Embed Size (px)
Citation preview

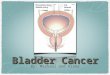
Bladder cancer Dr/omar hashim

Anatomy of bladderBladder is lie behind pubic bone,it is the
maximum storage is 500 ml.it has stronge muscular wall. It is
shape and relation according to containing volume. The
empty bladder is pyramidal ,having apex, base
superior, and two inferolateral surface. The superior surface is covered by
Peritoneum, when bladde is fills the superior surface bulges
Up ward so the bladder is become in direct contact to the
Abdomen wall.Lymphatic drange of the bladder is to the
internal and external lymph nodes







Epidemiology and etiology
the incidence of bladder cancer is 9.9/100.000 in men
And 2.3/100.000 in women in USA. New case in US in 2010
Is 70.530 .and death 13,060 .Risk factors ;-Age and gender ;-incidence ↑with age (more
common Age 60—70) .m:f ratio is 4:1Twice more common in white American than in
non cau-Cassians .Lifestyle cigarette smoking

Past medical history ;-pelvic radiation, chemotherapyBladder lithiasis,chronic catheterization, recurrent urinaryInfection exposure to schistosomiasis.Genetic factors ;-these is some gene associated withPoorer prognosis and↑chance of progression include(EGFR),P53,ras oncogene .Industrial chemicals ;- aniline dye,naphthylamineBenzidine.so aniline dye,leather,paint,and rubberWorkers more affected than general population.Drugs :-cyclophosphamide

pathologyPathologic subtypes of ca prostate;-1)Transitional cell carcinoma ;- represent 90% of bladder Cancer inUSA,70% are superficial carcinoma,arise fromNormal urohtellium and associated with smoking and Carcinogen exposure . 2) Squamous cell carcinoma;- caused by chronic irritationFrom urinary calculi,long term indwelling catheter,chronicUrinary infection,infection by schistomiasis or bladderDiverticula( transitional cell→squamous change ).The incidence is ↑in the Egypt 50%

Transitional cell carcinoma of bladder

Squamous cell carcinoma of the ca bladder

3) Adenocarcinoma ;- represent 2% ,include 3groups,1ry
Urachal and metastatic .4) Small cell carcinoma ;-represent 1%, behaves
similarly toSmall cell carcinoma found elsewhere in the body.5) Mixed histology ;- represent 25% of the
case ,usuallyTransitional with adenocarcinoma or squamous *most common site is trigone (inferiorly below ureter-Ovesical juncation,laterial wall,posterior wall,and
bladderneck

diagnosisClinical presentation ;-Hematuria is the most common presenting symptoms
75%. Irritative /obstructive symptoms occur in quarter of patients. plevic pain occur in local advanced disease
invading into adjacent organs. Poor appetite and weigth loss late systemic symptoms.Examination:- for metastatic sites / PR:- to see the local Extension .Cystoscopy:- is cornerstone procedure,biopsy should beTaken from abnormal area,of normal at random to searchFor cis, cystoscopy is followed by bimanual plevic
examination under general anesthesia

Cystoscopy is indicated in following:-a) Any gross or microscopic hematuria.b) Unexplained or chronic lower urinary tract symptomsc) Urine cytology that is suspicious for cancer.d) History of bladder cancer.CT:-to detect the 1ry sites and any enlarged LNs andMetastasis if is present.Urine cytology:-is not used for 1ry diagnosis but for Follow up of ca bladder patients/,screening for environ-Mental carcinogens/.evaluating pts with chronic irritativeBladder symptoms

Doagnosis procedure for bladder cancer;-
Hematuria or irritative bladder cancer
HX/EX /urinary cytologyCBC/CXR.*1
Invasive
Abd-u/s/pelvic CT &bones can
Superficial Muscular is -ve

Tumor,node and metastasis staging (TNM) determine byAmerican Joint Committee on Cancer (AJCC)PRIMARY TUMOR ;-
STAGE DESCRIPTION
T1
tumor invade subepithelial connective tissues
T2 tumor invade muscularis propria
T3 Tumor invade perivesical tissues
T4 Tumor invade any of the following (prostate stroma /seminal vesicle /uterus /vagina /pelvic wall /abdominal wall


Regional LNs include 1ry and 2ry drainage regions all nodesAbove the aortic bifurcation are considered distant metast-Asis ;-
N0 No regional LNs metastasis
N1 single regional LNs metastasis in true pelvic(hypogastric/obturator/external iliac or presacral )
N2 multiple regional LNs metastasis in true plevic
N3 lymph nodes metastasis to the common iliacLNs
Distant metastasis ;-M0;-no distant metastasisM1;- distant metastasis

Stage group of bladder cancer ;-
T1 T2 T3 T4a T4a
N0 1 11 111
111 1V
N1-3 1V 1V 1V 1V 1V
M1 1V 1V 1V 1V 1V

PROGNOSISStage is the most important determinant of the
survival . 5 yrs over all survival (OS) rate after
cystectomyDetermined according to stage
stage
superficialP0a,N0
Organ con-Fined p2,N0
extra vesicle p3-4,N0
nodes +ve
5yra survival
85% T2a 77% T2b 64%
47% 31% …/40%.(1-4) 25%(>4)
Type
description

Prognosis factors ;-
factor Favorable Adverse TURBT complete incomplete
Response to chemo-
complete regression
Residual disease
extent of tumor solitary Diffuse /multiple
disease invasion
organ confined Regional met-
Hydronephrosis absent present

treatmentPrinciple and practice ;- Treatment of ca bladder is multimodal and determined byPatients prognosis factors.1) Superficial bladder cancer is managed primary by trans-Urethral resection ±intravesicular chemotherapy .2) Localized invasive bladder cancer traditionally is treated
by cystectomy .3) If patient has prognostic factors predictive for bladderPreservation, the patient can be treated with chemo-Therapy . 4) mets- disease is primary treated by chemo-With palliative radiation or surgery for symptomatic control

Superficial bladder caner
TURBT
Low risk(low grade papillary)
high risk(high
grade,CIS,papillary)Superfical ca
bladder recurrence
Intravesicular
chemotherapy
Cytoscopic survellance
Every 3monthsx2yrs
then every 6months
x2yrs ,then yearly
Invasive recurrence
Bladder preservation
therapy cystectomy
Progressive high risk disease



Invasive bladder cancer
Unifocal no hydronephrosi
s/noEVD
Partial cystectomy If candidate
Local advanced disease
T3.T4;N+CTH/
preops-RT
cystectomy
CT /bone scan/NOmetastasis
Local advanc
ed disease
CTH
TURBT
CTH+RT
completeRegressio
n of disease
consolidative CTH+RT
yesno
yesno
yes

Definitive surgical intervention
Radical cystectomy ;- involve there move of the bladderProstate and lymph nodes dissection in male. In the
femaleAn anterior exenteration (removal of the bladder,urethra,Anterior vaginal wall and uterus )and pelvic lymph nodes Dissection is performed . Lymph dissection is
include(medialTo the genitofemoral/external iliac up to the bifurcation ofThe common iliac then extended to obturator fossa thenLymph nodes around hypogasteric artery then superorlyTo the aortic bifurcation and presacral LNs included .thenUrinary diversion is with segment of bowel(no continent)Or orthotopic neobladder or abdominal pouch

extent confined extra vesicle
nodes Total(NO ofpt)
Local failure
4% 16% 20% 9% 78810 yrs
distant metas-tasis
9.5% 19%
45% 18%
recurrence-free survival
T2a/b 70%10yrs
T3a/b,52%T4, 35%
15%10 yrs
45%

![Women and Bladder Cancer - Oncoscan yellow 8-20_.pdf · bladder cancer [18,170] than cervical cancer [11,270] > 500,000 people in the U.S. have/had bladder cancer – highest recurrent](https://img.pdfslide.us/doc/110x75/5f694c18ea002e289e4b0db0/women-and-bladder-cancer-yellow-8-20pdf-bladder-cancer-18170-than-cervical.jpg)