Embed Size (px)
Citation preview

11/04/2023 1
Bleeding and coagulation disorders in
childrenDr.K.V.Giridhar
Associate Prof. of Pediatrics
GMC. Ananthapuramu, A.P.,India.

Definition:• Spontaneous bleeding.• Excessive & Prollanged bleeding following trauma.
• Petechiae, purpura, echymosis, bruises, hematoma, hemarthrosis, IC bleeds, occult GI bleeds, melena, epistaxis.

Bleeding disorders
Coagulation
disorders

Hemostasis
Tissue phasePlatelet phaseClotting PhaseUnstable clot PhaseClot stabilization PhaseClot retraction PhaseClot resolving Phase

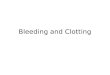
THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC
PROTHROMBIN(II) THROMBIN(III)
FIBRINOGEN
FIBRIN
(I)V
X
Tissue ThromboplastinCollagen
VIIXII
XI
IXVIII
VII
PTPTT Vit.K, Liver



Etiology
• VESSEL WALL ABNORMALITIES:
• PLATELETS DISORDER:
• COAGULATION DISORDER:

Vessel Abnormalities• increased vascular fragility• manifest by petechial hemorrhages of
skin/mucous membranes• not life threatening bleeding1. congenital: a. Ehlers-Danlos syndrome (AD)
b. hereditary hemorrhagic telangiectasia (AD)
2. acquired: a. hypersensitive vasculitis(i) drug reaction : immune complex
deposit in vessel walls(Thaizide diuetics)(ii) Henoch-Schonlein purpura
b. scurvy (vit C deficiency)
Lab: BT, Plt count, PT, PTT will be normal

VESSEL WALL ABNORMALITIES:
EHLERS DANLOS DISEASE:• Congenital disorder of collagen
synthesis • in which capillaries are poorly
supported by s/c collagen• ecchymosis are commonly
observed.

VESSEL WALL ABNORMALITIES:HERIDITARY HEMORHAGIC TELANGECTSIASIS• Dominant inherited condition.• Telengectias, are small aneurysms found on
finger tips, face, nasal passages, tongue and GIT.
• few people develop pulmonary A/V malformation.
• Pt. develops recurrent bleeding/epistaxis/ occult GIT bleeding, leads to Iron def. anemia
Rx.• Iron therapy for blood loss.• Local cautery/laser therapy for single lesion• Estrogens may be tried.

Henoch-Schonlein purpura(nonthrombocytopenic)
• generalized hypersensitivity vasculitis
• uncertain cause(immune mediated)clinical Sx:
• Purpura(palpable)• colicky abdominal pain• polyarthralgia• acute glomerulonephritis
Rx: Prednisolone for2-4 weeks

PLATELETS DISORDER:
• QUANTITATIVE PLATELETS DISORDERs
• QUALITATIVE PLATELET DYSFUNCTION :

QUANTITATIVE PLATELETS DISORDER (Thrombocytopenia)
Mechanisms:1 Failure of megakaryocytic maturation.2 Excessive platelets consumption after their
release into circulation i.e ITP, DIC etc.3 Platelets sequestration in enlarged spleen i.e
HYPERSPLEENISM. S/S:· Petechial cutaneous bleeding, intracranial
bleeding and oozing from mucus membrane & skin surface.
· Lab: decreased platelets count and prolong bleeding time.

(Thrombocytopenia) Causes:
Marrow DisorderAplastic anemiaHem. malignancyMyelodysplastic
disorderB12 deff.
Non Marrow DisorderImmune disordersITP, Drug inducedSec: ALL, SLEPost transfusionDIC, TTPHU syndrome, HyperspleenismHeamangiomasSepsisViral infection
Management:
Rx Underlying cause
Platelet transfusion

IDIOPATHIC THROMBOCYTOPENIC PURPURA(ITP)
• An autoimmune antibody IgG is formed against unknown antigen of platelets membrane/surface.
• Antipletelet antibody binds to complement, but platelets are not destroyed by direct lysis.
• Destruction takes place in spleen, where spleenic macrophages destroyes antibody coated platelets.

IDIOPATHIC THROMBOCYTOPENIC PURPURA. (Clinical Features)
In Children(acute):Often precipitated by viral infection and
usually self limited Asymptomatic not febrile. Present with mucosal/skin bleeding,
mennorrhagia, purpura, petechiae.Adults(chronic): Commonly affects female. Ratio 2:1 (male/female ratio) Peak incidence 20-50 years of age.

IDIOPATHIC THROMBOCYTOPENIC
PURPURA. Δ LAB:platelets below 10,000 /ml.Bone marrow will appear normal.RxPREDNISONONE: 1-2 mg/kg/day. Immunoglobulin: 1g/kg/day 2-3 days.DANAZOLE: 600mg/day response rate is 50%IMMUNOSUPPERESSIVE DRUGS: i-e vincristine,
vinblastine, azathioprine, cyclosprin, cyclophosphomide.
SPLEENECTOMY:Prognosis:The prognosis will be good, if disease is initially
controlled with prednisolone, spleenectomy is definite Rx.

EVANS SYNDROME:
• ITP + Autoimmune hemolytic anemia.
• These pts shows spherocytosis, reticulocytosis + anemia.

QUALITATIVE PLATELET DISORDER
CONGENITAL:Glanzmann’s
thrombosthenia
Bernard souliar syndrome
Von Willibrand’s disease
ACQUIRED
Myeloproliferative disorder.
Uremia
Drugs i-e NSAIDS Aspirin
Autoantibody
Fibrin degradation products

QUALITATIVE PLATELET DISORDERBERNARD SOULIER SYNDROME:Autosomal recessive intrinsic platelets disorder.Due to lack of glycoprotein (Gp1b), receptor for
vonWillibrand’s factor.Clinical Features:Presents with mucosal bleeding and post
operative oozes.LAB:Thrombocytopenia may be present, and Plt.s are
abnormally large in size.BT is prolonged Von Willibrand’s factor Normal Rx:Platelet transfusion

QUALITATIVE PLATELET DISORDERGLANZMANN’s THROMBASTHENIA:
Autosomal recessive disorder.Lack of receptors (glycoprotein Ib & IIIa)
for fibrinogen on platelets.Platelets fails to aggregate in respons to
ADP, collagen, thrombin.Clinical Features: Mucosal bleedingLAB:Platelets no’s and morphology are normal B.T is prolonged Rx:Platelet transfusion

QUALITATIVE PLATELET DISORDERVON-WILLIBRAND’S DISEASE:• Autosomal dominant(gene for vWF is
located on chromosome 12.)• vWF is synthesized by endothelial
cells and megakaryocytes • It acts as carrier protein for factor
VIII by non-covalent bond. A defect therefore leads to decreased plasma factor VIII level.
• It also forms bridges b/w platelets and sub endothelium.
• There fore defect of vWF leads to prolonged bleeding.

VON-WILLIBRAND’S DISEASE:Clinical Features:• Mucosal bleeding (mild-massive)LAB:• Reduced level of vWF which often
accomplished by sec: reduction in factor VIII and prolonged bleeding time (B.T)
Rx:• MILD HAEMORRHAGES:Desmopressin 0.3 μg/kg, after which vWF
levels usually raise 3 in 30-90 minutes • MASSIVE HAEMORRHAGES:Factor VIII

COAGULATION DISORDER:
Coagulation factor disorder can either due to single factor def., i.e. a “congenitaldeficiency”, eg factor VIII resulting in HAEMOPHILIA-A
or due to multiple factor def., which is an ‘’acquired” eg Sec: to liver disease or warfarin therapy.

• HEAMOPHILIA – A (CLASSIC TRUE HAEMOPHILIA)
• HAEMOPHILLIA – B (CHRISTMAS DISEASE).
• X-linked recessive Inheritance.
COAGULATION DISORDER:CONGENITAL BLEEDING DISORDER:


HEAMOPHILIA – A (CLASSIC TRUE HAEMOPHILIA)• X-linked disorder • Due to deff. of factor VIIIC/F:• Bleeding occurs as bruising at the age of 6
months.• Trauma results in excessively bleeding.• Recurrent bleeding /hemorrhage in knee,
elbow, ankle, and hip. (Hemarthrosis)• Mucus membrane /internal bleeding of
mouth, lips, gums, brain and kidney also occur• Muscle haematoma esp. calf and Psoas muscle Rx• Factor VIII infusion

Hemophilia A

HAEMOPHILLIA – B (CHRISTMAS DISEASE)
• Due to deff: of factor IX S/S:• Same in type ARx• Factor IX infusionLONG TERM COMPLICATIONCOMPLICATION due to repeated hemorrhage:• Arthropathy of large joints eg knee, elbow• Muscle atrophy due to haematoma• Mononeuropathy due to pressure of haematoma.COMPLICATION due to therapy• Antifactor VIII antibody develops• Virus transmission Hepatitis A-B-C-D + HIV

COAGULATION DISORDERACQUIRED BLEEDING DISORDER
• DIC• LIVER DISEASE • RENAL DISEASE

DISSAMINATED INTRAVASCULAR COAGULATION
• DIC is condition characterized by thrombosis within circulation.
• DIC can be induced by different mechanisms.• Due to Endothelial cell damage by endotoxins in
G –ve septicemia results in tissue factor release which in turn leads to coagulation cascade activation through extrinsic pathway.
• The presence thromboplastin from damaged tissue, placenta & fat embolus (following brain injury & Fractures) may activate coagulation
• This results in excessive consumption of platelets and coagulation factors, with secondary activation of fibrinolysis leading to bleeding tendency.

DIC:
CAUSESInfectious:• E Coli• Nessieria
meningitis• Strep pneumonia• MalariaCancer • Lung,Pancreas,• Prostate
CLINICAL FEATURES:
Bleeding & thrombosis, bleeding is more than thrombosis.
Subacute DIC:
Occurs primarily in cancerous pts results in superficial + deep venous thrombosis.
Other Manifestation:
High incidence of cardio respiratory failure

DIC
LAB:• Thrombocytopenia• Prolong PT• APTT may be normal/increased• Low fibrinogen• Increased level FDP/D-dimmer

Treatment of DIC
Rx. Underlying cause.General Measures:• Correction of dehydration• Renal failure• Acidosis and • ShockReplacement:• Platelets transfusion if platelets counts below
10,000/l• cryoprecipitate to maintain plasma fibrinogen
level above 150 mg/dl • FFP• Heparin, if there is DVT, Pulmonarythrombosis.

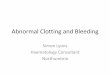
Approach to a child with bleeding disorder
Bleeding Not sick sic
kSuperficial bleeds
Deep Bleeds
CBC, BT Factor assay, Gene analysis
Bone marrow
Blood culture
CBC, Bonemarrow
LFT
RFT
FDP

THANKYOU