Embed Size (px)
Citation preview

b-card symposium
Cardiac Arrest in the Field TodayU A Goes Beyond ACLS
TuesdayMarch 7th
2017
Nicolas PESCHANSKI, MD, PhD
Acknowledgments
Salim R. Rezaie, MD@srrezaie
Tom R. Bouthillet, EMT@tbouthillet

Cardiac Arrest in the Field
USA
2016
STATE
of
the
UNION
Principles for EMS in the Field
Immediate Recognition & EMS Activation (911)
Early CPR w/ Emphasis on Chest Compressions
Rapid Defib’
Effective ACLS
Integrated Post-Resus Care
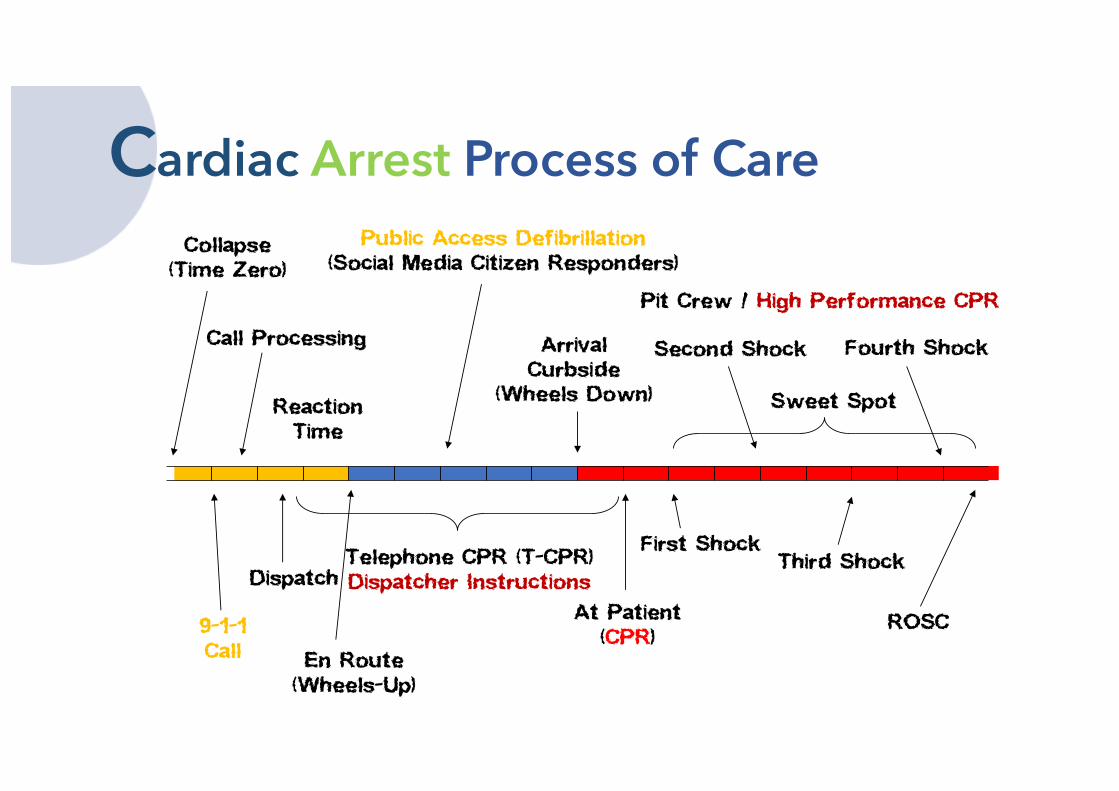
Cardiac Arrest Process of Care
Call Processing
Collapse(Time Zero)
ReactionTime
Pit Crew / High Performance CPR
Public Access Defibrillation(Social Media Citizen Responders)
9-1-1Call
Dispatch
En Route(Wheels-Up)
At Patient(CPR)
First Shock
ArrivalCurbside
(Wheels Down)
Second Shock
Third Shock
Fourth Shock
Sweet Spot
Telephone CPR (T-CPR)Dispatcher Instructions
ROSC
“It isn’t complicated
but it’s not easy.”

Multidisciplinary
Approach
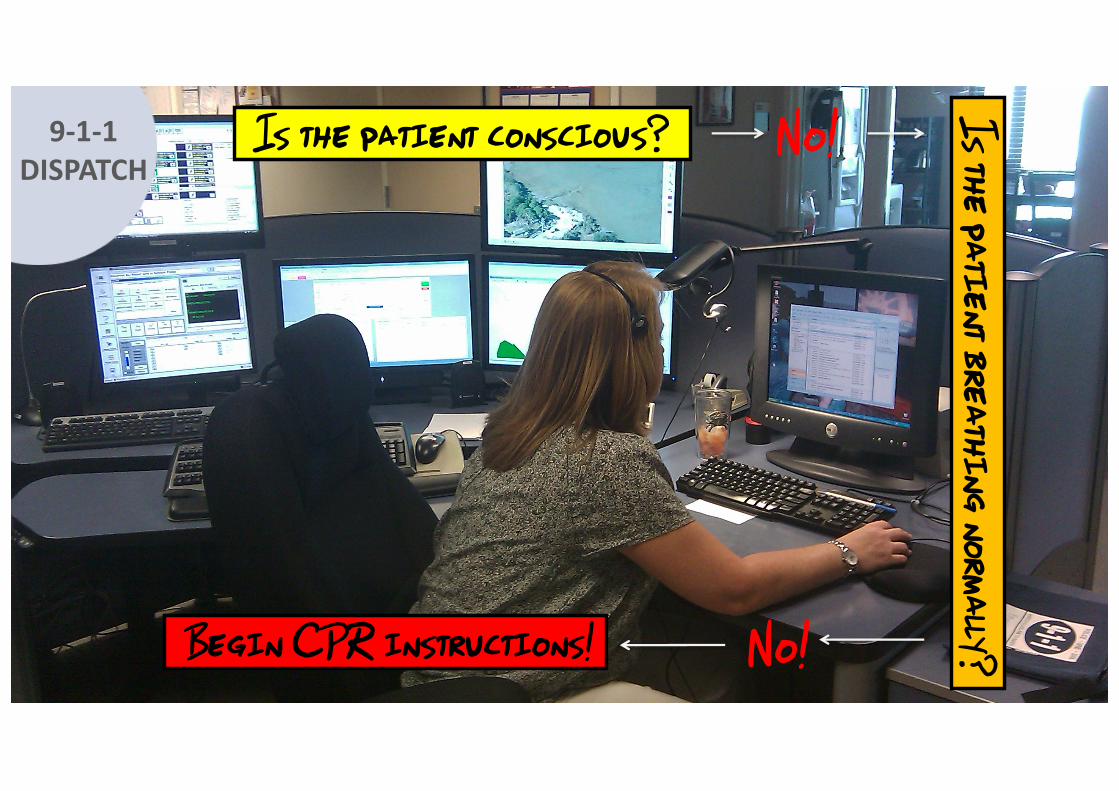
Is the patient conscious? Is the patient breathing normally?Begin CPR instructions!
No!
No!
9-1-1DISPATCH
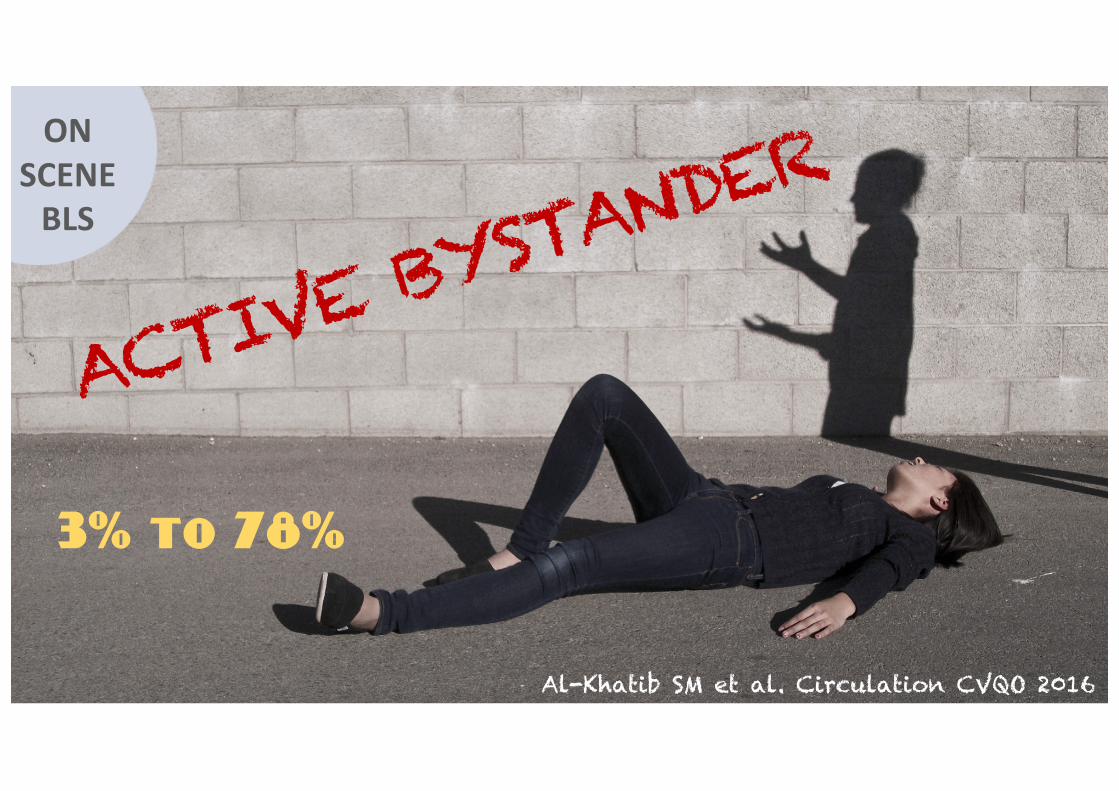
ONSCENEBLS
3% to 78%
Al-Khatib SM et al. Circulation CVQO 2016

ONSCENEBLS+
T-CPR & More
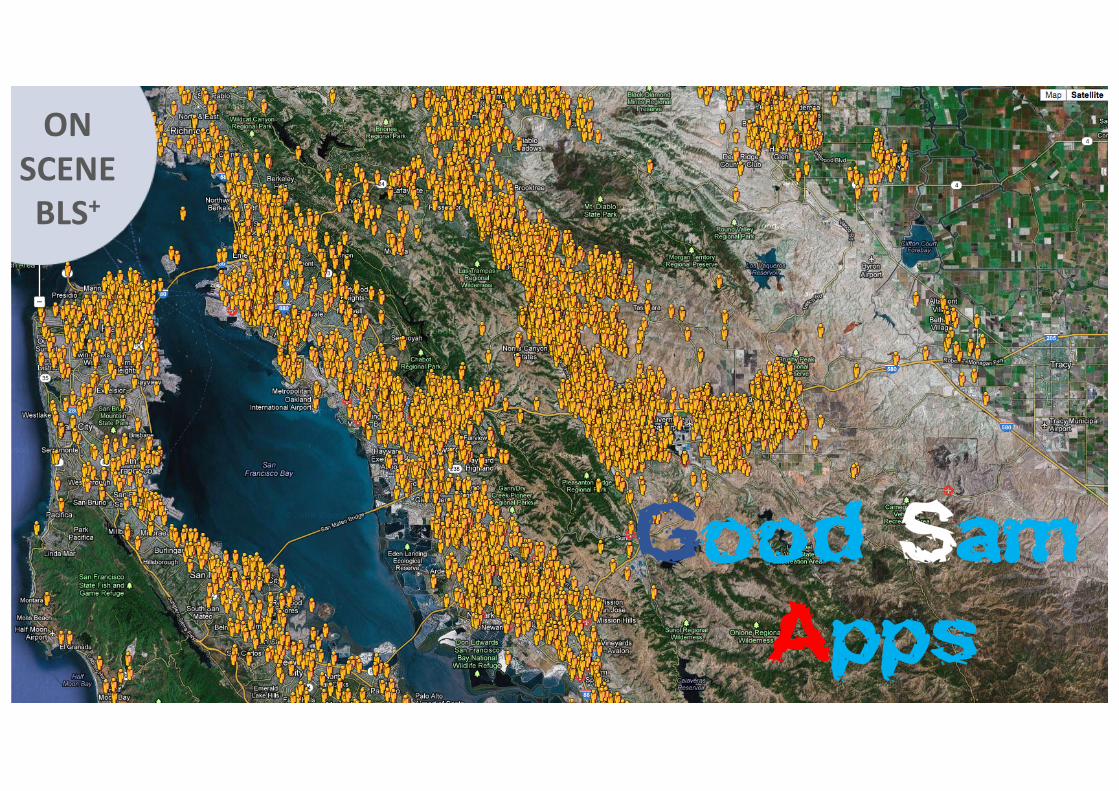
Good SamApps
ONSCENEBLS+

EMSTeamsACLS
Fire Dept Stations

CPREpiPulse
EMSFOCUS

CPR
EMSACLS

2015 AHA CPR
RATE100 – 120/min
DEPTH:2in - 2.4in
RECOILAllow Full Recoil
INTERRUPTIONSMinimize Pauses
RULES
Guideline Update

CPR: Man or Machine?
vs
EMSACLS+
Gates S et al. Resuscitation 2015
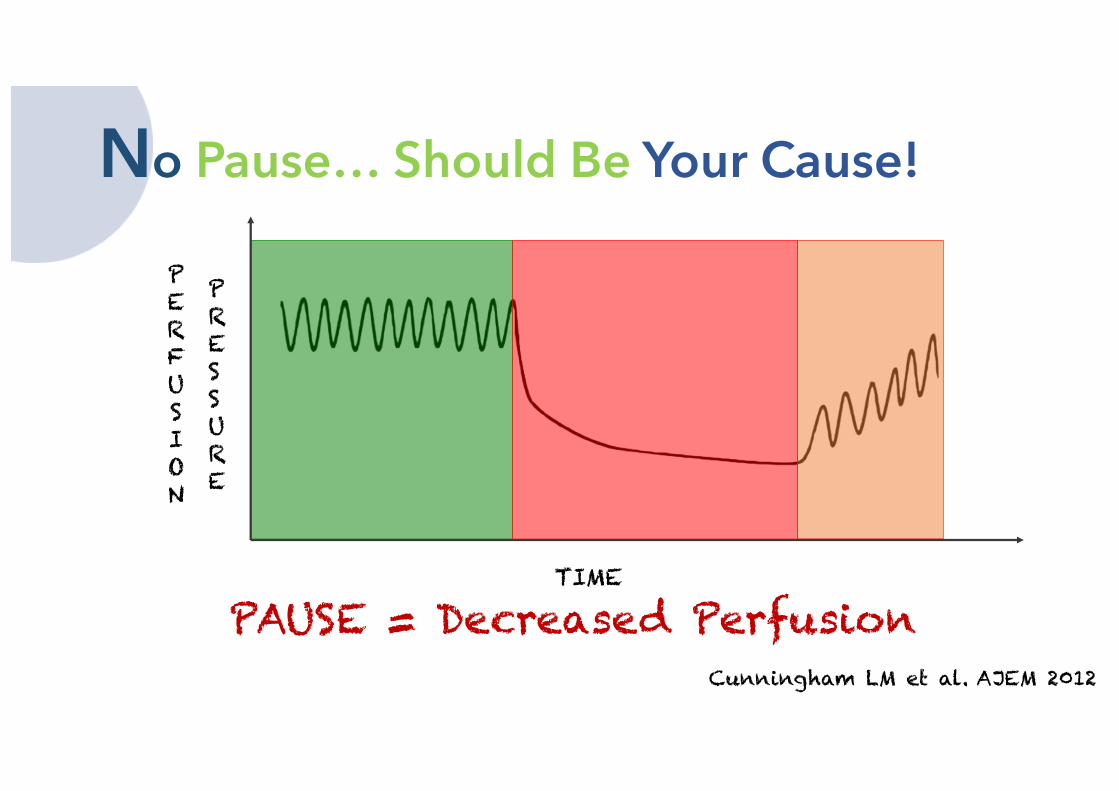
Cunningham LM et al. AJEM 2012
PAUSE = Decreased Perfusion
PERFUSION
PRESSURE
TIME
No Pause… Should Be Your Cause!
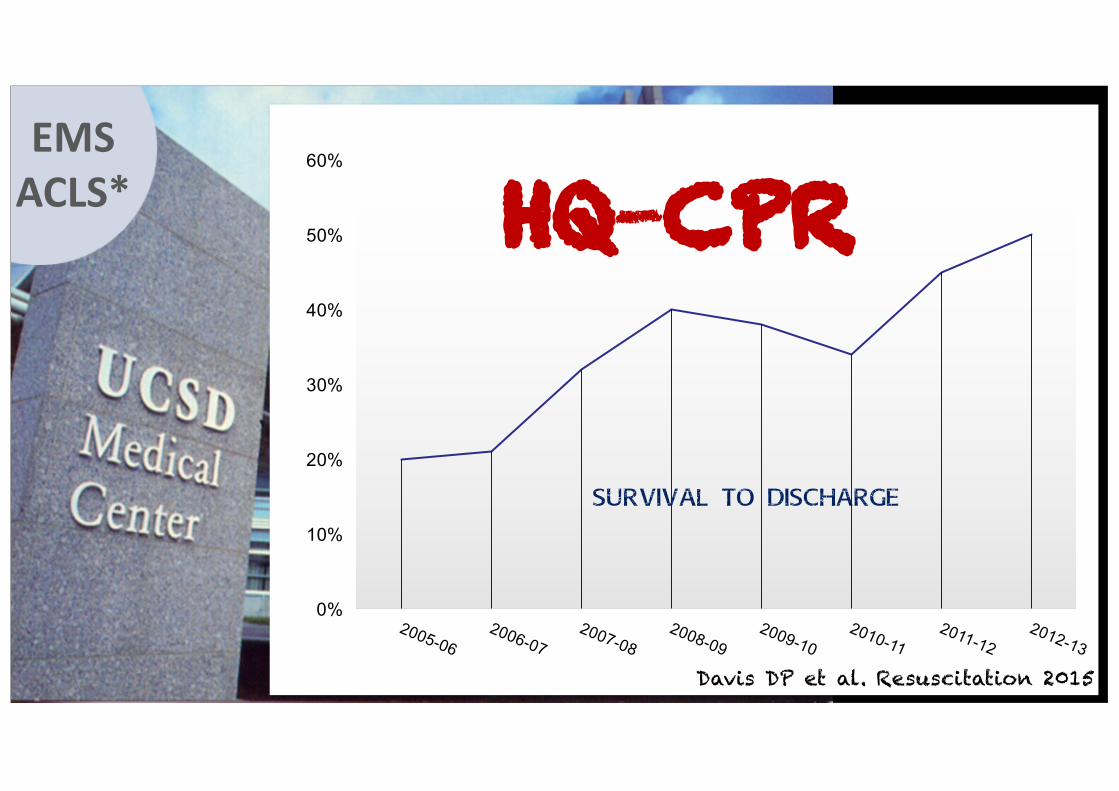
EMSACLS*
0%
10%
20%
30%
40%
50%
60%
Survival to Discharge
HQ-CPR
Davis DP et al. Resuscitation 2015
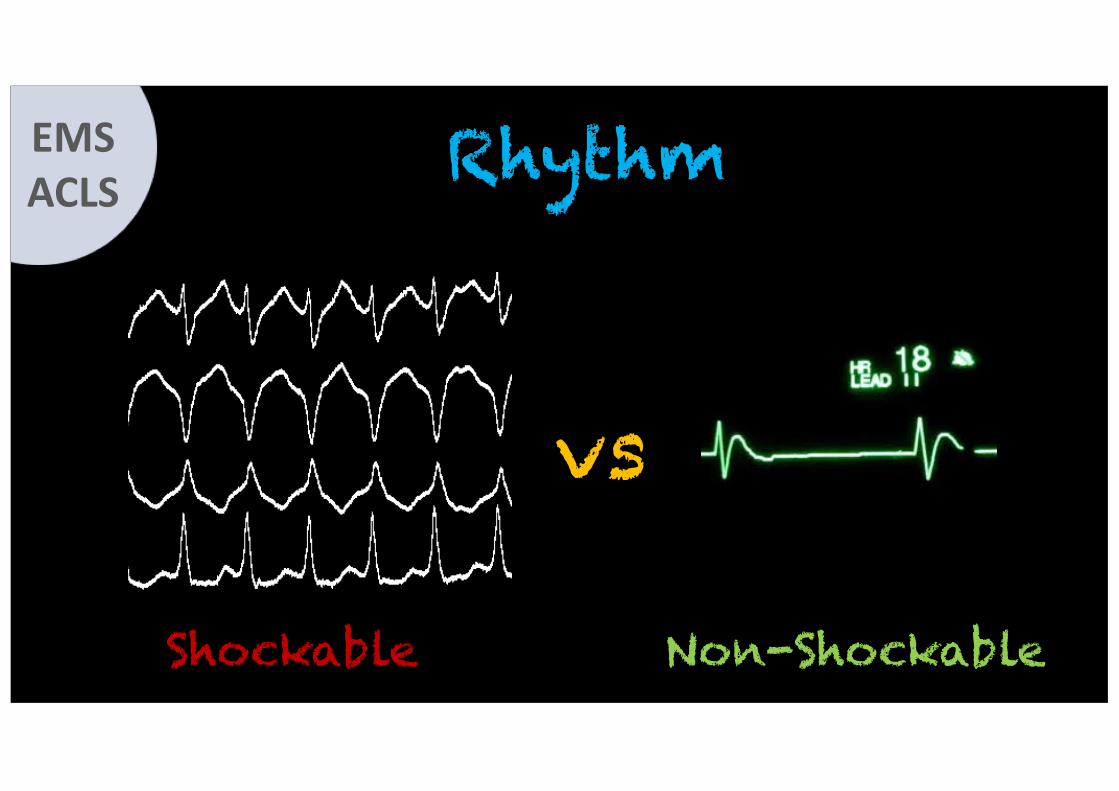
RhythmEMSACLS
vs
Shockable Non-Shockable

Early DefibrillationEMSACLS

PulseChecks
EMSACLS
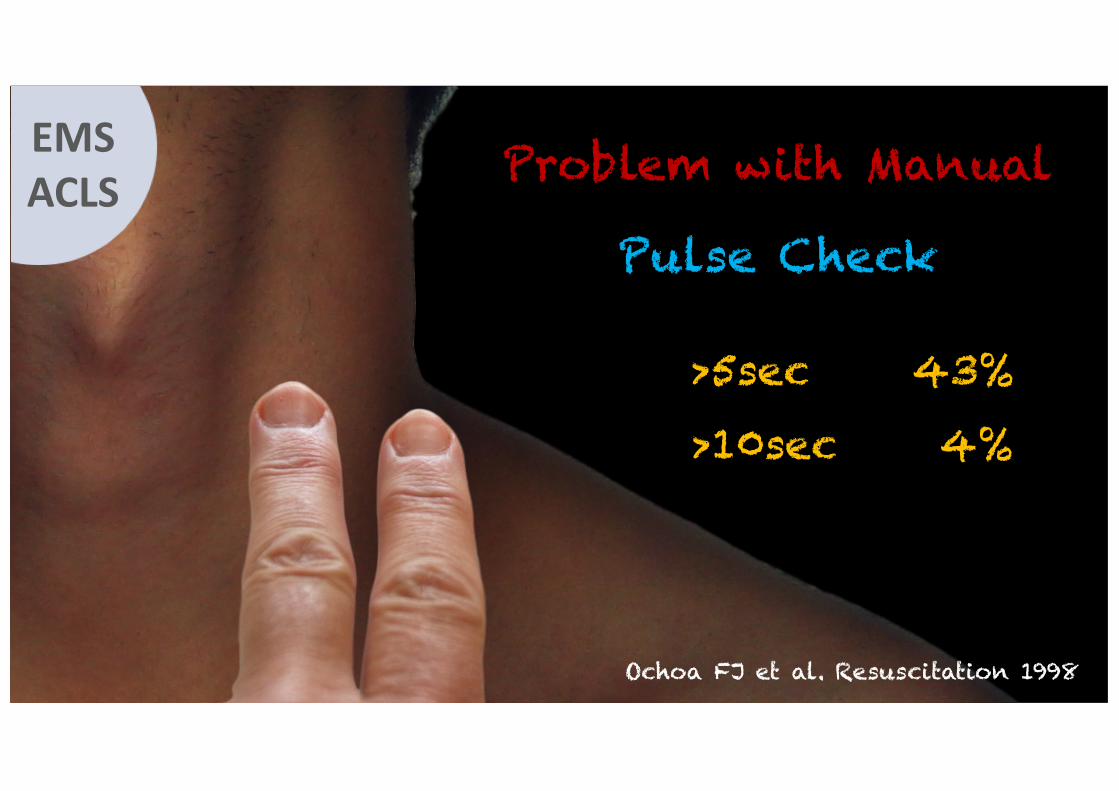
>5sec 43%
>10sec 4%
Ochoa FJ et al. Resuscitation 1998
Pulse Check
EMSACLS Problem with Manual
Is the Pulse Check Dead?EMSACLS
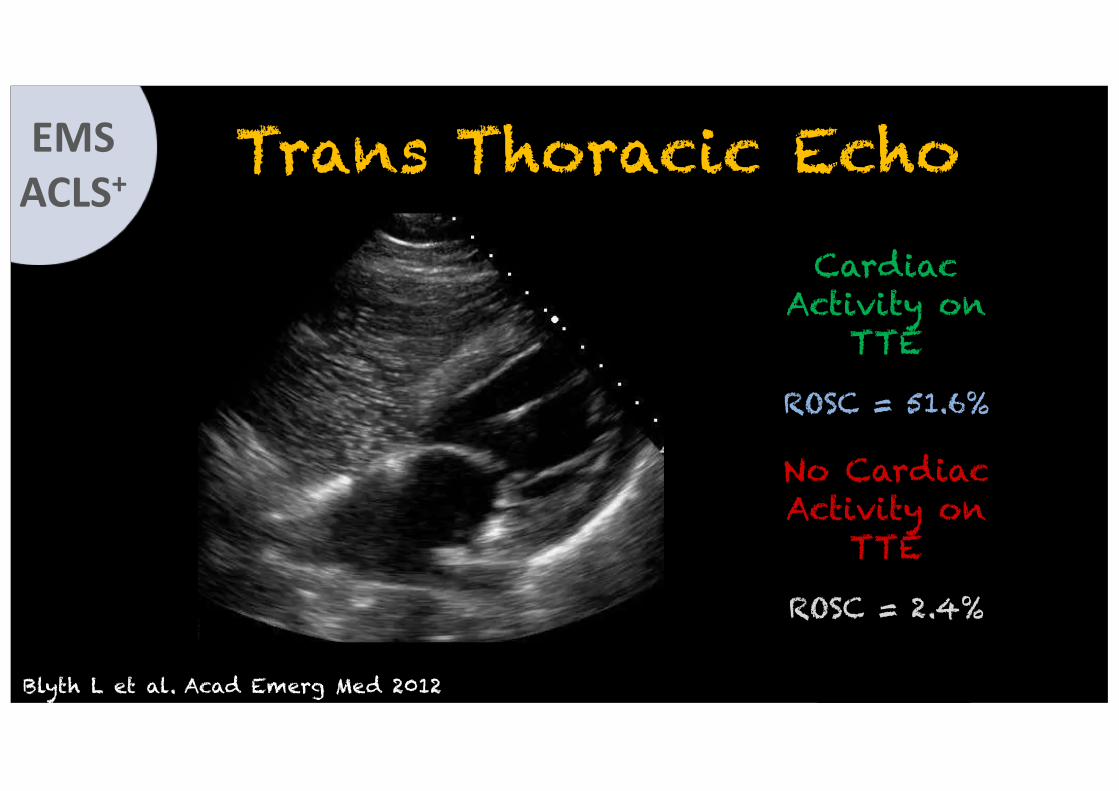
Trans Thoracic Echo
No Cardiac Activity on
TTE
ROSC = 2.4%
Cardiac Activity on
TTE
ROSC = 51.6%
Blyth L et al. Acad Emerg Med 2012
EMSACLS+
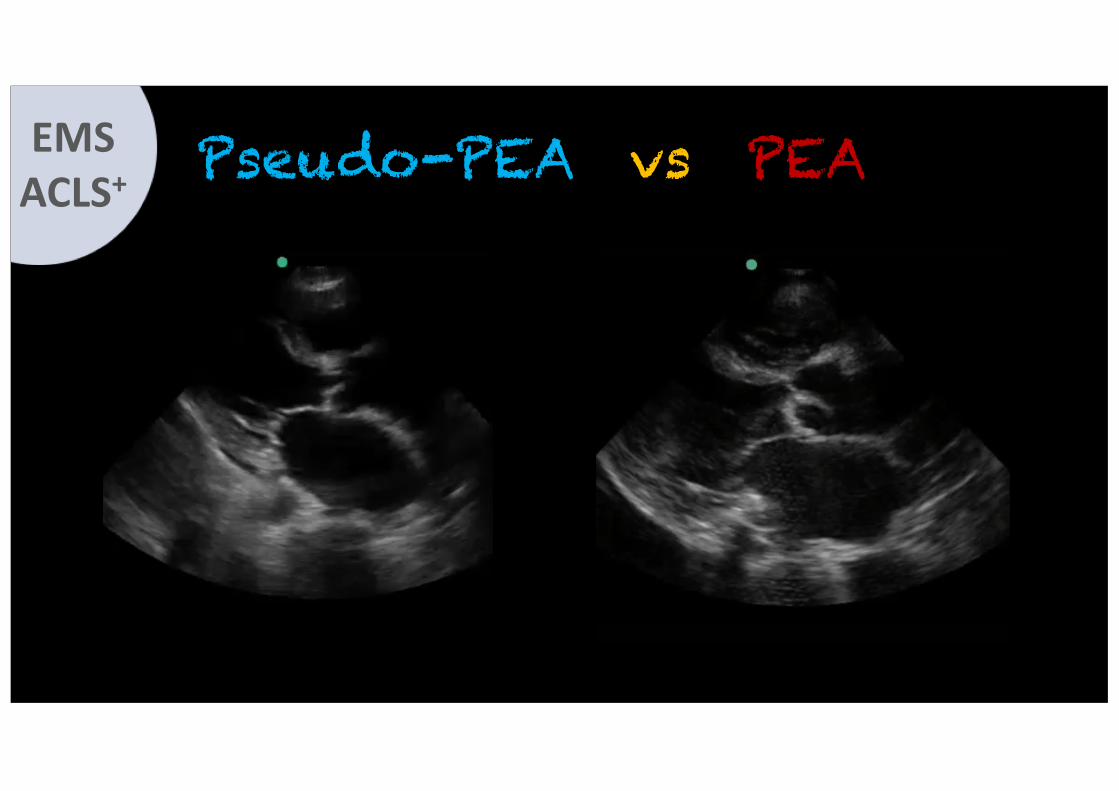
Pseudo-PEA vs PEAEMSACLS+
EMSACLS
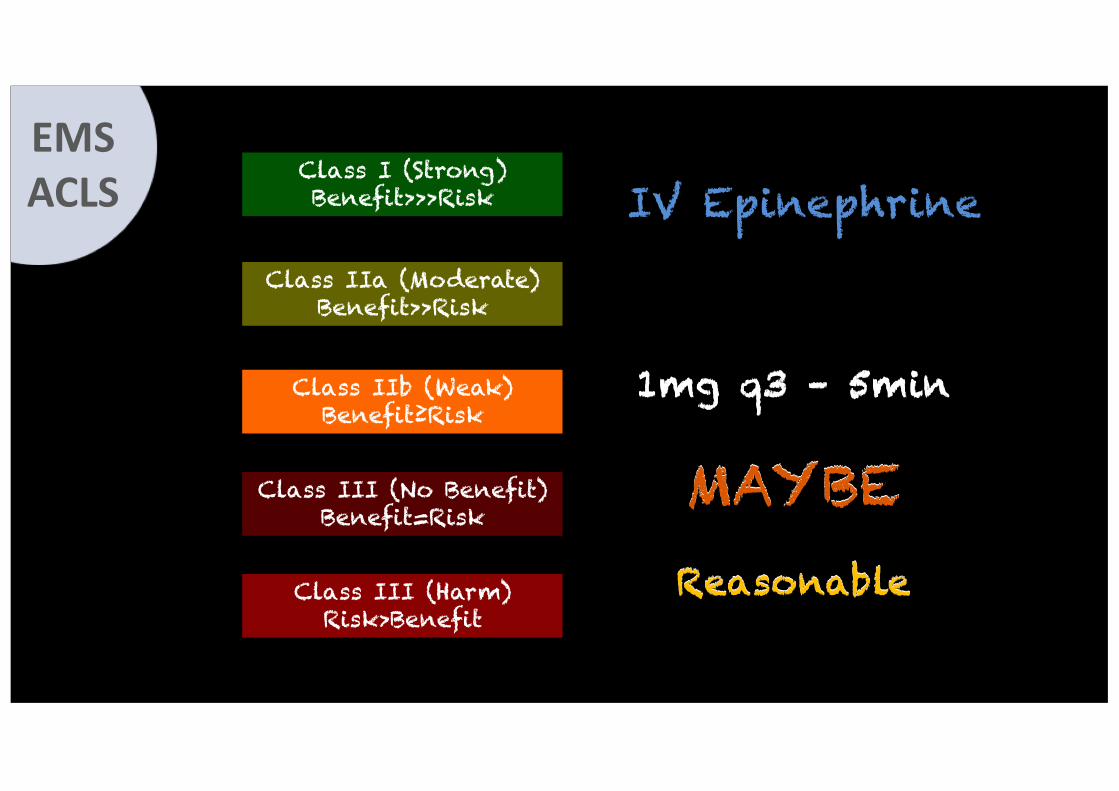
IV Epinephrine
1mg q3 – 5min
MAYBEReasonable
Class I (Strong)Benefit>>>Risk
Class IIa (Moderate)Benefit>>Risk
Class IIb (Weak)Benefit≥Risk
Class III (No Benefit)Benefit=Risk
Class III (Harm)Risk>Benefit
1mg q3 – 5min
MAYBEReasonable
EMSACLS
Evidence for Epi
OHCA
EMSACLS+
ROSC ≠ Neuro
Intact Survival
↑ ROSCNo ↑ Survival↑ Mortality

IV Access in the Field
EMSACLS

IO vs PIV
Higher Success Rate
Faster Access Achieved
EMSACLS+
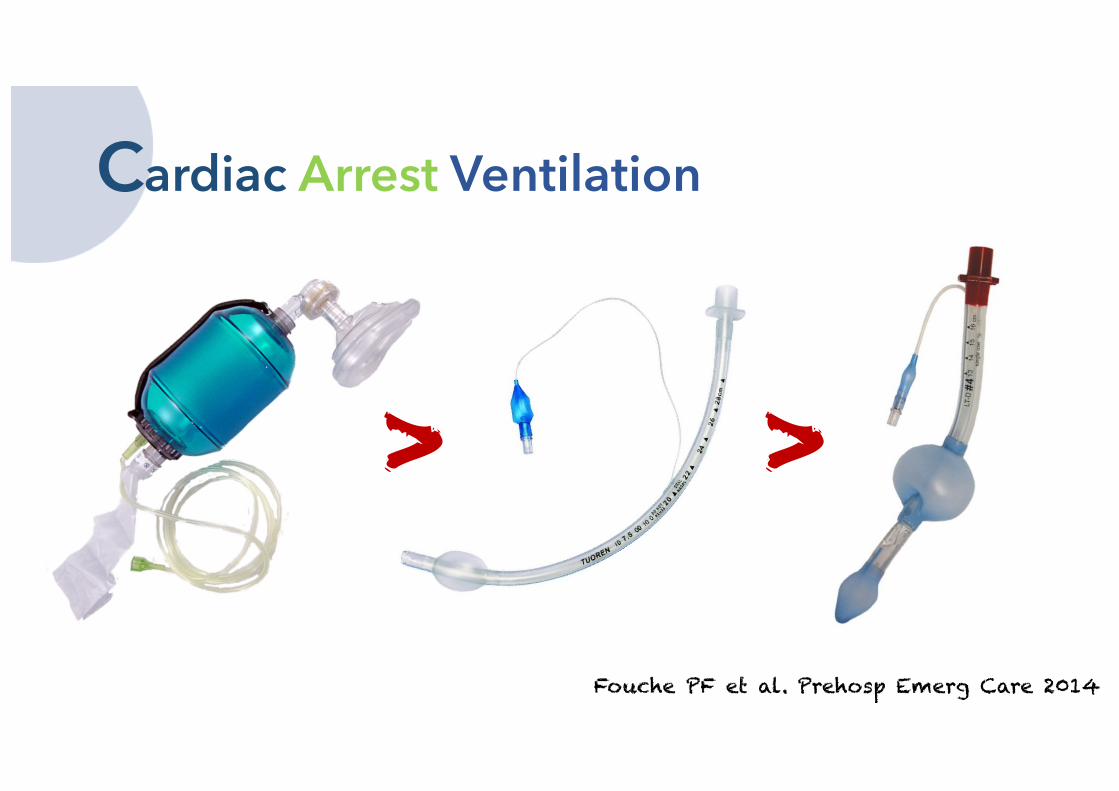
Cardiac Arrest Ventilation
Fouche PF et al. Prehosp Emerg Care 2014
> >

BVM Vent is Difficult!
EMSACLS
Guyette FX et al. Prehosp Emerg Care 2007
EMSACLS+
Is There Still Room for ETI?
Sunde GA et al. Scan J Trauma Resus Emerg Med 2015
EMSACLS+
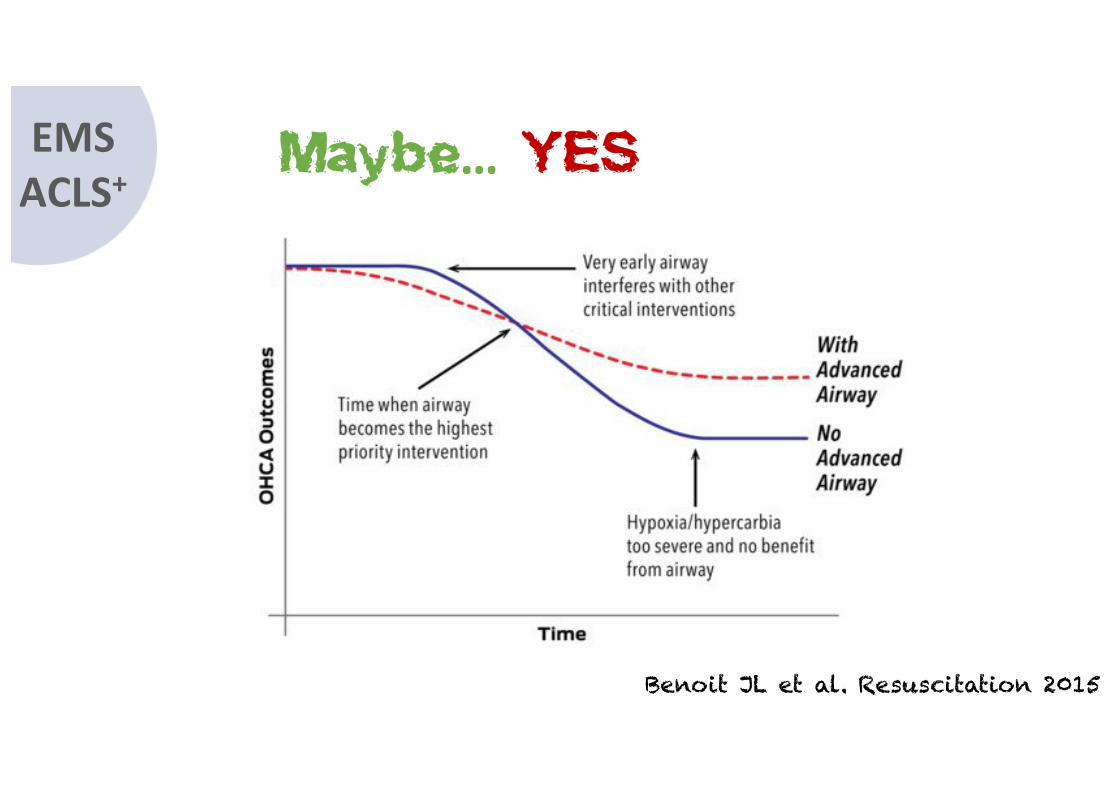
Maybe… YES
Benoit JL et al. Resuscitation 2015
b-card
ACLS & Beyond…?ACLS2020

b-card symposium
Thank You for Your AttentionQ & A
TuesdayMarch 7th
2017
Nicolas PESCHANSKI, MD, PhD