Embed Size (px)
Citation preview
FIRAS BCC
Basal cell carcinoma
Dr. firas kassab
FIRAS BCC
Basal cell carcinoma is a slow-growing form of skin cancer.
Skin cancer falls into two major groups: Nonmelanoma and melanoma.
Basal cell carcinoma is a type of nonmelanoma skin cancer
FIRAS BCC
Basics of BCC
Background Most common cutaneous malignancy (~80-90%) Typically slow-growing, rarely metastasizes Sun-exposed skin, mostly face and scalp, esp
nose, cheek, and periorbital regions (~80%)Frequency
900,000 Dx in US/year estimated lifetime risk of 33-39% for
men and 23-28% for womenSex
Men 2X over women
FIRAS BCC
Basics of BCC
Mortality/Morbidity <0.1% metastasize Very low mortality Significant morbidity with direct invasion of
adjacent tissues, especially when on face or near an eye
Age Likelihood increases with age Rare in <40 yo
Race Most often in light-skinned, rare in dark-skinned
races
FIRAS BCC
Classification
according to
AppearanceHistological
FIRAS BCC
Appearance
we can divide basal-cell carcinoma into 3 groups, based on location and difficulty of therapy:
1. . Superficial basal-cell carcinoma :is very responsive to topical chemotherapy such as .It is the only type that can be effectively treated with topical chemotherapy.
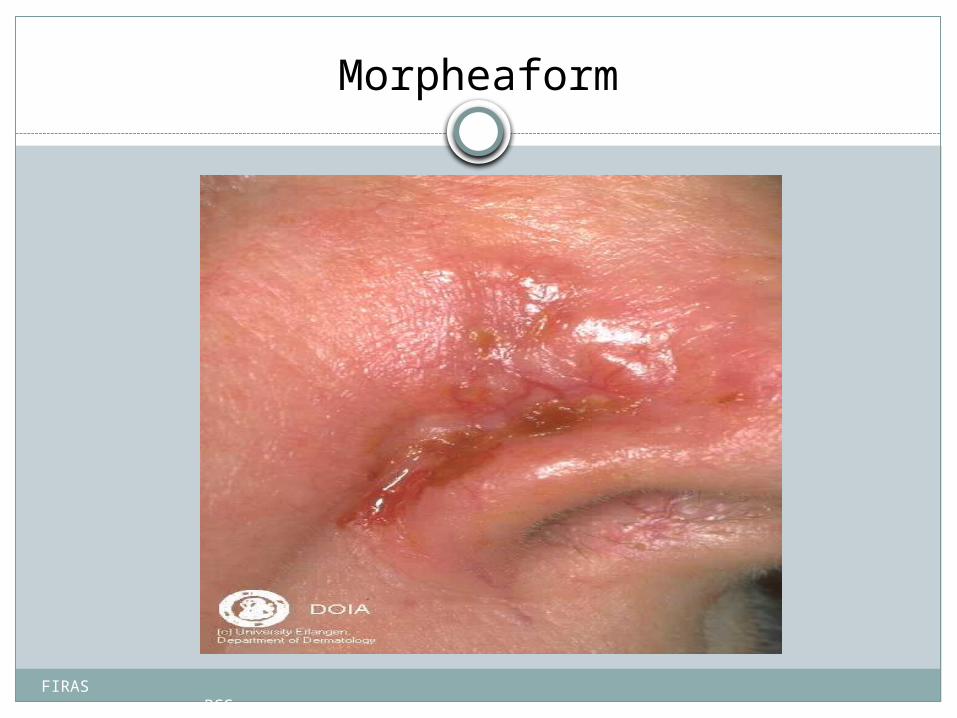
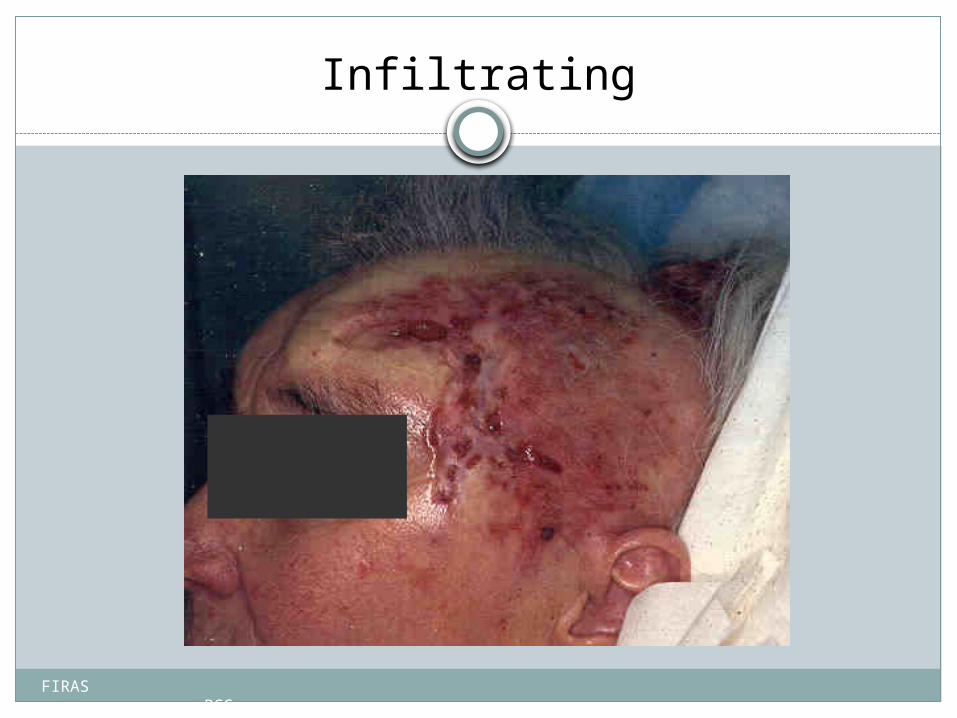
2. Infiltrative basal-cell carcinoma: which often encompasses morpheaform and micronodular basal-cell cance. More difficult to treat with conservative treatment methods such as electrodessiccation and curettage, or with curettage alone.
3. Nodular basal-cell carcinoma: which essentially includes most of the remaining categories of basal-cell cancer. It is not unusual to encounter morphologic features of several variants of basal-cell cancer in the same tumor.
FIRAS BCC
Histological
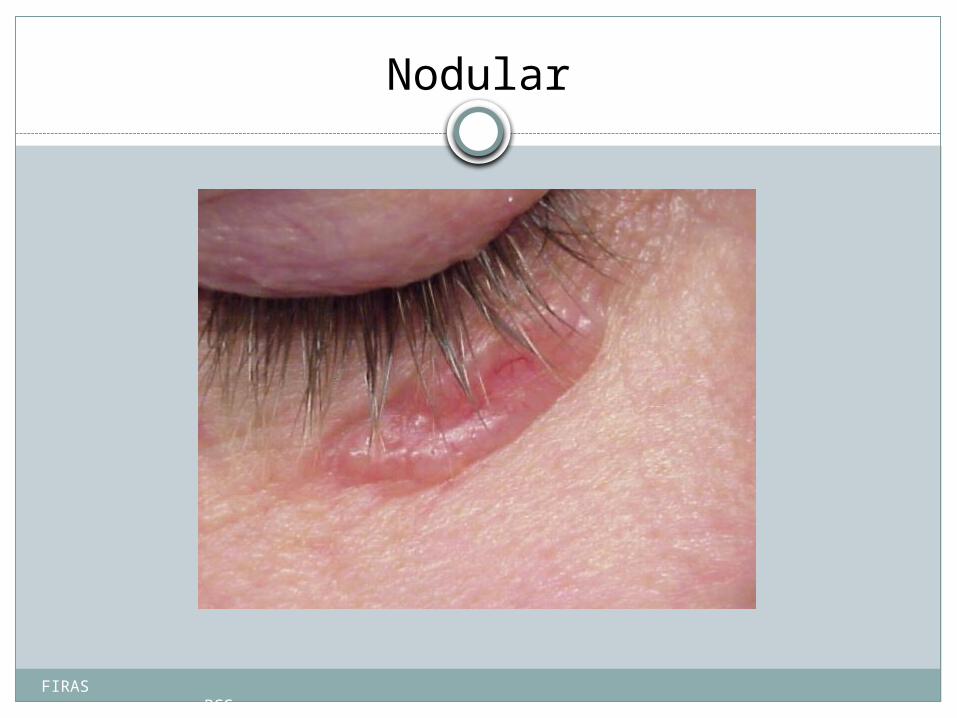
Basal-cell carcinomas may be divided into the following types: Nodular basal-cell carcinoma is a subtype of basal-cell carcinoma, most
commonly occurring on the sun-exposed areas of the head and neck.[
Cystic basal-cell carcinoma is characterized by dome-shaped, blue-gray cystic nodules.
Cicatricial basal-cell carcinoma is an aggressive variant with a distinct clinical and histologic appearance.
Infiltrative basal-cell carcinoma is an aggressive type of basal-cell carcinoma characterized by deep infiltration.
Micronodular basal-cell carcinoma is characterized by a micronodular growth pattern.
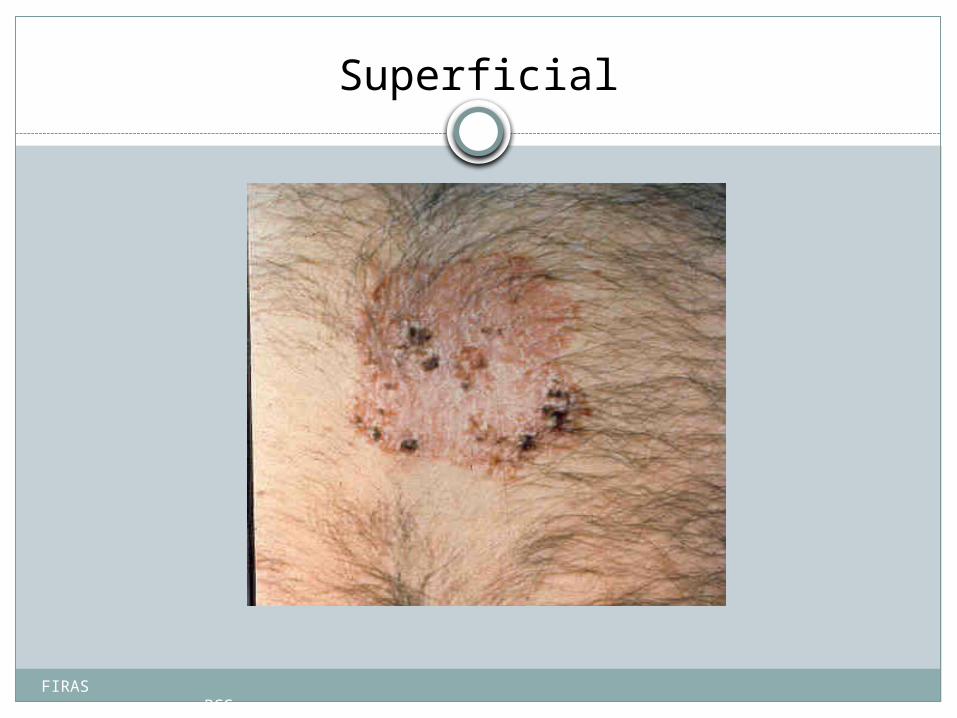
Superficial basal-cell carcinoma that occurs most commonly on the trunk and appears as an erythematous patch.
FIRAS BCC
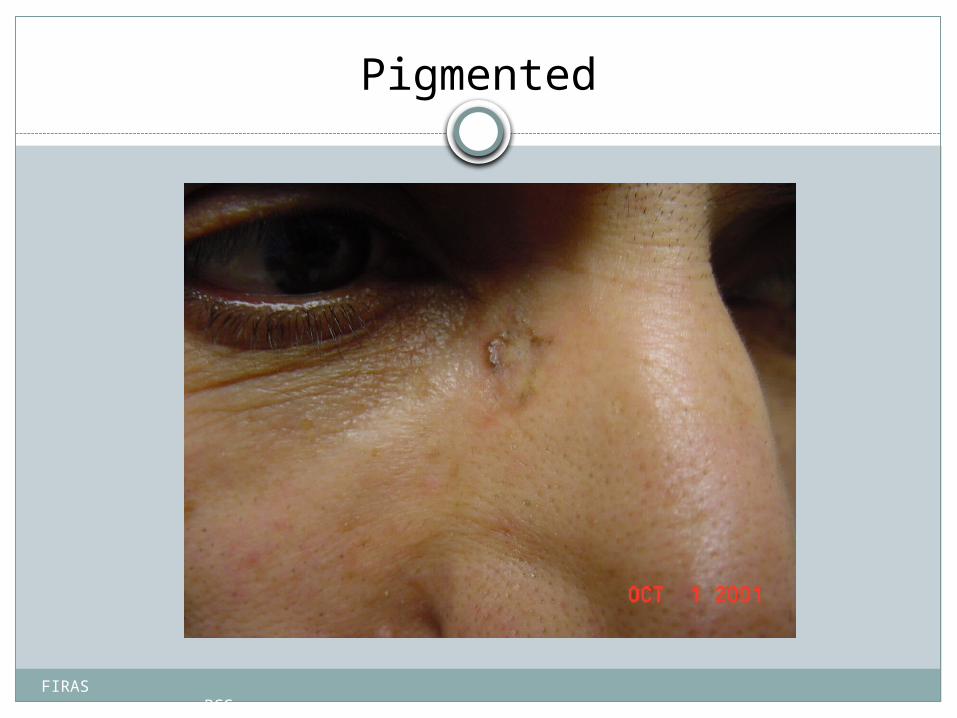
Pigmented basal-cell carcinoma that exhibits increased melanization.About 80% of all basal cell carcinoma in chinese are pigmented while this subtype is uncommon in white people.
Rodent ulcer is a large skin lesionof nodular basal cell carcinoma with central necrosis
Fibroepithelioma of pinkus most commonly occurring on the lower back.
Polypoid basal-cell carcinoma is characterized by exophytic nodules (polyp-like structures) on the head and neck.
Pore-like basal-cell carcinoma is characterized by a basal-cell carcinoma that resembles an enlarged pore or stellate pit.
Aberrant basal-cell carcinoma is characterized by the formation of basal-cell carcinoma in the absence of any apparent carcinogenic factor, occurring in odd sites such as scrotum, vulva, perineum, nipple, and axilla.
FIRAS BCC
See also:Nevoid basal cell carcinoma syndromCystic basal-cell carcinomaMicronodular basal cell carcinomaSuperficial basal cell carcinomaMicrograph of a fibroepithelioma of Pinkus.
FIRAS BCC
Variants of Basal Cell Carcinoma
Superficial Nodular Micronodular Infiltrating (5%) Sclerosing/ morpheaform (5%) Metatypical Infundibulocystic Nodulocystic Adenoid Clear cell Follicular Sebaceous Perineurally invasive
FIRAS BCC
Nodular
FIRAS BCC
Superficial
FIRAS BCC
Morpheaform
FIRAS BCC
Pigmented
FIRAS BCC
Infiltrating
FIRAS BCC
Differential Diagnosis
Malignant melanomaSquamous cell carcinomaBasal cell carcinoma, infiltrativeInfectious
FIRAS BCC
Causes, incidence, and risk factors:
Basal cell carcinoma starts in the top layer of the skin called the epidermis. Most basal cell cancers occur on skin that is regularly exposed to sunlight or other ultraviolet radiation. This includes the top of your head, or scalp.
Basal cell skin cancer is most common in people over age 40. However, it occurs in younger people, too.
FIRAS BCC
You are more likely to get basal cell skin cancer if you have:Light-colored or freckled skinBlue, green, or grey eyesBlond or red hairOverexposure to x-rays or other forms of radiationMany molesClose relatives who have or had skin cancerMany severe sunburns early in lifeLong-term daily sun exposure (such as the sun exposure people who
work outside receive)
FIRAS BCC
Sings and Symptoms:
Basal cell skin cancer grows slowly and is usually painless. It may not look that different from normal skin.
patient may have a skin bump or growth that is:Pearly or waxyWhite or light pinkFlesh-colored or brownIn
some cases the skin may be just slightly raised or even flat.
FIRAS BCC
patient may have:A skin sore that bleeds easilyA sore that does not healOozing or crusting spots in a soreA scar-like sore without having injured the
areaIrregular blood vessels in or around the spotA sore with a depressed (sunken) area in the
middle
FIRAS BCC
Diagnosis:
doctor should check the skin and look at the size, shape, color, and texture of any suspicious areas.
If the patient might has skin cancer, a piece of skin will be removed and sent to a lab for examination under a microscope. This is called a skin biopsy. There are different types of skin biopsies.
FIRAS BCC
The most common method is a shave biopsy under locale anesthesia.
Most nodular basal-cell cancers can be diagnosed clinically; however, other variants can be very difficult to distinguish from benign lesions such as:
intradermal naevussebaceomasFibrous papulesearly acnes scarsand hypertrophing scarring.
FIRAS BCC
Treatment Options
Electrodessication and curettageCurettage aloneSurgical excisionMohs micrographically controlled surgeryCryosurgeryIonizing radiationSurgical excision plus radiationExenteration
FIRAS BCC
Treatment depends on the sizedepth location of the skin canceroverall health.
Treatment
FIRAS BCC
may involve:Excision: Cutting out the skin cancer and stitching the skin
togetherCurettage and electrodesiccation: Scraping away cancer cells
and using electricity to kill any that remainCryosurgery: Freezing the cancer cells, which kills themMedication: Skin creams containing imiquimod or 5-
fluorouracil for superficial (not very deep) basal cell cancer
Treatment
FIRAS BCC
Treatment
Mohs surgery: Removing a layer of skin and looking at it immediately under a microscope, then removing many layers of skin until there are no signs of the cancer; usually used for skin cancers on the nose, ears, and other areas of the face.
Photodynamic therapy: Treatment using light Radiation may be used if a basal cell cancer cannot be treated
with surgery
FIRAS BCC
Is excellent How well a patient does depends on many
things, including how quickly the cancer was diagnosed. Most of these cancers are cured when treated early.
Some basal cell cancers may return. Smaller ones are less likely to come back.
Basal cell carcinoma almost never spreads to other parts of the body ,Because basal-cell carcinoma rarely metastasis, it grows locally with invasion and destruction of local tissues
prognosis
FIRAS BCC
Complications
Basal cell skin cancer almost never spreads. But, if left untreated, it may grow into surrounding areas and nearby tissues and bone. This is most worrisome around the nose, eyes, and ears.
FIRAS BCC
Prevention
The best way to prevent skin cancer is to reduce exposure to sunlight.
Ultraviolet light is most intense between 10 a.m. and 4 p.m., so try to avoid sun exposure during these hours.
Protect the skin by wearing hats, long-sleeved shirts, long skirts, or pants.
Always use sunscreen
FIRAS BCC
Conclusion
Basal cell carcinomas are not always as innocent as we tend to believe
In formulating treatment course: Strong pt preference and
other pt factors Current research