Embed Size (px)
Citation preview
Best Practices for Cancer Survivorship and
Rehabilitation
Providence St. Joseph Medical CenterApril 2014
No Financial Disclosures or Conflicts
Cancer Survivorship and Rehabilitation
• Scope of the problem
• “Lost in Transition”
• Side effects of treatment
• Definition and phases of survivorship
• Stakeholders
• Best practices
Cancer Statistics (US)
• 1.6 million patients diagnosed with cancer (2013 estimate)
• 40.8% of people will develop some form of cancer in their lifetime
• 65.8% surviving >5 years (2003-2009)
• As of 2010 there were an estimated 13 million people living with a diagnosis of cancer
Surveillance, Epidemiology and End Results www.SEER.cancer.gov
Reasons for Improved Survival• Improved identification of cancers that can sometimes be
found early through screening, such as mammography, colonoscopy, etc
• Improvements in treatment
• More effective treatment of side effects, making it possible to give patients the optimal / planned doses of cancer drugs
• The development of new treatments, such as targeted therapies
Cancer Statistics (US)
• Approximately 20% of childhood cancer survivors and 53% adult-onset cancer survivors have problems with physical function related to their cancer and treatment
• Problems may be apparent immediately or many years after treatment
Sutbblefield, Schmitz, NessSemin Oncol 2013 Dec 40(6) 784-95
Cancer TreatmentSurgery
Cancer TreatmentChemotherapy
Cancer TreatmentRadiation Therapy
YOU’RE CANCER FREE!!
From the Patients…• Feeling lost in the months after cancer treatment. Intense
period from diagnosis thru treatment, life on hold then “dropped” – told to go on my way, live my life. It’s not like I just had a cold and am now “ok”
• Media stereotype of being treated, then cancer free – reality is much more gray. No one wants to think / talk about recurrence / mets – even the docs. But there is no forever cure. Docs need to be more honest about these realities instead of buying into the false narrative
• Patience and guidance from the physicians and other support staff essential but often lacking
From the Patients…
• Transition from when oncologist ceases to be PCP is challenging for patients and physicians alike. Coordination of care difficult and important
• Rollercoaster experience. Fear, depression, PT stress, anxiety, insomnia. Accused of lack of gratitude for being alive when attempted to talk about experiences. I see everything now through a lens of gratitude, but there is the background of knowing that recurrence or metastatic disease is a real possibility
• Safety net is gone, training wheels are off
From Cancer Patient to Cancer Survivor: Lost in Transition
• Despite increase in cancer survivors, physicians not extremely familiar with consequences of cancer and treatment
• Seldom receive explicit guidance from oncologists
• Lack of clear evidence for what constitutes best practices contributes to wide variation in care
Institute of Medicine 2005www.IOM.edu
Importance of Survivorship
• Transition from active treatment to post-treatment care is critical to long-term health
• Consequences of cancer and its treatment are substantial
• Range from few late effects to permanent disabling symptoms that impair normal functioning
Institute of Medicine 2005
Side Effects of TreatmentPhysical
• Pain, limitation in range of motion, neuropathy, weakness
• Lymphedema, arthralgias• Cardiovascular, pulmonary effects• Osteoporosis• Sexual dysfunction, fertility• Alteration in appearance – alopecia, visible scars• Weight gain / loss, digestive problems• Neutropenia, anemia• Fatigue, sleep disturbance
Side Effects of TreatmentMental / Emotional
• Anxiety, Depression• Cognitive dysfunction• Sense of isolation, feeling “lost” after treatment• Accepting the “New Normal”• Fear of recurrence, metastasis• Spiritual changes• Alteration in family / friends / work relationships• Financial considerations
When Does Survivorship Start?Question from Patients
• At diagnosis?
• After surgery?
• After all active treatment has been completed?
• 5-10 years after diagnosis / surgery / treatment?
• When does the “clock” start?
Definition of Survivorship• The process of living with, through, and beyond cancer.
By this definition, cancer survivorship begins at diagnosis. It includes people who continue to have treatment to reduce the risk of recurrence or manage chronic / metastatic disease
• Using this definition, family, friends and caregivers can also be considered survivors
• Some consider family / friends “co-survivors”
• No matter how it is defined, survivorship is unique for each person
American Society of Clinical Oncology
Survivorship begins at Diagnosis
• “Survivorship beginning at diagnosis is NOT a concept. It simply is.”
• Transition from treatment to post-treatment (not treatment to survivorship); from active treatment to “watch and wait”
• Coordination of care – who is responsible (PCP vs Oncologist)
Phases of Survivorship
• Acute phase – diagnosed, but information
gathering
• Active treatment phase
• Extended / Follow up phase – getting back to
“normal”www.cancer.netDr. Robert Miller Podcast
Survivorship Stakeholders• Patient and family
• Oncologic physicians (Surgical, Medical and Radiation)
• Primary Care Physicians
• Nursing (Nurse Practitioners, Nurse Navigators, Oncology Nurses)
• Psycho-Social Support (Social Work, Psycho-oncology, counselors, spiritual care)
• Other Clinicians (PA’s, Pharmacy, Research Staff, Palliative Care, Genetics, Nutrition, PT/OT, Rehabilitation, etc.)
Lifelong Surveillance• Current Model: focuses on treatment of disease,
followed by ongoing surveillance to detect recurrence
• Evidence supports prospective surveillance for early identification and treatment as a means to prevent or mitigate many of these concerns
Stout, et alCancer 118:2191-2200
Lifelong Surveillance
• Female adult survivors of Hodgkin’s lymphoma treated at a young age with mantle irradiation are at a high risk for subsequent breast cancer, but only 47% reported having had a mammogram in the past 2 years.
• As many as 40% were unaware of their increased risk
Diller et al 2002
Lifelong Surveillance
• Breast cancer survivors report knowing little about lymphedema before developing it, and physicians report not routinely counseling women or providing written information on lymphedema prevention to their patients with breast cancer
Paskett and Stark 2000
Lifelong Surveillance
• Only about half of men and women with cancer who are of childbearing age receive timely information from their health care providers about their risk of infertility and options to preserve or restore fertility
Canada and Schover 2005

Best Practices• Establish survivorship as a distinct phase of
cancer care
• Ensure the delivery of appropriate survivorship care
• Provide patients with a comprehensive treatment summary and follow-up plan
• Develop quality of care measures for survivorship
Institute of Medicine 2005
IOM Standards for Survivorship Care
• Prevention of new and recurrent cancers and other late effects
• Surveillance for cancer spread, recurrence, or second cancers
• Assessment of late psychosocial and medical effects
• Intervention for consequences of cancer treatment (medical problems, symptoms, psychologic distress, financial and social concerns
• Coordination of care between PCP and specialists to ensure that all of the survivor’s health needs are met
Institute of Medicine 2005
Best Practices / Standards
• National Comprehensive Cancer Network (NCCN)
• Institute of Medicine (IOM)
• American Society of Clinical Oncology (ASCO)
• American College of Surgeons Commission on Cancer (ACS CoC)
• Livestrong
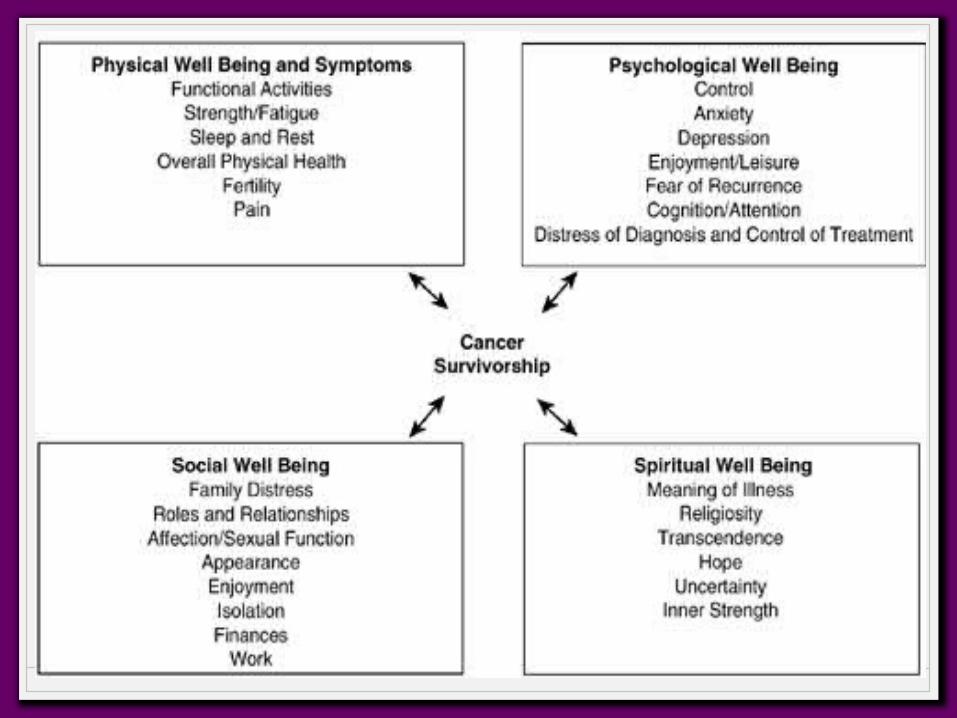
Survivorship Care PlansQoL Model
• Physical Well Being and Control of Symptoms
• Psychological Well Being
• Social Well Being
• Spiritual Well Being
Survivorship Care PlanEssential Components
• Treatment summary - dates of the diagnosis, reports, test results, and treatment details
• On-going care - tests for recurrence, identifying and managing late and long-term effects of cancer and treatments
• Healthy behaviors recommendations - diet, exercise, sunscreen, smoking cessation, osteoporosis prevention, emotional / psychosocial support
• Contact information for all of treating MDs, therapists, integrative care providers. Identify point of contact
Survivorship Care PlanEssential Components
• Documentation of patient’s understanding of predicted recurrence rates, QoL expectations; description of recommended screening / schedule
• If appropriate, chemoprevention strategies
• Reinforce the need for ongoing health maintenance or therapy
• If appropriate, genetic counseling / testing, recommendations for screening for family members
• Information on potential insurance / employment / financial considerations; referral for counseling / aid / assistance
Survivorship Care PlanEssential Components
• Involvement of primary care providers
• Available in multiple languages
• Available for all disease sites
• Listing of cancer-related resources and information (print, online, telephone)
• Consideration of a survivorship clinic or addition to multidisciplinary program
• Establish metrics for evaluating the program performance
Other Providers and Role
• Rehabilitation specialists – PT, OT, speech and language pathologists –
• Neuropathy• Balance• Lymphedema, scarring• Fitness programs for strength and flexibility
• “My PT is my angel”
Role of Physical TherapyScar / Radiation Fibrosis
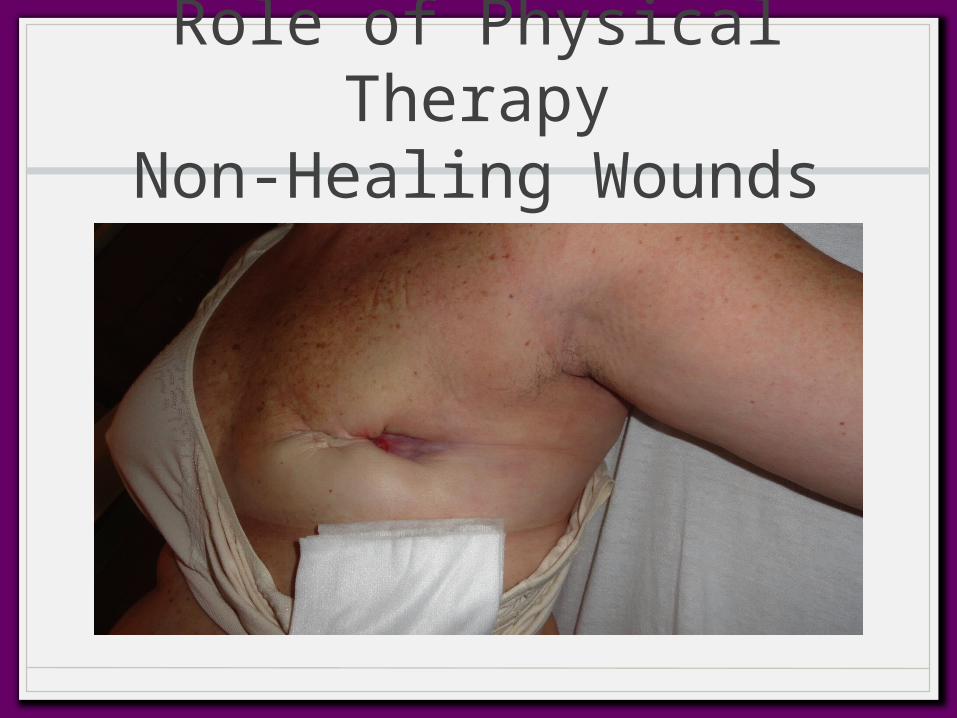
Role of Physical TherapyNon-Healing Wounds
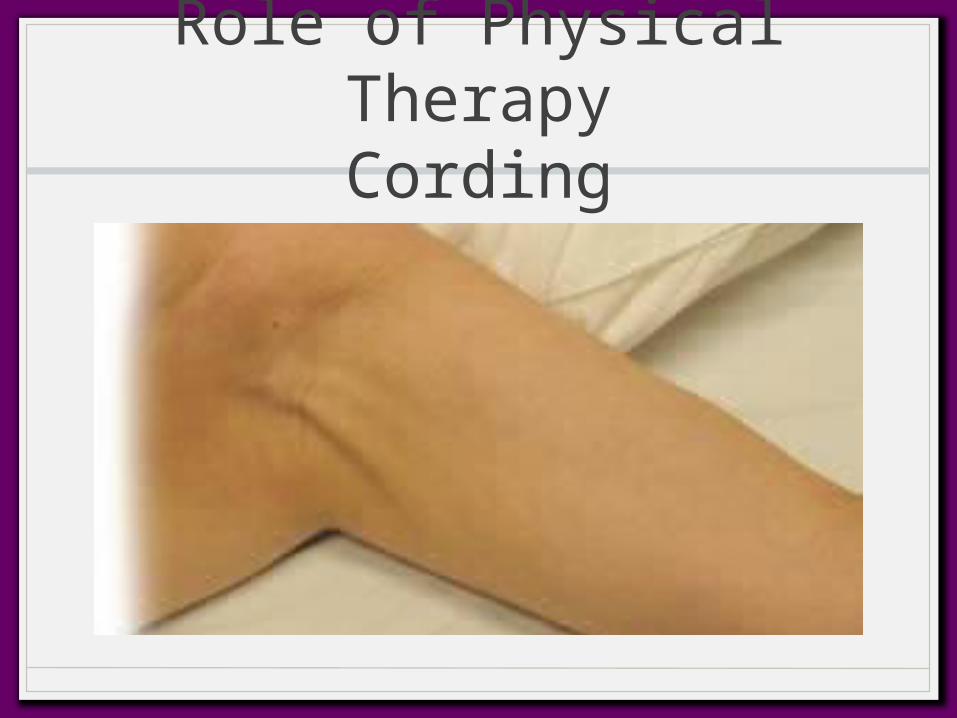
Role of Physical TherapyCording
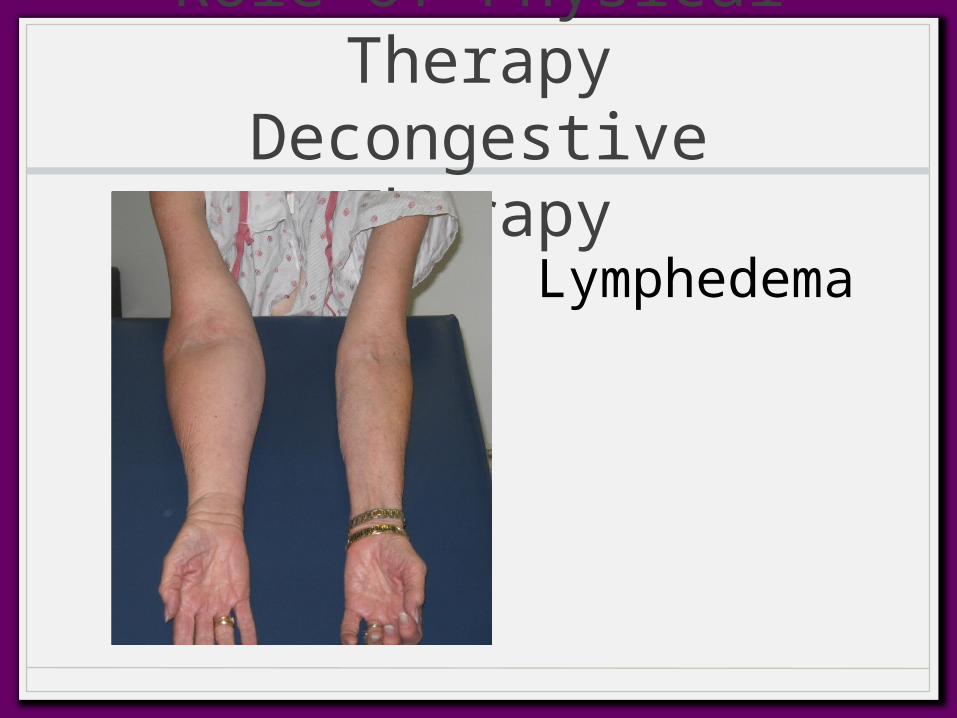
Role of Physical TherapyDecongestive Therapy
Lymphedema
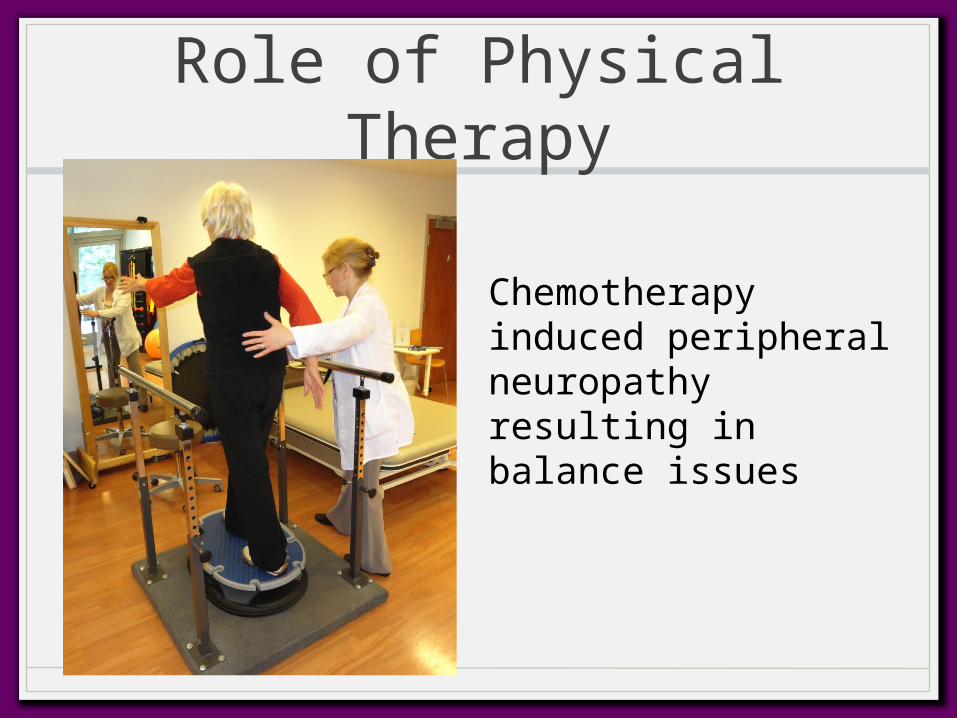
Role of Physical Therapy
Chemotherapy induced peripheral neuropathy resulting in balance issues
Other Providers and Role
• Psychosocial and mental health providers – social worker, psychologist, psychiatrist, rehabilitation counselor, marriage and family therapist, spiritual counselor
• Various forms of counseling and therapy• Home care services• Vocational counseling• Support groups, survivor matching
Other Providers
• Genetic counselor
• Nutritionist
• Pain management
• Complementary therapists
• Research coordinators – clinical trials focusing on QoL
System Barriers to Optimal Survivorship Care
• Fragmented, poorly coordinated cancer care system
• Absence of ownership of responsibility for follow up care
• Poor mechanism for communication
• Lack of guidance on specific tests, exams, and advice that make up survivorship care
• Inadequate reimbursement from insurers for some aspects of care
• Limited experience on the best way to deliver care
System Barriers to Optimal Survivorship Care
• Consequence of poorly coordinated care is poor-quality care – cancer survivors may not receive the necessary non-cancer care if cancer diagnosis shifts attention away from care that is routine but necessary (heart disease, diabetes, recommended preventative services)
• Collaborative approach between oncologists and primary care physicians is essential
Patient Barriers to Optimal Care
• Lack of availability
• Lack of access to care due to cost, lack of insurance coverage
• Education, awareness – health literacy
• Language, cultural barriers
• All of the above lead to racial, economic, and geographic disparities in care and outcomes
The Label “Survivor” is not universally embraced by patients• The celebrations cast the survivor in the role of hero and winner.
Survivors of other devastating personal traumas (fires, flood, etc) rarely use the celebratory hero language. Mostly they speak of themselves as being lucky.
• I’m not comfortable with that word, “survivor,” which connotes some sort of superhero who has battled and defeated the demon known as cancer. The problem is that there’s a blame game going on: those who survive did something heroic; those who don’t survive just weren’t tough enough
• Survivor, to me, sounds too triumphal, too final, like it’s finished – all over. But breast cancer is not like that – as I am finding – now approaching four years from diagnosis
The Survivors View“I wish I'd known earlier that survivorship care is neither a do-it-yourself project nor is it something that I can simply hand off to experts. There is no stable set of signs, signals and test protocols that, if followed assiduously — and that come up negative — means I am protected from a recurrence, new cancer or late effects of treatment. Observation, expertise and self-knowledge from both me and my doctor are critical to getting the best follow-up care.”
Jessie Gruman, August 2013www.CFAH.org/blog
The Survivors View
“This is a mutual enterprise, my survivorship care. Without me, my careful monitoring of my own health and willingness to act to find good solutions, my doctor has nothing to work with. Without my doctor, his careful monitoring of research developments, his wealth of experience with other patients and his ability to personalize what he knows for my unique history, I have no guidance to discover and address the long-term effects of cancer treatment.”
Jessie Gruman, August 2013www.CFAH.org/blog
Conclusions
• While cancer treatments have improved, they still result in significant short and long-term complications
• As a goal of cancer treatment is to preserve QoL, focus on the complications of treatment is necessary even before treatment starts
• An integrative model of cancer survivorship including all of the stakeholders with a focus on the patient will result in the best QoL and outcomes for our patients
Thank you