Embed Size (px)
Citation preview

Benign Paroxysmal Positional Vertigo

CONTENT
1
2
3
4
5
Anatomy/BPPV Characteristics
Epidemiology
Review of literature
Interventions
Discussion
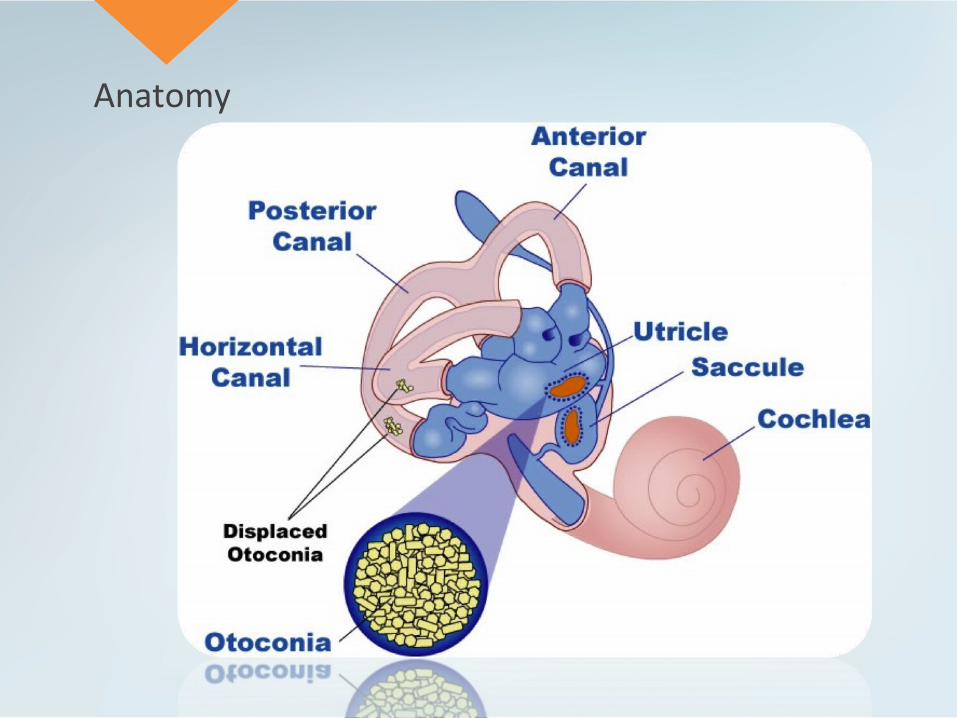
Anatomy

What is BPPV?
• Occurs when one of the crystals dislodge and enter the semicircular canals
• One of the most common causes of vertigo
• Characterized by brief episodes of mild to intense dizziness associated with positions

Epidemiology
• Idiopathic in 50-70% of the cases• Head trauma accounts for 7-17% of the cases• Female male ratio 2:1• Mean age of 50 years old• Posterior canal most common• Commonly missed after head trauma6

Review of Literature
342 BPPV articles were identified, only 4 articles met the inclusion criteria of:•Diagnosis of Anterior BPPV•Unilateral canal involvement•Interventions specifically designed for ACBPPV•Diagnosis made with Dix-Hallpike test•Outcome based measures were presented

Comparing treatments
• After one treatment Yacovino9, Korres8, Kim11, and Casani10 demonstrated resolution rates of 85%, 60%, 47% and 44%
• In terms of two treatments Yacovino9 and Korres8 demonstrated 100% resolution rate.
• Yacovino et al.9 appeared to be the most effective maneuver for treating AC-BPPV
Patient Demographics
• Gymnastics All-around athlete• 20 year old • Sophomore • Has past medical history of concussions
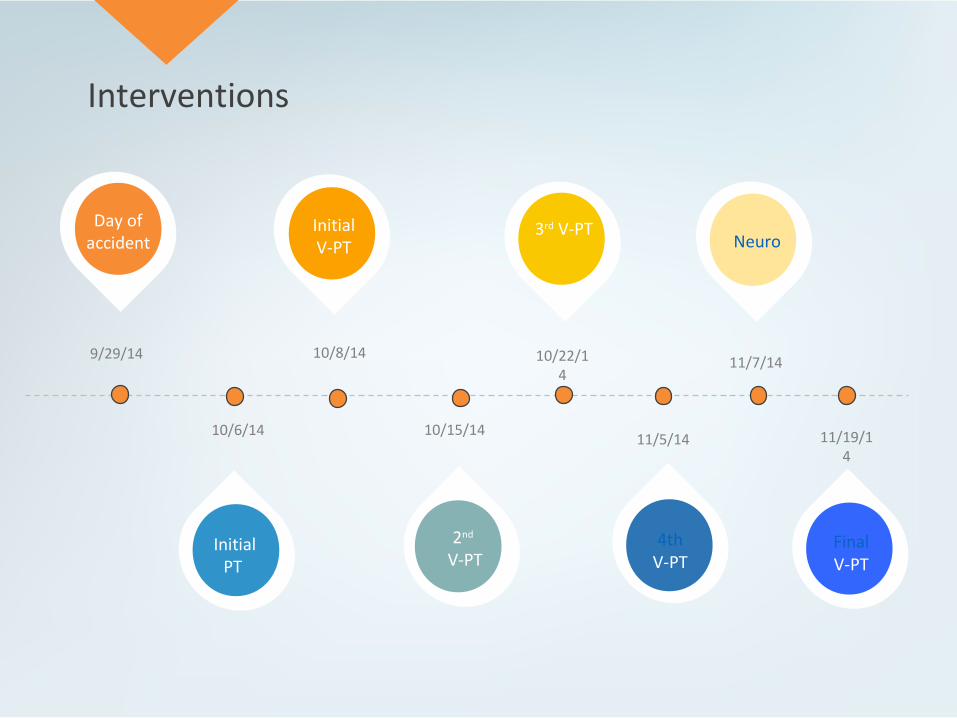
Interventions
Day of accident
Initial V-PT
3rd V-PT
Initial PT
2nd V-PT
9/29/14
10/6/14
10/8/14
10/15/14
10/22/14
11/5/14
4thV-PT
11/7/14
11/19/14
Neuro
FinalV-PT

September 29, 2014
Mechanism: The patient was performing a dismount on the bars when she under rotated and landed on her chest with her forehead on the mate
Symptoms: nausea, dizziness, feeling foggy, 7/10 headache, 7/10 neck pain, and demonstrated unsteady walking.
Plan: ATC placed a c-collar on the patient and was immediately rushed to the emergency room in Winona Health to rule out neck fracture
↵

October 6, 2014
• Pain localized to the mid and upper cervical
• Patients active ROM was within normal limits
• Cervical flexion 4/5 with a pain level of 6/10 noted• Cervical extension 4/5 pain level of 5/10• Cervical left rotation 4/5 with a pain level of 3/5• Cervical Right rotation pain of +4/5 with a pain level of 4/5• Bilateral flexion was 4/5 with a pain level of 4/5.
• Distraction and compression were negative and had no signs of radicular symptoms.
• Isometric exercises with scapular retraction exercises. Stretches were prescribed in all directions
↵

October 8th, 20141st Vestibular PT appointment
• Post concussion symptom scoring scale with a grand total of 48 • Dizziness provocation movements • Sense of being off-balance
• Tandem Romberg eyes open: 25 seconds bilaterally• Tandem Romberg eyes closed: 15 seconds bilaterally• Single leg stance eyes open: 30 seconds bilaterally• Single leg stance eyes closed: <5 seconds bilaterally
• Frenzel lens testing: Positive Dix-Hallpike (Downbeating Nystagmus) • https://www.youtube.com/watch?v=wgWOmuB1VFY (:09-:53sec)

Rehab Exercises: •Right Forward Roll followed by Yacovino 1x/day•Saccades in single leg stance. 2 x 15reps, 3x/day
October 8th, 2014 Rehab home program
↵

↵
October 15th, 2014 2nd Vestibular PT appointment
• “Headache and dizziness are better. Neck feels a lot better”
• The patient still gets dizzy with laying down to sitting up, sit to stand, looking up, slight with turning her head, and side to side flexion
• Today the patient presented the post concussion symptom scoring scale with a grand total of 41, was 48 on October 8th, 2014.
• With Frenzel Lens testing, on the affected side there was a positive for a very small right downbeating nystagmus and dizziness.

↵
• Canalith repositioning maneuver utilizing a Modified Semont’s Maneuver for Right Anterior Canal Canalithiasis
• Saccades in single leg stance: 2x 20 seconds, 3x/day
• Cervical Joint positioning exercise with laser.
October 15th, 2014 Rehab home program

↵

↵
October 22nd, 2014 3rd Vestibular PT appointment
• “Headache and dizziness are better; neck is still doing well”
• Gets dizzy laying down to sitting up
• Today the patient presented the post concussion symptom scoring scale with a grand total of 20, was 41 on October 15th, 2014
• Continues to experiences a sense of being off-balance and poor convergence
• Cervical JPE 4/6 incorrect
• With Frenzel Lens testing, negative for nystagmus or dizziness

October 22nd, 2014 Rehab home program
• Canalith repositioning maneuver utilizing a Left Eply Maneuver for Right Anterior Canal Canalithiasis 1-2x/day
• Pencil push ups 2x/day
• Single leg stance at counter, gaze fixed with horizontal head movement for 3x 30 seconds 2x/day
• Single leg stance at counter gaze moving with horizontal head movement for 30 seconds. 2x/day
• Single leg stance at counter, eyes closed, 3 x 30 seconds for 2x/day
↵

November 5th, 20144th Vestibular PT appointment
↵
• “Headache and dizziness are better overall and neck is doing well”
• Dizzy with laying down to sitting up if she does it too fast
• Today the patient presented the post concussion symptom scoring scale with a grand total of 11, was 20 on October 22nd, 2014.
• SET back: With Frenzel Lens testing, the Dix-Hallpike maneuver found a positive for dizziness and right down torsional nystagmus.
• Cervical JPE 5/6 incorrect
• Balance improvements:• Tandem Romberg eyes open: 25 seconds bilaterally• Tandem Romberg eyes closed: 30 seconds bilaterally• Single leg stance eyes open: 30 seconds bilaterally• Single leg stance eyes closed: 30 seconds bilaterally

• Right Forward Roll, every other day
• Yacovino Maneuver, every other day
• Brock String training 2x/day
• Cervical retraction/Rotation 2x5, 2x/day
November 5th, 2014 Rehab home program
↵

November 7th, 2014 Neur-ophthalmologist appointment
• The neuro-ophthalmologist states that the patient’s distance vision is “good” better than 20/20.
• The neuro-ophthalmologist states that convergence is the current problem• The neuro-ophthalmologist states that the patient does have good near vision

November 10th, 2014 Treadmill test
Minutes Incline Speed HR (bpm)
Baseline 62bpm
0-5min 12 3.0 140bpm
5-10min 12 3.0 128bpm
10-15min 12 3.3 132bpm
15-20min 3.0 4.2 144bpm
20-25min 3.0 4.2 168bpm
25-30min 3.0 4.2 164bpm
30-35min 3.0 4.2 180bpm
35-40min 3.0 4.2 176bpm
40-50min 3.0 4.2 178bpm

November 14th, 2014 2nd Treadmill test
Minutes Incline Speed HR (bpm)
10min warm-up 15 3.0 124bm
10-15min 4.0-4.8 5.0
15-20min 4.8 5.0
20-25min 4.8 5.0 180bpm
25-30min 4.8 5.0 182bpm
↵

November 19th, 2014 Final Vestibular PT appointment
• Only has headaches after studying or reading for more than an hour or working out at a heart rate >170-180bpm
• She no longer getting nauseous during her classes and has resumed attending all classes.
• Today the patient presented the post concussion symptom scoring scale with a grand total of 4, was 11 on November 5th , 2014
• Cervical JPE exercises the patient was incorrect 5/6 times again.
• Balance:• Tandem Romberg eyes open: 30 seconds bilaterally• Tandem Romberg eyes closed: 30 seconds bilaterally• Single leg stance eyes open: 30 seconds bilaterally• Single leg stance eyes closed: 30 seconds bilaterally
• Cervical joint position error training with laser: 2 x 10 every other day
• Convergence exercises 10 reps , 2x/day
• BPPV exercises as needed
November 19th, 2014 Home Program

December 8th, 2014 BESS Test
Firm Surface Soft Surface
Double Leg Stance 0 0
Single Leg Stance 3 7
Tandem 0 4
Total: 3 11
Retest on January 14th, 2015
Firm Surface Soft Surface
Double Leg Stance 0 0
Single Leg Stance 0 5
Tandem 0 1
Total: 0 6

Outcomes
• The patient had no concussion like symptoms with reading, studying, watching TV, and listening to music.
• No symptoms reported with exercising • The patient was able to preform ADL’s without any symptoms
reported.
Meet all her physical therapy goals of: • Resume all ADL’s with symptoms below 1-2/10 in order to improve
quality of life,• No nystagmus in the infrared Frenzel lenses indicating BPPV in order
to reduce dizziness/imbalance symptoms, • Demonstrated of improved balance score to >30 seconds with eyes
closed in order to reduce risks of falls, • Demonstrate independently self treatment maneuvers and know
when to apply them if their vertigo symptoms returned.
Compared to the Literature
• BPPV symptoms such as having episodes of vertigo and nystagmus when she is rotating, extending, and flexing her head, as well as bending over, sitting down from standing up
• Several studies4-6 mentioned that the number of women was approximately twice that of men
• Dix-Hallpike maneuver
• Yacovino maneuver

Questions raised?
• Patient adherence to the take home program? • Literature articles did not perform any other
maneuvers in conjunction?• Are there other treatment options?
Salient features
• Patient reported common BPPV symptoms of dizziness, imbalance, difficulty concentrating, and nausea
• Hanging the head’s position with respect to gravity precipitates many of the symptoms
• Dix-Hallpike Maneuver• Yacovino maneuver

Conclusion
• Patient was very easy to work with and extremely aware of her situation and understanding of our recommendations
• The sole purpose of this case study was to educate health care practitioners about BPPV and maneuvers that we may utilize to make our head assessments more accurate
• Different approach

• Xiang-Dong G. Benign paroxysmal positional vertigo. Journal of Neurosciences in Rural Practice. 2011;2(1):109-110.
• Purves D, Augustine GJ, Fitzpatrick D, et al., editors. Sunderland (MA): Sinauer Associates; 2001.
• Fife TD. Benign paroxysmal positional vertigo. Seminars in neurology. 2009;29(5):500-508.
• Soto-Varela A, Santos-Perez S, Rossi-Izquierdo M, Sanchez-Sellero I. Are the three canals equally susceptible to benign paroxysmal positional vertigo? Audiol Neurootol. 2013;18(5):327-34.
• Parnes L, Agrawal S, Atlas J. Diagnosis and Management of Benign Paroxysmal Positional Vertigo (BPPV) 2003; 169(7): 681-693.
• Liu H. Presentation and outcome of post-traumatic benign paroxysmal positional vertigo. Acta Otolaryngol. 2012;132(8):803-6.
• Kinne BL, Crouch NA, Strace CL. Anterior canal benign paroxysmal positional vertigo treatment techniques. Physical Therapy Reviews 2014; 19(2): 79-85

• Korres S, Riga M, Sandris V, Danielides V, Sismanis A. Canalithiasis of the anterior semicircular canal (ASC): treatment options based on the possible underlying pathogenetic mechanisms. Int J Audiol. 2010 Aug;49(8):606-12.
• Yacovino DA, Hain TC, Gualtieri F. New therapeutic maneuver for anterior canal benign paroxysmal positional vertigo. J Neurol. 2009;256(11):1851-5.
• Casani AP, Cerchiai N, Dallan I, Sellari-franceschini S. Anterior canal lithiasis: diagnosis and treatment. Otolaryngol Head Neck Surg. 2011;144(3):412-8.
• Kim YK, Shin JE, Chung JW. The effect of canalith repositioning for anterior semicircular canal canalithiasis. ORL J Otorhinolaryngol Relat Spec. 2005;67(1):56-60.
• Herdman, S. (1996). "Physical therapy in the treatment of patients with Benign Paroxysmal Positional Vertigo." Neurology Report 20(3): 46-53.
• Sacco R, Burmeister D, Rupp V, Greenberg M. Management of Benign Paroxysmal Positional Vertigo: A Randomized Controlled Trial. Journal Of Emergency Medicine (0736-4679) [serial online]. April 2014;46(4):575-581.

THANK YOU





























