oblique cut allows simultaneous correction of varus and internal rotation .
• permits postoperative cast wedging if necessary to obtain appropriate position.
• Post-operatively
Cast is changed at 4 weeks
Weight bearing allowed if callus evident over radiographs
Cast worn till 8 weeks/ till union is evident radiologically
CHEVERON OSTEOTOMY• GREENE
• MODIFICATION OF DOME OSTEOTOMY
• Advantages
Greater Stability
Mininmal changes in leg length.
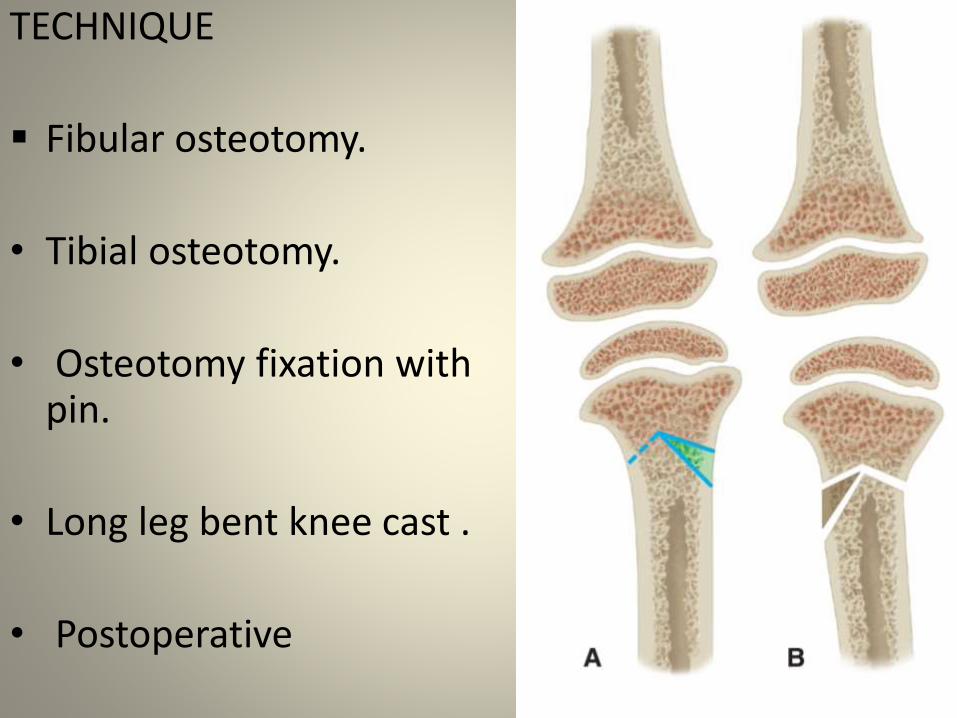
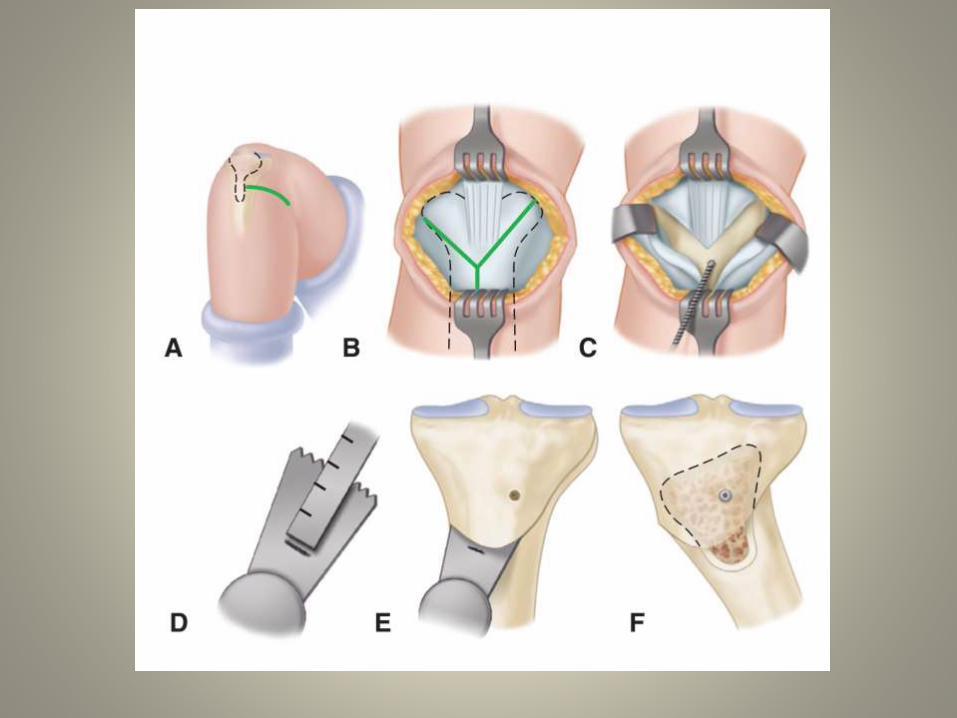
TECHNIQUE
Fibular osteotomy.
• Tibial osteotomy.
• Osteotomy fixation with pin.
• Long leg bent knee cast .
• Postoperative
DISADVANTAGES
Loss of fixation/ correction
longer period of cast immobilisation
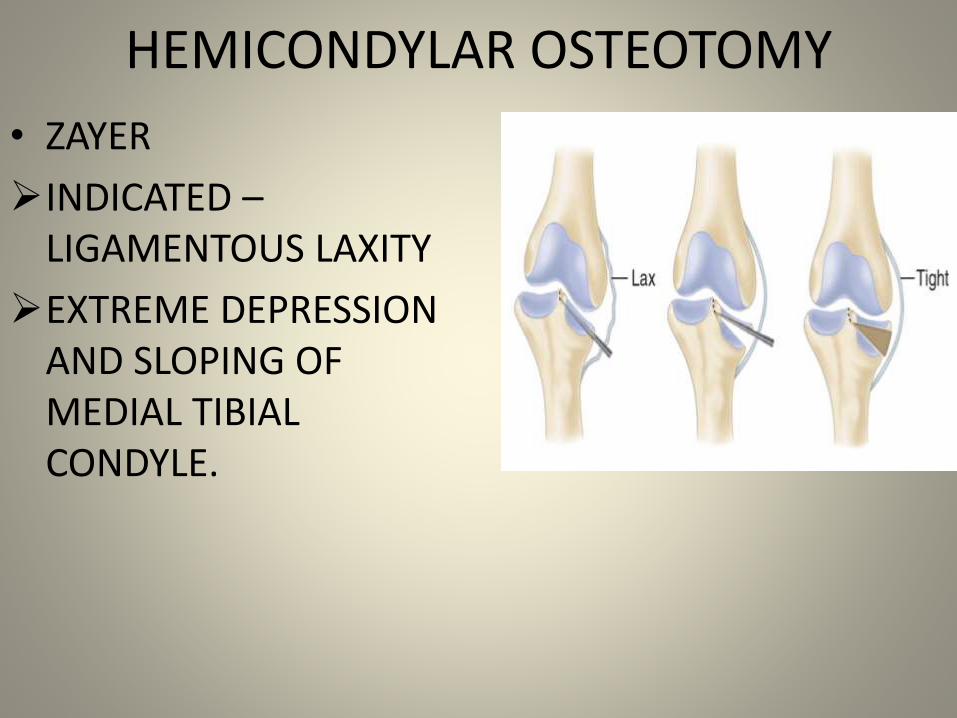
HEMICONDYLAR OSTEOTOMY
• ZAYER
INDICATED –LIGAMENTOUS LAXITY
EXTREME DEPRESSION AND SLOPING OF MEDIAL TIBIAL CONDYLE.
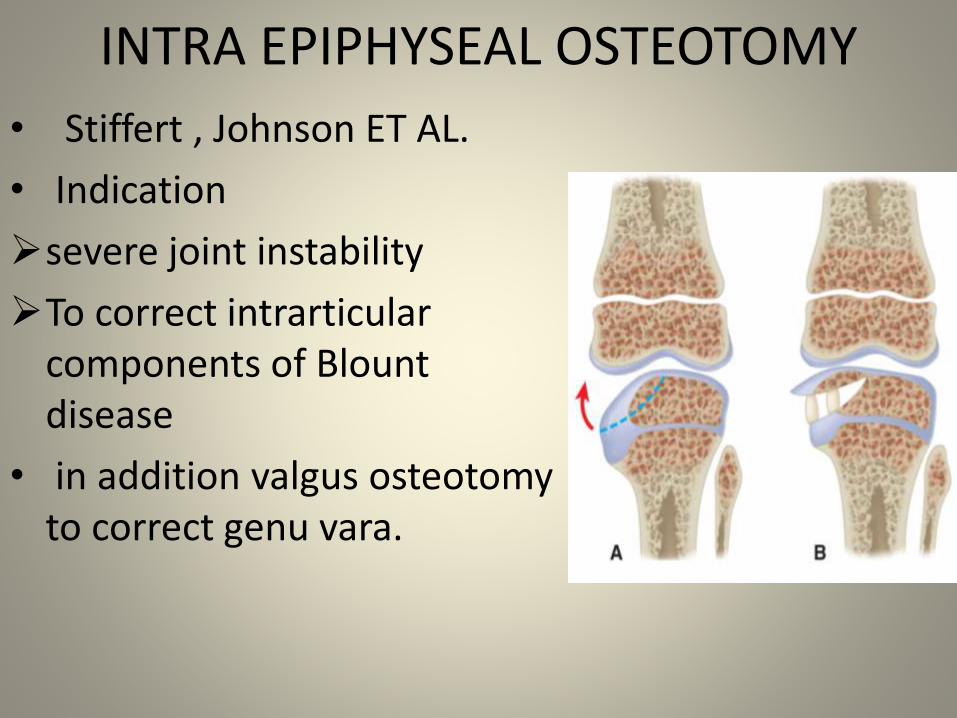
INTRA EPIPHYSEAL OSTEOTOMY
• Stiffert , Johnson ET AL.
• Indication
severe joint instability
To correct intrarticularcomponents of Blount disease
• in addition valgus osteotomyto correct genu vara.
ILIZAROV TECHNIQUE
• Effective in correction of deformity and lengthening if indicated in adolescent patient.
• Allows – adjustment of limb alignment postoperatively.
• Fixation to tibia is achieved by 4 proximal and 4 distal wires that are affixed to rings and tensioned.
COMPLICATIONS
• Common peroneal nerve palsy.
• Compartment Syndrome
• Anterior Tibial Artery Occlusion
• Recurrence
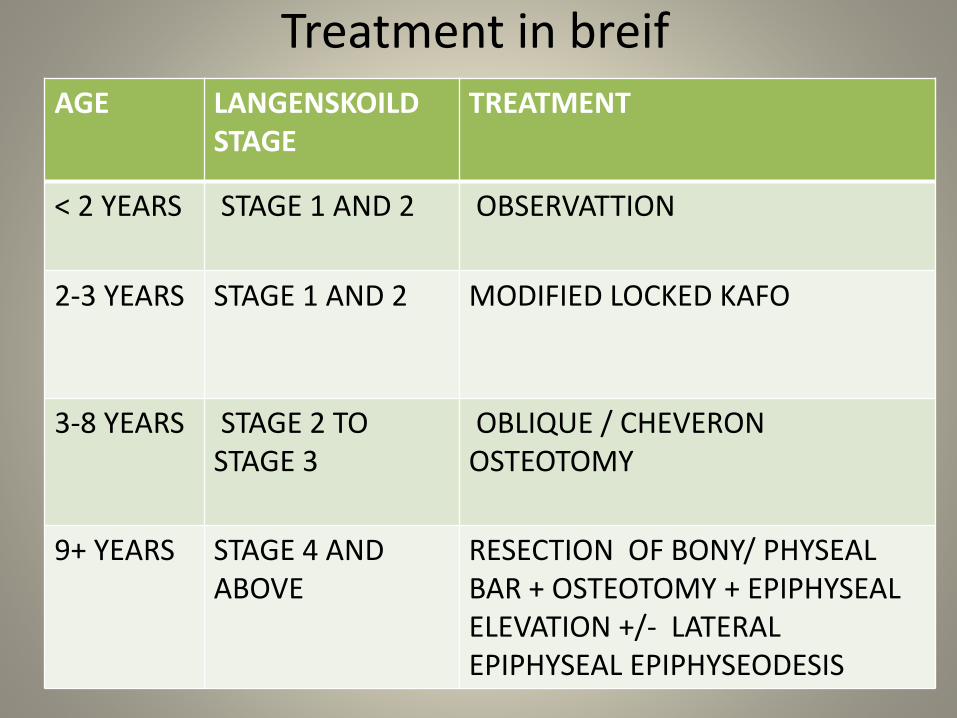
Treatment in breifAGE LANGENSKOILD
STAGETREATMENT
< 2 YEARS STAGE 1 AND 2 OBSERVATTION
2-3 YEARS STAGE 1 AND 2 MODIFIED LOCKED KAFO
3-8 YEARS STAGE 2 TO STAGE 3
OBLIQUE / CHEVERON OSTEOTOMY
9+ YEARS STAGE 4 AND ABOVE
RESECTION OF BONY/ PHYSEAL BAR + OSTEOTOMY + EPIPHYSEAL ELEVATION +/- LATERAL EPIPHYSEAL EPIPHYSEODESIS
REFERENCES
1. Campbells operative orthopaedics volume 2; 12th edition
2. Tachdijian’s pediatric orthopedics volume 2; 4th edition
3. Turek orthopaedic principle and application volume 2 ;4th edition.
THANK YOU!!!!!!!
![Beaufort County Community Collegecircanceast.beaufortccc.edu/BCCC/articles/December 1995... · 2019-02-18 · Mr. Woolard: Hot dog! [Everyone laughed.] A bunch of boys from Blounts](https://img.pdfslide.us/doc/110x75/5f8d07b5253091332f72e55f/beaufort-county-community-1995-2019-02-18-mr-woolard-hot-dog-everyone.jpg)