Embed Size (px)
Citation preview

DR.ABDULHAFED ALHEMYARI
Benign brain tumours

The benign brain tumours may be intimately associatedwith, and surrounded by, the adjacentbrain, but the tumour cells do not invade the underlyingbrain. This is in contradistinction to thegliomas, which are intrinsic brain tumours activelyinvading the adjacent brain. This chapter
will discuss the more common benign brain tumours—meningioma and acoustic neuroma—
and give a brief description of the less commontumours: haemangioblastoma, epidermoid anddermoid cysts and colloid cysts.

Meningioma
Meningiomas are the most common of the benignbrain tumours and constitute about 15% of all intracranialtumours, being about one-third of thenumber of gliomas. Although they may occur atany age, they reach their peak incidence in middleage, are very uncommon in children andoccur more frequently in women than men.

The term meningioma was introduced byHarvey Cushing in 1922, although the tumourhad been described in the late eighteenth century.The tumour arises from the arachnoid layer of themeninges, principally the arachnoid villi andgranulations.

Aetiology
As for other brain tumours, no definite aetiologicalfactor has been identified. However, thepossibility that head trauma predisposes to thedevelopment of meningioma has been the subjectof controversy for many years. Although epidemiologicalstudies do not support trauma as

an aetiological factor, there have been casesreporting the development of meningiomas atthe site of substantial meningeal trauma.Meningiomas are known to occur followinglow levels of irradiation as was given in the pastfor tinea capitis, and an analysis of the Nagasakiatomic bomb survivors found a high correlationbetween the incidence of meningiomas and thedistance from the epicentre of the explosion

Meningiomas occur with a high frequency inpatients with neurofibromatosis type 2 (NF2)
(often multiple .)This association has promptedcytogenetic studies, which have shown thatmonosomy of chromosome 22 is the mostcommon chromosomal abnormality noted inmeningiomas, occurring in 50–80% of sporadictumours.

In addition, alterations of many otherchromosomes (including chromosomes 1, 6, 9, 10,
11 ,13 ,14 ,18 and 19) have been noted to beinvolved in the formation and progression ofmeningioma.

The importance of sex hormones and their receptorsin meningioma is suggested by the 2–4times incidence in females. Oestrogen binds inless than 30% of meningiomas, with the majorityof those receptors being type II subtype, thathave a lower affinity and specificity for oestrogenthan the classic type I receptor usually found inbreast cancer. Progesterone receptors are muchmore commonly associated with meningiomas,occurring in 50–100% of tumours tested.

Position of meningiomas(
Meningiomas arise from the arachnoid layer ofthe meninges, especially the arachnoid cap cellsThe most common location is in the parasagittalregion arising either from the wall of the superiorsagittal sinus (parasagittal) or from the falx
(falcine .)Less frequently the tumours may arisefrom the convexity of the cranial vault, wherethey are particularly concentrated in the region ofthe coronal suture.

Sphenoidal ridge meningiomasare divided into those that arise from theinner part of the lesser wing of the sphenoid andthe adjacent anterior clinoid process, and thosearising from the outer sphenoidal ridge, comprisingthe greater wing of the sphenoid and theadjacent pterion (the junction of the temporal,parietal and frontal bones). Less frequently, thetumours may arise from the olfactory groove, tuberculumsella (suprasellar), floor of the middlecranial fossa, cavernous sinus or posterior fossa
(Table 7.1.)

Position of intracranial meningiomas.)%(
Parasagittal and falx 25Convexity 20Sphenoidal wing 20Olfactory groove 12Suprasellar
12Posterior fossa 9Ventricle 1.5Optic sheath
1.5

Meningiomas usually occur as a single intracranialtumour but multiple intracranialmeningiomas may present in NF2

Pathology
Unlike gliomas, where the classification system isbased on the histological appearance of the tumour,meningiomas are usually classified accordingto their position of origin rather than theirhistology. The reason for this is that the biologicalactivity of the tumour, the presenting features,the treatment and prognosis are all related moreto the site of the tumour than to the histology

The major histological types are listed below. •Syncytial or meningotheliomatous—sheets of
cells with varying amounts of stroma. •The transitional type is characterized by

whorls of cells which may undergo hyalin degenerationwith subsequent deposition of calciumsalts. These calcified concentric psammomabodies form the characteristic feature of manytransitional meningiomas but they may also bepresent in the syncytial or fibroblastic types

The fibroblastic type contains abundantreticulin and collagen fibres.
•Angiomatous meningiomas are much lesscommon and their characteristic feature is thepredominance of vascular channels separatedby sheets of cells. Histologically, these tumoursresemble cerebellar haemangioblastomas.

Malignant meningiomas occur infrequently.The indications of malignancy include cellularpleomorphism, necrosis, increased numbers ofmitotic figures and local invasion of brain. Atypicalmeningiomas are tumours that lack thehistological features of malignancy, but have abiological behaviour intermediate between thetypical and malignant meningioma. These tumoursare most likely to recur

Clinical presentationMeningiomas present with features of:
•raised intracranial pressure •focal neurological signs
•epilepsy.The position of the tumour will determine thefeatures of the clinical presentation. The tumoursgrow slowly and there is frequently a long history,often of many years, of symptoms prior tothe diagnosis

Parasagittal tumours (Fig. 7.2)
These tumours most often arise in the middlethird of the vault and the patient may presentwith focal epilepsy and paresis, usually affectingthe opposite leg and foot as the motor cortex onthe medial aspect of the posterior frontal lobe isaffected. Tumours arising anteriorly are oftenbilateral and patients present with features ofraised intracranial pressure. As these tumoursinvolve the frontal lobes, pseudopsychiatricsymptoms, as well as impairment of memory,intelligence and personality, may occur. Urinaryincontinence is occasionally a symptom of a large

frontal tumour, especially if it is bilateral.Tumours arising from the posterior falx mayaffect the parieto-occipital region and produce ahomonymous hemianopia. If the tumour liesabove the calcarine fissure the inferior quadrantis more affected; when the tumour is below thefissure the upper quadrant is predominantlyaffected.

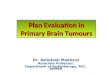
Parasagittal meningioma. (a) CT scan.
(b )MRI.

Convexity tumours (Fig. 7.3)
Convexity tumours may grow to a large size if situated in front of the coronal suture. They present with raised intracranial pressure. Moreposterior tumours will cause focal neurologicalsymptoms and focal epilepsy.

Fig. 7.3 Convexity meningioma. (a) CT scan. (b) MRI.

Sphenoidal ridge tumours (Fig. 7.4
Tumours arising from the inner sphenoidalridge cause compression of the adjacent opticnerve and patients may present with a history ofuniocular visual failure. If the tumour is largeenough to cause raised intracranial pressure papilloedemawill develop in the contralateral eye.

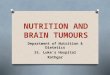
Fig. 7.4 (a) CT scan. Hyperostosis of the leftsphenoidal ring causing unilateral proptosis dueto a sphenoidal ring meningioma. (b) MRI. Innersphenoidal wing meningioma.

The presenting features of primary optic atrophyin one eye and papilloedema in the other isknown as the Foster Kennedy syndrome, andwas described in 1911. Inner sphenoidal ridgetumours may also cause compression of theolfactory tract, resulting in anosmia.

Patients with tumours involving the outersphenoidal ridge present with features of raisedintracranial pressure, often severe papilloedemawith relatively inconspicuous localizing symptomsthin sheet, and are known as ‘en plaque’. Theymay cause an excessive bony reaction (hyperostosis)resulting in proptosis (Fig. 7.4).or signs. Tumours in this region occur as a

Olfactory groove tumours
Olfactory groove meningiomas cause anosmia,initially unilateral and later bilateral. The presentingfeatures may include symptoms of raisedintracranial pressure, and failing vision eitherfrom chronic papilloedema or from direct compressionof the optic nerve or chiasm causingvisual field defects. These tumours may alsopresent with the Foster Kennedy syndrome andthe intellectual and psychiatric problems causedby frontal lobe compression described for innerspheroidal ridge meningiomas.

Fig. 7.5 (a) CT scan. Olfactory groove meningioma.
(b )MRI. Olfactory groove meningioma extending onto tuberculum sella and over pituitary fossa.

Posterior fossa tumours (Fig. 7.8)
Posterior fossa tumours may arise from the cerebellarconvexity or from the cerebellopontineangle or clivus. The cerebellopontine angle tumourssimulate an acoustic neuroma with symptomsinvolving the acoustic nerve, trigeminalnerve and facial nerve, ataxia due to cerebellar involvementand raised intracranial pressure, oftendue to hydrocephalus caused by obstruction ofthe 4th ventricle. Meningiomas arising from the

clivus or the foramen magnum region may compressthe brainstem directly.

Fig. 7.6 Tuberculum sellae meningioma. (a) CT scan.
(b )MRI

Radiological investigations
The CT scan appearance shows a tumour ofslightly increased density prior to contrast; itenhances vividly and uniformly following
intravenous contrast. Hyperostosis of thecranial vault may be a focal process at the site the tumour attachment or, as seen with en plaquemeningioma, a more diffuse sclerosis. Thesebone changes may also be seen on plain skullX-ray.of

Magnetic resonance imaging will demonstratemeningiomas following the intravenous injectionof gadolinium contrast (Figs 7.9–7.11).Meningiomas are usually isointense on T1-
weighted images, but enhance intensely and usuallyhomogeneously following administration ofgadolinium. Cerebral angiography is no longernecessary as a diagnostic investigation but maybe useful preoperatively to ascertain the positionof the cerebral vessels.

It will demonstrate externalcarotid artery supply to the tumour with acharacteristic tumour blush, differentiating itfrom a glioma or metastatic tumour (Fig. 7.12).Angiography also allows preoperative embolizationof the tumour, if necessary.

Preoperative management
Meningiomas are frequently surrounded by severecerebral oedema and patients should betreated with high-dose steroids (dexamethasone)prior to surgery if possible. Preoperativeembolization of the tumour vasculature may beconsidered advisable in some anterior basaland sphenoidal wing tumours where the majorvascular supply is not readily accessible in theearly stages of the operation.

Fig. 7.8 (a) CT scan. Meningioma arising in thecerebellopontine angle and from the tentorial edge.
(b )MRI. Clivus meningioma. (c) MRI. Foramenmagnum meningioma.

Treatment
The treatment of meningiomas is total surgicalexcision, including obliteration of the dural attachment.Although this objective is usually possiblethere are some situations where completeexcision is not possible because of the position ofthe tumour. Tumours arising from the clivus, infront of the brainstem or those situated withinthe cavernous sinus, are notoriously difficult toexcise without causing serious morbidity.

Radiation therapy may be used to treatresidual tumours following subtotal resection in order to reduce the risk of recurrent growth,Stereotactic radiotherapy has been used totreat small meningiomas (less than 3 cm in diameter),particularly if the tumours are located inportions not easily amenable to surgery, or in theelderly or medically infirm patient .

Clinical studies have shown short-term controlrates of over 90%, but long-term studies willbe necessary to prove the efficacy and safety offocused radiation treatment

Fig. 7.10 MRI. Falcine meningioma. (a) Before contrasttumour is iso- or hypodense. (b) Tumour enhanceswith intravenous contrast

Fig. 7.11 MRI. Extensive parasagittal meningioma.
(a )Sagittal view. (b) Coronal view

Fig. 7.12 Cerebral angiogram of olfactory groove meningioma showing displacement of anterior cerebral arteries
(a,b )and the characteristic tumour blush, usually due to the external carotid artery supply (c

Postoperative management
The postoperative care of patients following excisionof a meningioma involves the routine managementof patients following a craniotomy butwith particular attention to the minimization ofcerebral oedema. Steroid therapy is continuedinitially and gradually tapered .

Care is taken toavoid excessive hydration and the patient isnursed with the head of the bed elevated to promotevenous return. Neurological deteriorationrequires urgent assessment and a CT scan willdetermine the pathological cause, either postoperativehaemorrhage or cerebral oedema

Tumour recurrence
The risk of tumour recurrence depends on theextent of tumour excision. When the tumourand its dural origins are completely excised, therisk of recurrence is remote. The most commonsource of recurrence is from a tumour that hasinvaded a venous sinus and which was not resected
(e.g. superior sagittal sinus or cavernoussinus). Recurrence is more common if the tumourhas histological features of malignancy.

Meningeal haemangiopericytoma
Meningeal haemangiopericytoma is a malignantneoplasm with sarcoma-like behaviour. It wasoriginally classified by Cushing and Eisenhardtin 1938 as an angioblastic variant of meningioma.The tumour’s radiological and macroscopic appearanceresembles a vascular meningioma, butit arises from the meningeal capillary pericyteand typically contains a subpopulation of cellsthat express factor VIIIa.

The tumour incidence is 2–4% of meningiomaand it is slightly more common in males than infemales.The presenting features are dependent on thetumour location, with symptoms usually beingpresent for less than 1 year

Acoustic neuroma
Acoustic schwannomas arise from the 8th cranialnerve and account for 8% of intracranial tumours.Schwannomas occur less frequently onthe 5th cranial nerve and rarely involve othercranial nerves. The acoustic schwannoma takesorigin from the vestibular component of the 8thcranial nerve near the internal auditory meatus,at the transition zone where the Schwann cellsreplace the oligodendroglia. As such it shouldmore correctly be called a vestibular schwannoma,although the term acoustic neuroma orschwannoma is more commonly used.

Macroscopically, the acoustic schwannoma islobulated with a capsule that separates it fromthe surrounding neural structures. Small tumoursusually arise from within the internalauditory canal and occupy the porus of the internalauditory canal and, as the tumour grows, the8th nerve is destroyed and the adjacent cranialnerves become stretched around the tumour. The7th nerve is typically displaced on the ventraland anterior surface of the tumour and thetrigeminal nerve is carried upwards and forwardsby the upper pole.

The 6th nerve lies ventraland usually medial to the major mass and thelower cranial nerves are displaced around the inferiorpole of the tumour. As the tumour growsmedially it compresses and displaces the cerebellumand distorts the brainstem. Large tumourswill result in obstruction of the 4th ventricle andBilateral acoustic neuromas are the hallmark ofneurofibromatosis type 2 (NF2), inherited as anautosomal dominant condition (see Chapter 6).hydrocephalus.

Clinical presentationThe presenting features will depend on the sizeof the tumour at the time of diagnosis. The earliersymptoms are associated with 8th nerve involvement. Tinnitus and unilateral partial or completesensorineural hearing loss are the earliest features.Episodes of vertigo may occur but thesemay be difficult to distinguish from Menière’sdisease.

Although the tumour causes compressionof the facial nerve, the growth of the tumouris so slow that facial paresis is not evident untilthe tumour is large. At that stage 5th nerve compressionmay be evident, with diminished facialsensation and a depressed corneal reflex. Cerebellarinvolvement will result in ataxia, andcompression of the pyramidal tracts from a verylarge tumour causing brainstem compressionwill cause a contralateral hemiparesis. If a largetumour has caused obstructive hydrocephalusthe patient will also present with features ofraised intracranial pressure

Radiological investigations
The CT scan or MRI will show an enhancing tumourextending from the internal auditory canalinto the cerebellopontine angle (Fig. 7.13). The internalauditory meatus will be widened indicatingthat the tumour has arisen from the 8thcranial nerve (Fig. 7.14). While there is no difficultyin diagnosing a tumour large enough to beevident on the CT scan, very small acousticneuromas, which are predominantly within theinternal auditory canal, may be more difficult todiagnose. These tumours may be seen on highqualityCT scan but are particularly evidentusing MRI, especially following gadolinium contrast
(Fig. 7.15 ,)which is now the investigation ofchoice.

Other investigations
Pure tone audiometry, by both air and bone conduction,is an essential part of the investigation ofa patient with an acoustic neuroma, the mostcommon finding being high-frequency hearingloss. Other special auditory tests include the useof brainstem auditory evoked responses whichare particularly sensitive for changes in the retrocochlearauditory system; these are helpful indiagnosing a small intracanalicular tumour.Vestibular function is impaired early in

Fig. 7.13 Acoustic neuroma. Acontrast-enhancingtumour in the cerebellopontine angle arising from the8th cranial nerve in the internal auditory canal.

Fig. 7.14 Widened internal auditory meatus,indicative of an acoustic neuroma

patients with acoustic neuroma. The Hallpikecaloric test is carried out with the patient supineon a couch and the head raised to 30°C abovehorizontal, bringing the horizontal canals intothe vertical plane with the position of maximumsensitivity to thermal stimuli. Warm and coolwater is irrigated and the nystagmus reactionobserved. The caloric response on the side of theacoustic nerve tumour is depressed or absent

Differential diagnosis
The major differential diagnoses for a cerebello-pontine angle tumour, in decreasing frequency,are:
•meningioma •metastatic tumour
•exophytic brainstem glioma •epidermoid tumour.

Treatment
The total excision of a large acoustic neuromaremains one of the major operative challengesin what Cushing has described as ‘the gloomycorner of neurologic surgery.’
The aim of the operation is complete resectionof the tumour while sparing the adjacent neuralstructures. If the patient presents with a large tumourcausing severe hydrocephalus and raisedintracranial pressure, a preliminary ventriculoperitonealshunt or ventricular drain may beconsidered.

Steroid administration prior tosurgery may be advisable if the tumour is large.There are three basic approaches to the cerebellopontineangle: by excision of the labyrinth
(translabyrinthine ;)through a posterior fossacraniectomy (suboccipital/retrosigmoid); or viathe middle cranial fossa.

No clear consensus has emerged from the literatureas to which is the procedure of choice.There are definite advantages and disadvantagesassociated with each surgical approach. Theroute chosen is governed by tumour size, thedegree of hearing loss, the hearing level inthe contralateral ear, and the surgical preferenceand expertise of the operator.

The major advantage of the translabyrinthineoperation is that the facial nerve can be identifiedlateral to the tumour at an early stage in the dissection,and access to the fundus of the internalauditory meatus is excellent. Furthermore, retractionof the cerebellum is minimal and the riskof postoperative oedema is consequently less.

The major disadvantage of this route is thatresidual hearing is irrevocably destroyed. Theapproach is unfamiliar to neurosurgeons, andrequires the close cooperation of a neurotologistexperienced in dissection of the temporal bone.Access is confined, but even the largest of tumourscan be removed safely via this approach.

As a consequence of progressive improvementsin operative results, particularly in mortalityand facial nerve outcome, attention hasturned more recently to the ability to preserveuseful hearing. The suboccipital operation providesgood access to the cerebellopontine anglebut, if hearing is to be conserved, tumour at thefundus of the internal auditory meatus may bedifficult to expose under direct vision.

This is trueparticularly when the posterior semicircularcanal is medially placed. Theoretically, this mayincrease the risk of subtotal tumour excisionwhen compared with the translabyrinthine operation.Recently there has been renewed interestin the middle fossa approach for removal ofintracanalicular tumours or those with a smallcerebellopontine angle component, particularlywhere the tumour in the internal auditory canalextends to the fundus.

Higher rates of hearingpreservation have been reported without anycompromise of facial nerve function, but thisroute provides more limited access to the cerebellopontineangle, and is therefore restricted to thetreatment of small lesions.The question of hearing conservation deservescareful consideration when selecting the surgicalapproach.

Anatomical preservation of the innerear and cochlear nerve does not guarantee function,and it is exceptional for hearing to be improvedbeyond its preoperative level. Whethersuch hearing is useful depends upon the level ofhearing in the contralateral ear. Hearing lossneed not be profound before it is socially uselesswhen the other ear is normal.

For hearing to beuseful socially there must be both good speechdiscrimination, and a pure tone audiogram within
20–40 dB of the contralateral ear. It is alsoessential that the attempt to preserve hearingshould not compromise the likelihood of completetumour removal.

At The Royal Melbourne Hospital thetranslabyrinthine operation is favoured for largetumours, regardless of hearing level, and formedium-sized lesions with poor hearing. It providesa more direct approach to the cerebellopontineangle, and retraction of the cerebellum isnegligible. For hearing preservation the retrosigmoidapproach for tumours with up to 2 cm cerebellopontine

cerebellopontineangle extension is preferred. Themiddle fossa approach is preferred for intracanaliculartumours and for those with up to
1 cm cerebellopontine angle extension where tumourcompletely fills the internal auditory canal.Stereotactic radiosurgery using either a 60COGamma Knife or a highly focused linear acceleratorhas been advocated for the treatment ofsmaller tumours, less than 3 cm in diameter.

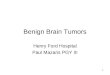
Fig. 7.15 (a) MRI showing small intracanalicularmeningioma. (b) MRI showing large acoustic neuromainvading into temporal bone and extending intocerebellopontine angle with severe compression of thebrainstem.

Thecontrol rates are greater than 90% over a 5-yearperiod, but post-radiation neurological complicationshave been reported including delayedfacial numbness and dysaesthesia, facial weaknessand hearing loss. To minimize the complicationsof single-dose stereotactic radiosurgerymany centres advocate fractionated stereotacticradiotherapy.

There is continuing debate as to the relativeadvantages of surgery and stereotactic radiationtreatment. Whilst some clinicians advocate radiationtreatment for smaller tumours, others wouldonly recommend it for elderly or medicallyinfirm patients or if there is residual tumour orregrowth after subtotal resection.

The management plan for patients with bilateralacoustic neuromas (NF2) is complex, andmust be tailored for each patient, with the aim ofpreserving useful hearing for as long as possible,whilst minimizing the possible serious neurologicalcomplications from enlarging tumourscausing cranial nerve, cerebellar and brainstemcompression. Therapeutic options includesurgery, radiosurgery and hearing preservations/
restoration utilizing brainstem electrodeimplants at the time of tumour resection.

Postoperative care
The postoperative management is similar to thatindicated for the posterior fossa tumours in theprevious chapter. Any neurological deteriorationmust be investigated urgently. A postoperativehaemorrhage in this region may be rapidly fatal.Postoperative swallowing difficulties mayoccur if there has been injury to the lower cranialnerves or brainstem.

Great care should be takento avoid aspiration and nasogastric feeding maybe necessary. Facial paralysis will occur if the 7thnerve is not intact at the end of the operation andmay result even if the nerve is in continuity dueto neuropraxia of the nerve. Atarsorrhaphy maybe necessary to prevent corneal ulceration andwill be essential if there is a facial palsy andcorneal sensation is diminished due to 5th nervedamage.

damage. Alternatively temporary closure of theeye can be obtained by using botulinum toxin.The cosmetic appearance of a permanentfacial paralysis can be improved by a number ofprocedures including:
•nerve anastomoses, such as a hypoglossal–facial anastomosis
•cross-facial nerve grafts •facial slings.

Haemangioblastoma
Haemangioblastomas are uncommon intracranialtumours accounting for 1–2% of all braintumours and approximately 10% of posteriorfossa tumours.The haemangioblastoma arises from proliferationof endothelial cells. The tumour usually occursin young adults, although it may occur atany age. It usually occurs in the posterior fossaand often produces a large cyst.

Although haemangioblastomamay occur as a component ofvon Hippel–Lindau’s disease, which includesmultiple haemangioblastomas, haemangioblastomasof the retina (von Hippel tumour), renaltumour, renal cyst, pancreatic cyst and tubularadenomata of the epididymis, the majority ofpatients with the cerebellar tumour do not havevon Hippel–Lindau’s disease. Incomplete formsof the syndrome may occur and cerebellar haemangioblastomasoccur in about 20% of patientswith retinal haemangioblastoma.

Clinical presentation
The tumour presents as a slowly growingposterior fossa mass with features of raisedintracranial pressure and cerebellar involvement.Occasionally the patient may be polycythaemicdue to increased circulating erythropoietin.Radiological investigationsCT scan or MRI show a cerebellar tumour whichmay involve the vermis and hemispheres andwhich shows vivid enhancement following intravenouscontrast (Fig. 7.16). There is usuall

There is usually alow-density cyst surrounding the tumour nodule
(Fig. 7.17 ,)although haemangioblastomas maysometimes be solid. If considered necessary,vertebral angiography will confirm the highlyvascular mass.Total surgical excision through a posteriorfossa craniotomy is nearly always possible. Greatcare must be taken not to enter the highly vasculartumour during the dissection and excision.

Fig. 7.17 MRI. Cystic haemangioblastoma.

Colloid cyst of the 3rd ventricle
The colloid cyst of the 3rd ventricle is situated inthe anterior part of the ventricle and is attachedto the roof just behind the foramen of Monro.Several possibilities as to the origin of thetumour have been proposed, including the paraphysis,choroid plexus epithelium, ependymaor a diverticulum of the diencephalon.

The cyst consists of a thin, outer fibrous capsulelined by a layer of epithelium; the contentsconsist of mucoid material, epithelial debris andmucin. The cyst may be very small and asymptomatic,as was the case with Harvey Cushing,where a 1-cm colloid cyst was found at postmortem.As the tumour grows it will causebilateral obstruction to the foramina of Monro,leading to raised intracranial pressure from hydrocephalus.

The headaches may fluctuate,being aggravated by stooping and relieved bystanding upright. Episodes of abrupt, suddenleg weakness causing the patient to fall mayoccur without a change in conscious state.Alternatively, an abrupt loss of consciousnessmay occur and this, although usually transient,might be fatal.

Radiological investigationsThe usual CT scan picture is a high-density,rounded tumour in the anterior 3rd ventriclewhich enhances following intravenous contrast
(Fig. 7.18 ,)although isodense, hypodense andnon-enhancing tumours have been reported.MRI helps to define the position of these tumours
(Fig. 7.18 )and will be able to differentiatebetween a colloid cyst and an aneurysm ofthe basilar tip, which may occasionally beindistinguishable on CT scan

Treatment
Surgical excision is performed through a craniotomywith a small incision in the anteriorcorpus callosum giving access to the lateralventricle. The tumour is seen expanding the foramenof Monro and, using the operating microscope,a complete excision is usually possible.Great care must be taken during the operation topreserve the venous structures, including theseptal veins, thalamostriate vein and internalcerebral veins. Damage to the columns of thefornix will result in severe postoperativememory disturbance.cerebral veins.

Epidermoid and dermoid cysts
Epidermoid and dermoid cysts arise fromepithelial cells embryologically misplaced intracranially,particularly into the meninges andventricles and, less frequently, into the parenchymaof the brain. Rarely, the cells can be implantedas a result of trauma such as a lumbarpuncture, which can implant skin into the spinalcanal causing an epidermoid cyst.

Epidermoid cysts make up about 1% of braintumours, although their incidence is higher inJapan, where the incidence of dermoid cysts ismuch less.Epidermoid tumours are found principally inthe arachnoid spaces, the cisterns or the diploeof the bone.

The most frequent localizations arethe cerebellopontine angle, the suprasellar andparasellar regions, the lateral or 4th ventricles,and the quadrigeminal cisternDermoid tumours occur mostly in theposterior fossa as a midline lesion and a fistulamay connect the dermoid with the skin.

Fig. 7.18 Colloid cyst of the 3rd ventricle. (a) CT scanshows hyperdense tumour before contrast. (b) MRI.Colloid cyst. (c) MRI. Colloid cyst sagittal view.

Fig. 7.19 (a) Dermoid cyst. Avery low density lesionon CT scan that does not enhance. (b) MRI.Epidermoid cyst adjacent to brainstem.

HistologyThe epidermoid cyst contains desquamatedepithelium surrounded by keratin-producingsquamous epithelium. The dermoid cyst includesdermal elements such as hair follicles,sebaceous glands and sometimes sweat glands

Clinical presentationThe cysts usually present following a long historyof symptoms related to their position.Cranial nerve abnormalities such as trigeminalneuralgia and hemifacial spasm may occur withcerebellopontine angle epidermoid tumours andthe suprasellar cyst will produce visual impairmentwith optic atrophy and often a bitemporalhemianopia. Leakage of epidermoid cyst contentsmay result in a chemical meningitis, and inpatients with posterior fossa dermoid cysts,bacterial meningitis may occur through thedermal sinus connecting the cyst with the skin

Radiological investigationsThe CT scan of an epidermoid cyst is characterizedby a low-density lesion that does notenhance. The dermoid cyst will also have areaswhich are even less dense than CSF, indicatingthe presence of fat (Fig. 7.19). MRI has supercededCT for accurate preoperative evaluationand planning. Epidermoid lesions are usuallymanifest as low signal on T1 and high signal on T2images, although depending on lipid content,variable signal intensities may be seen within thesame lesion.

TreatmentThe treatment is operative, with resection of thecyst. Complete excision may be prevented if thecyst wall is densely adherent to major vessels andimportant neural structures.