Embed Size (px)
Citation preview
2016 ESC Guidelines for the management of atrialfibrillation
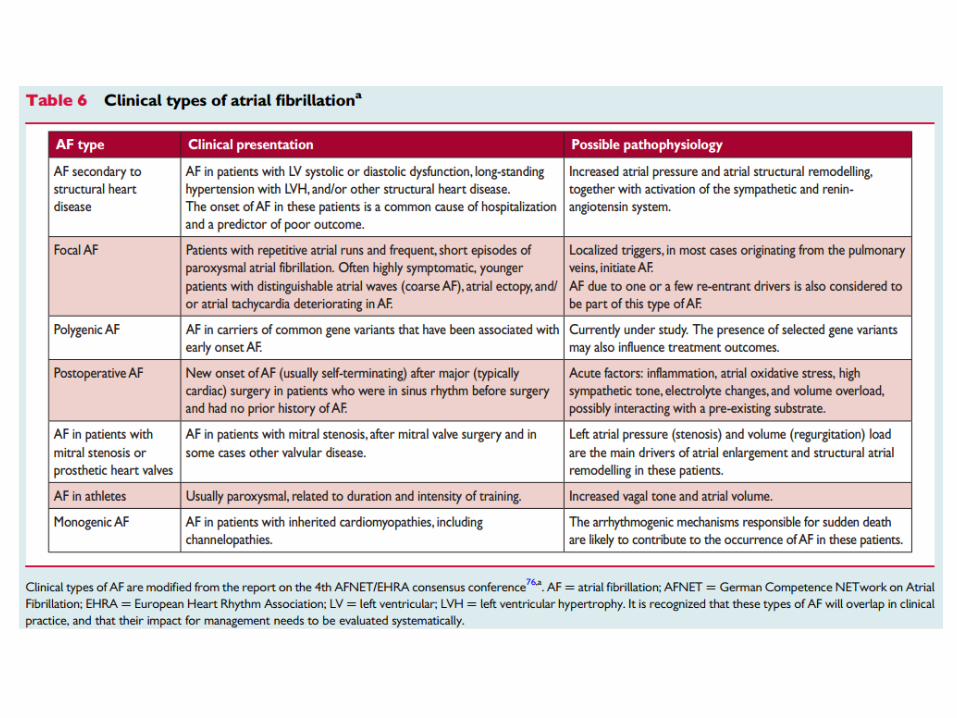
Valvular AF ?
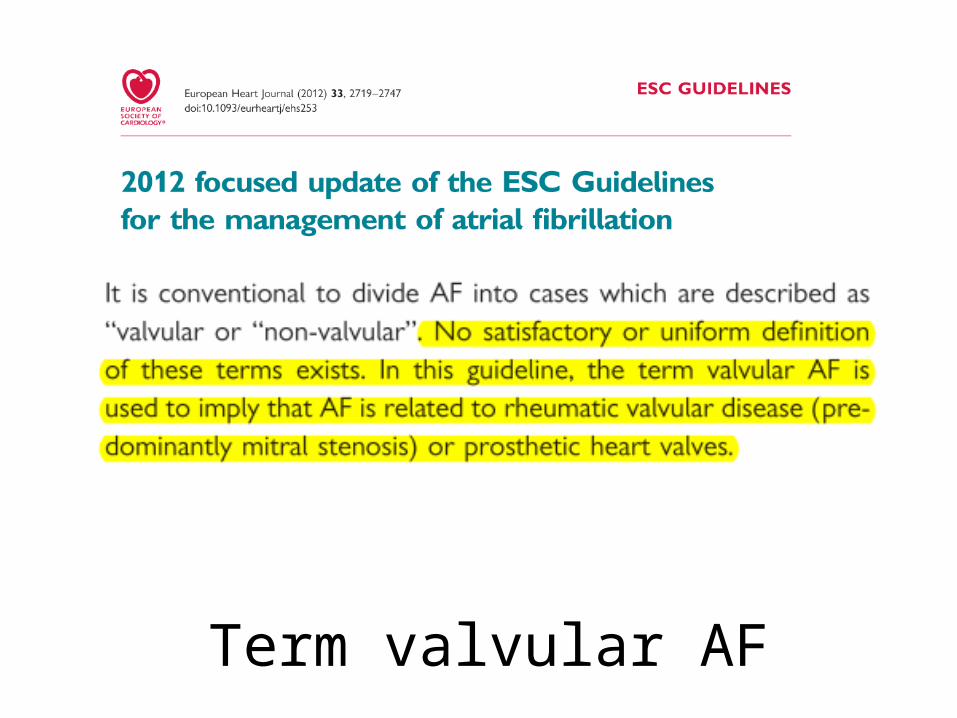
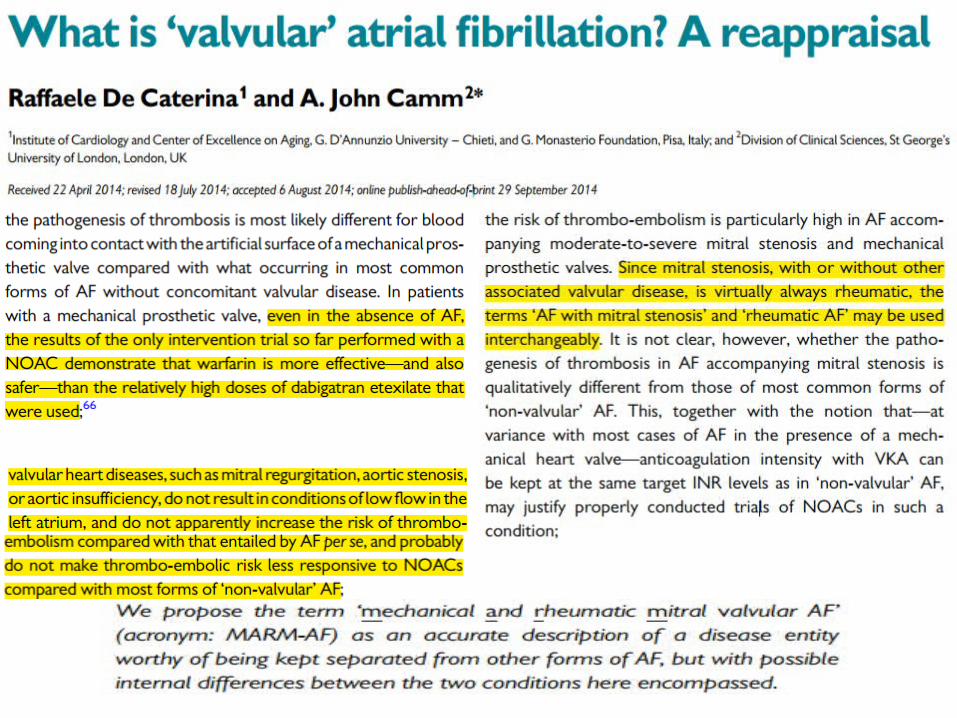
Term valvular AF

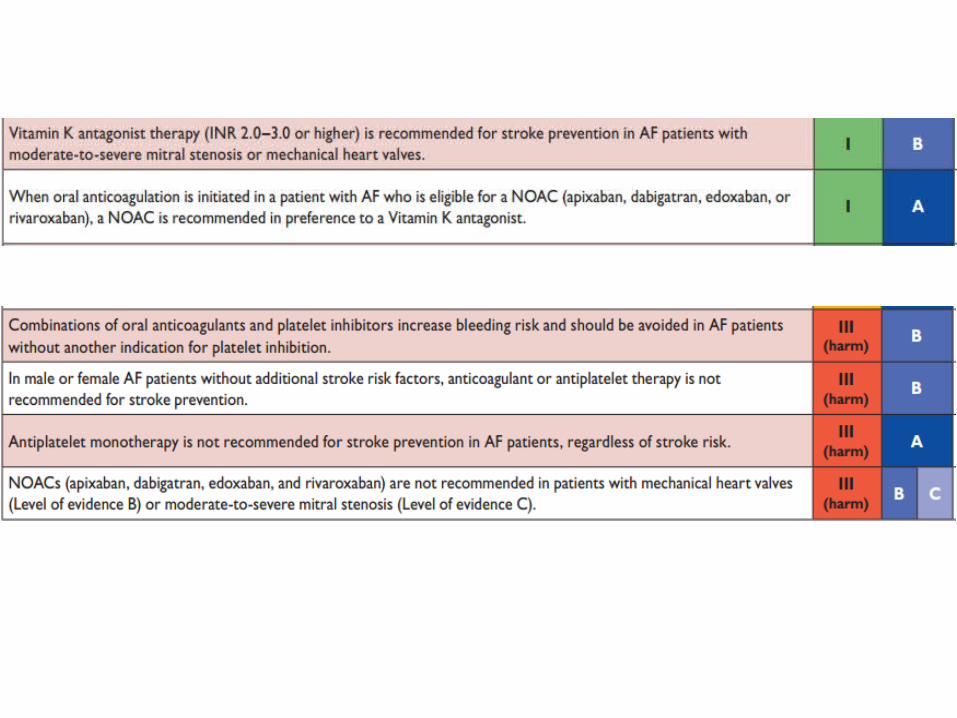
1. Stroke prevention in atrial fibrillation
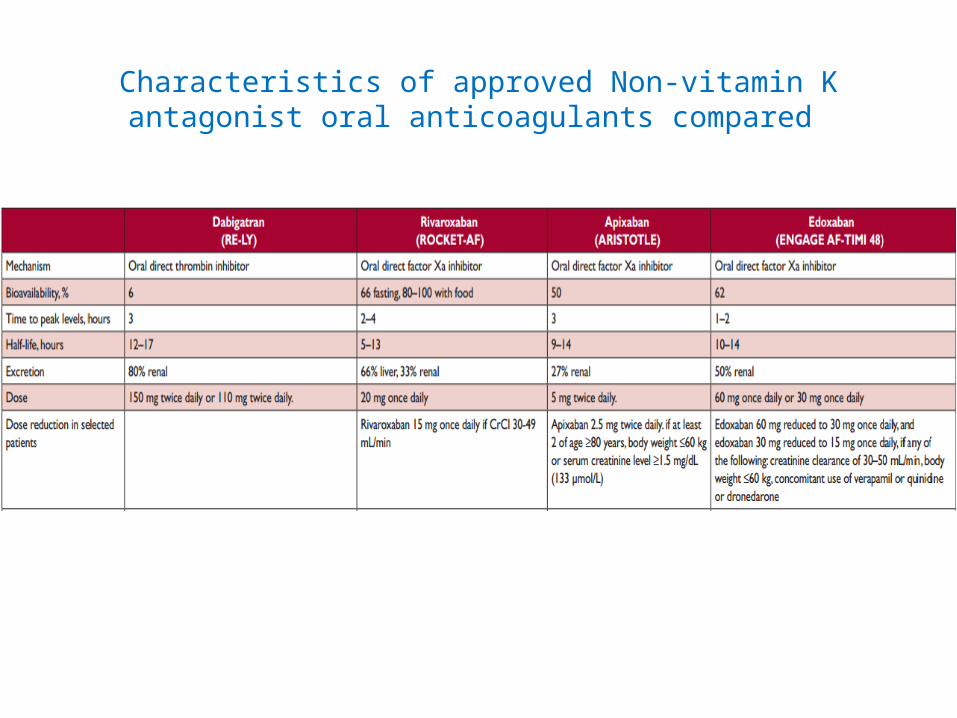
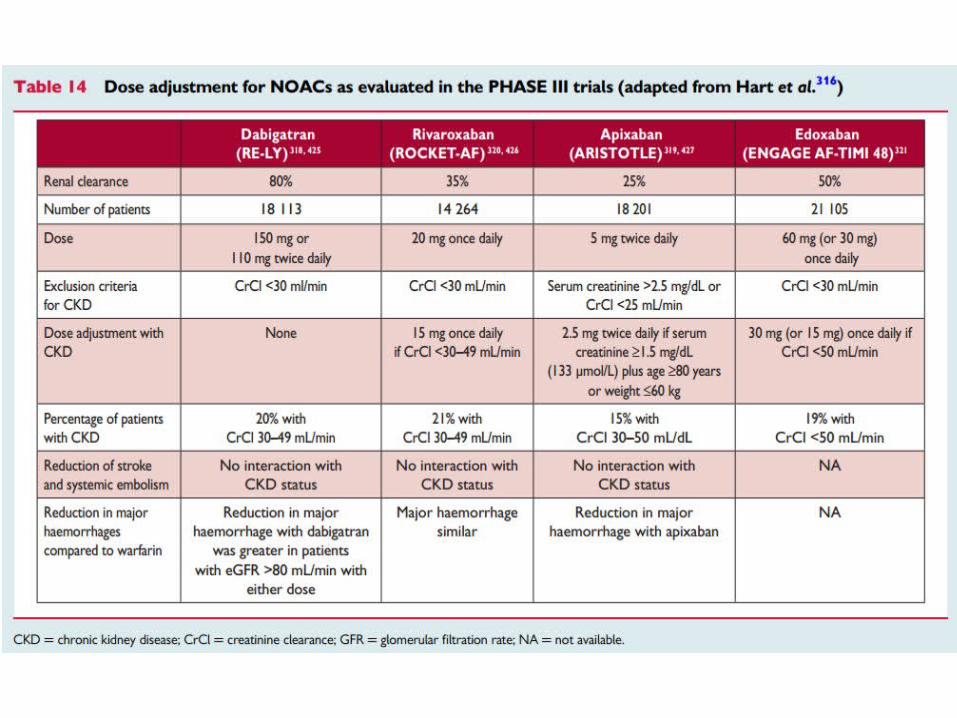
Characteristics of approved Non-vitamin K antagonist oral anticoagulants compared
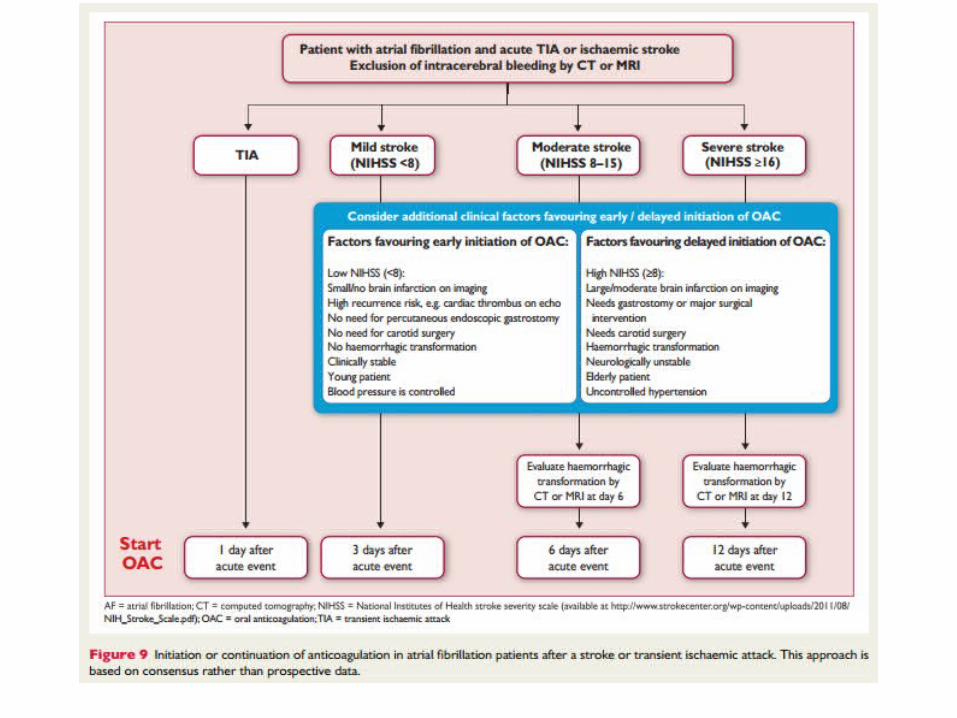
Secondary stroke prevention
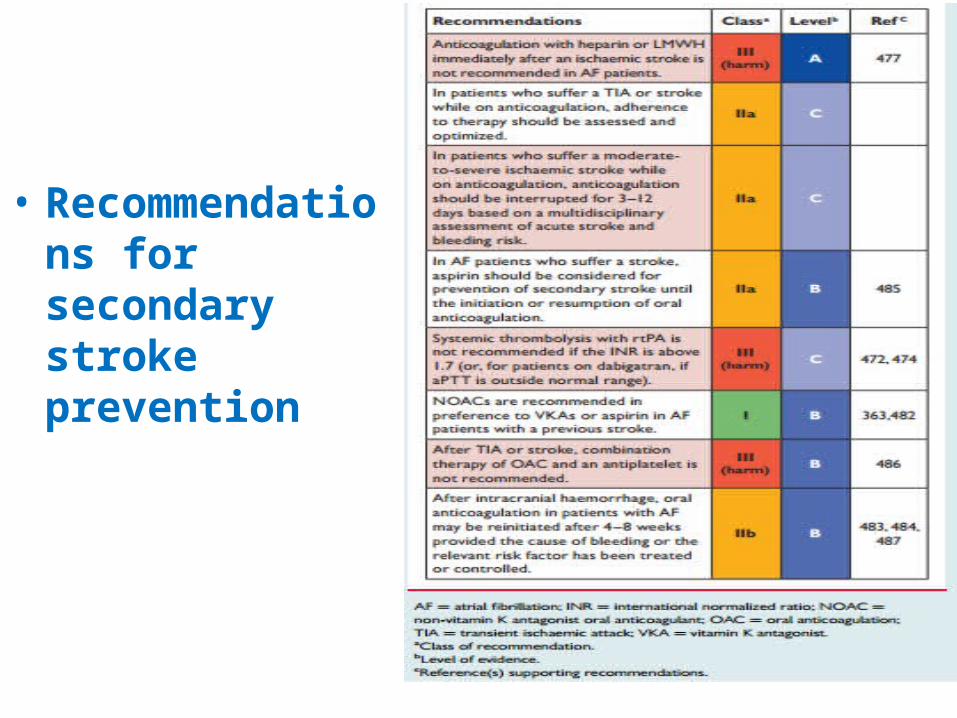
• Recommendations for secondary stroke prevention

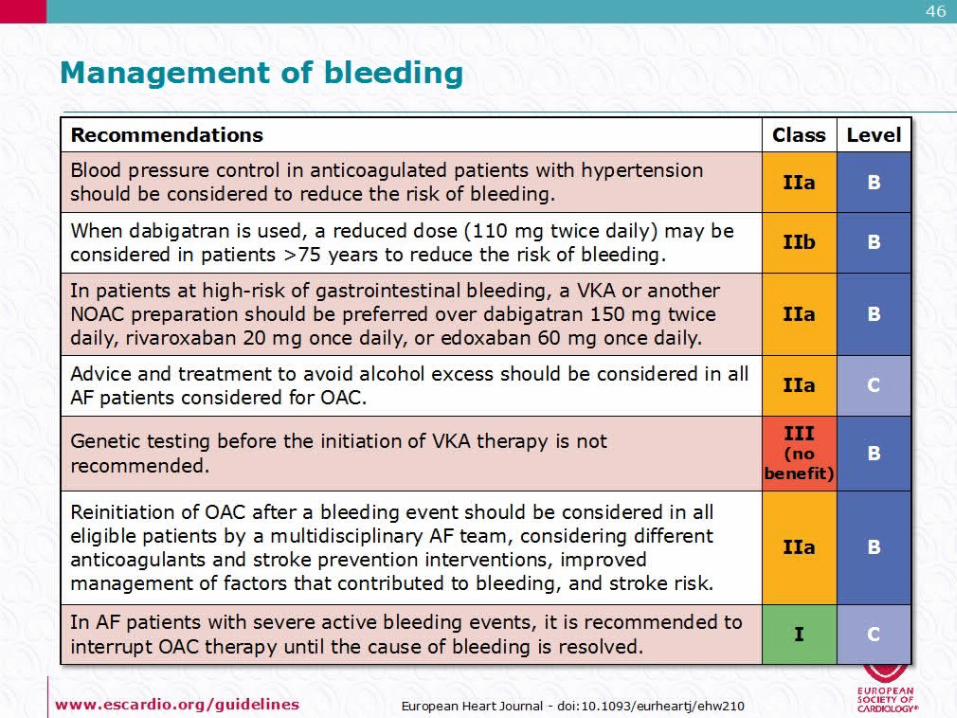
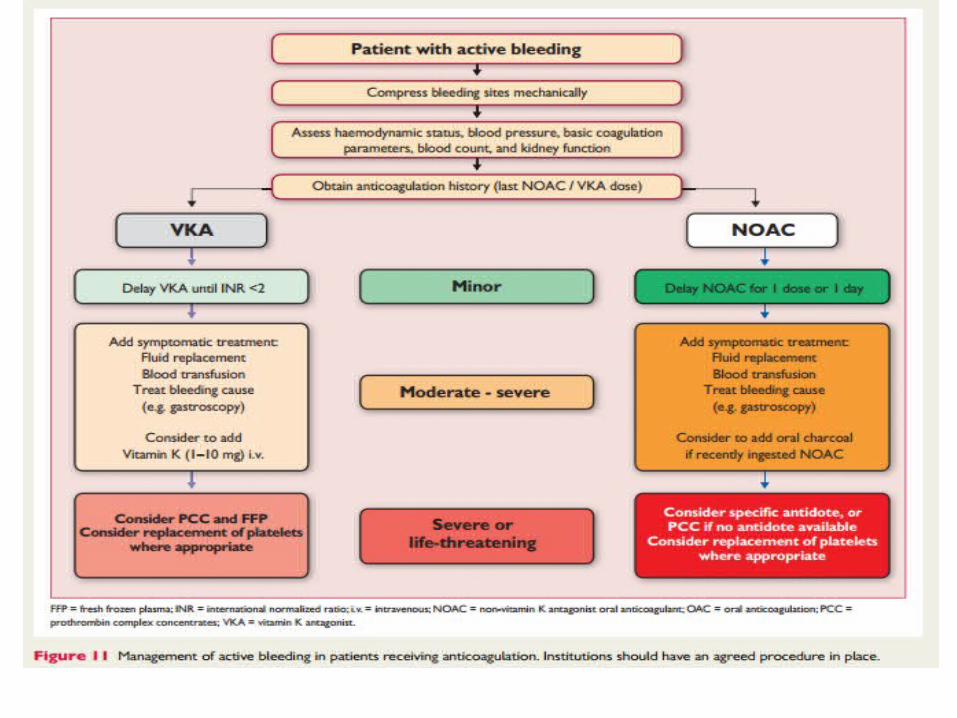
Recommendations for management of bleeding
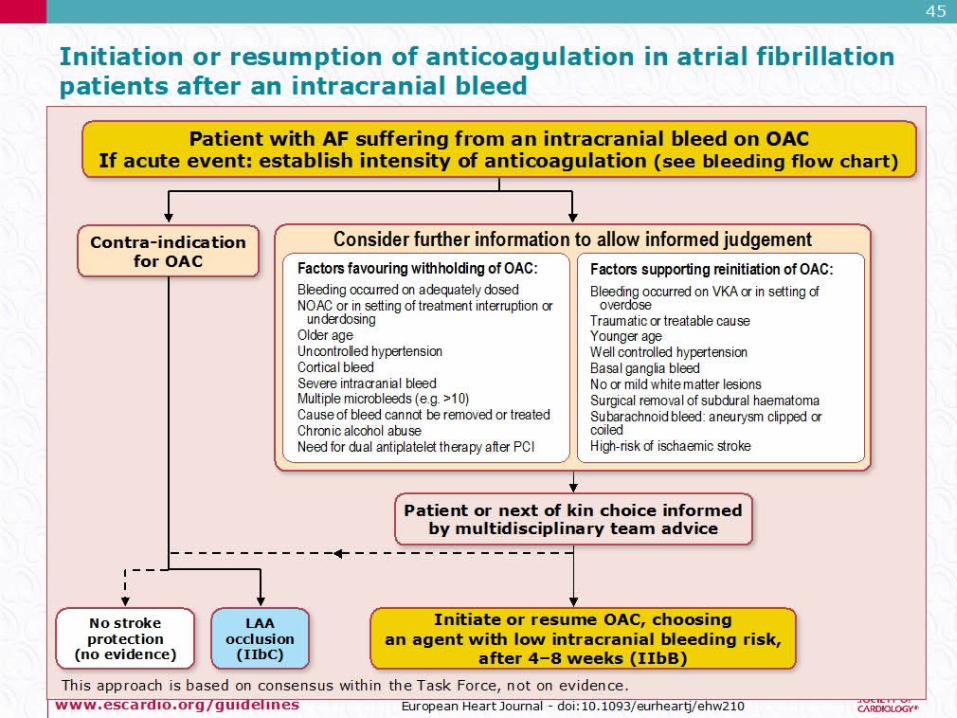
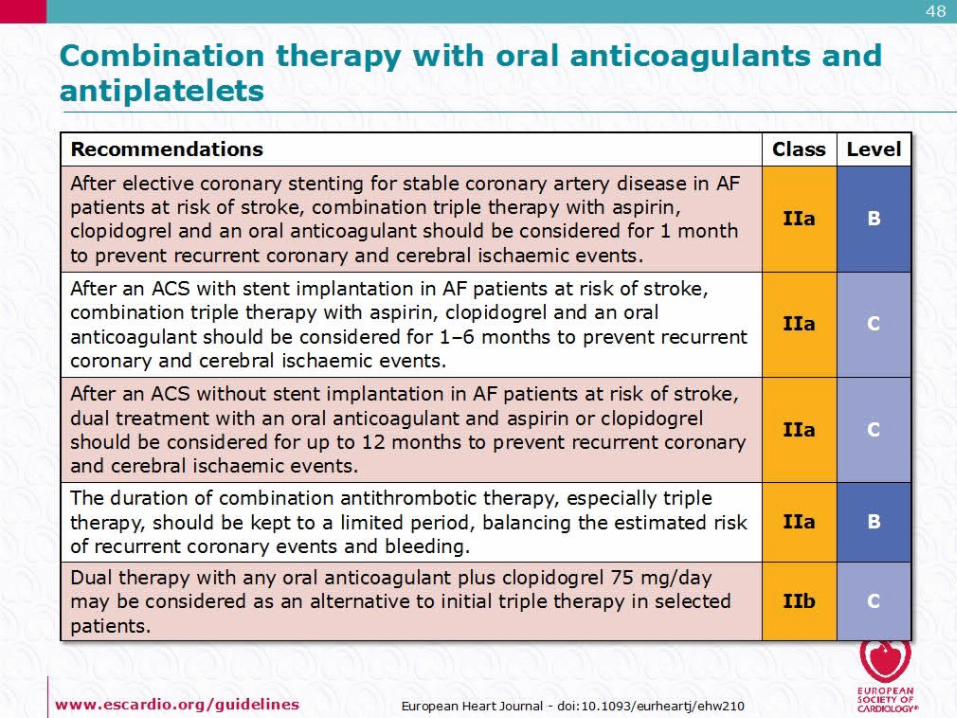
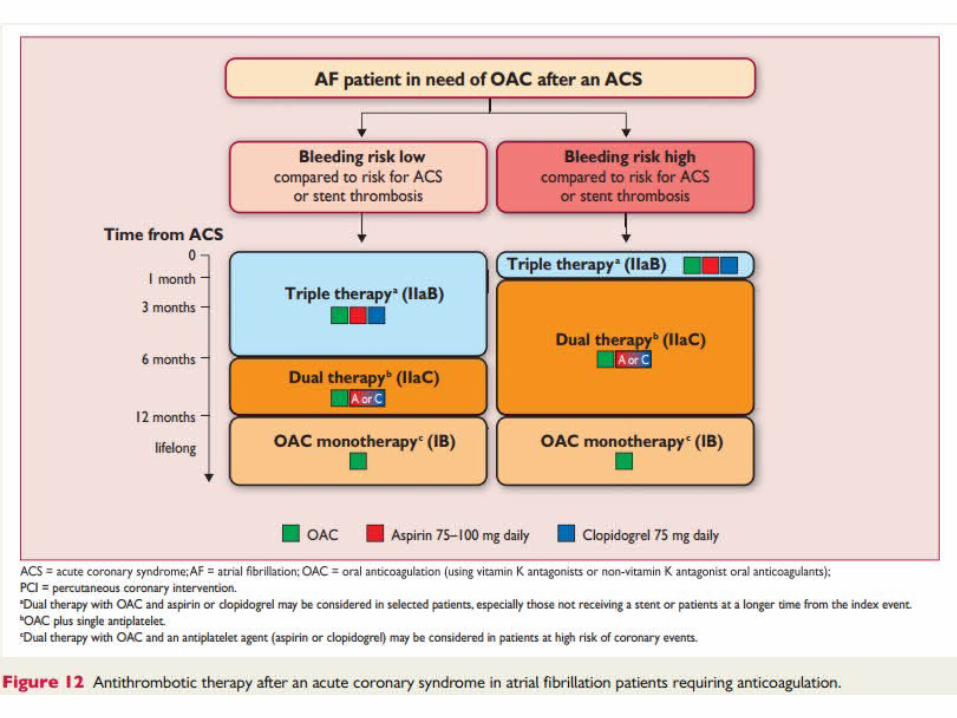
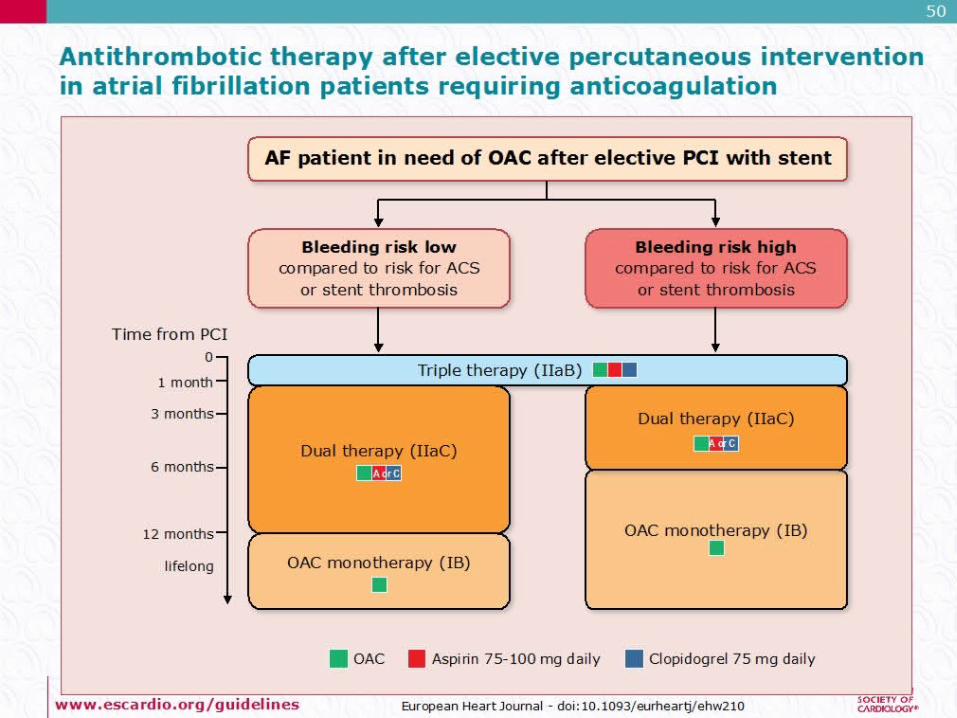
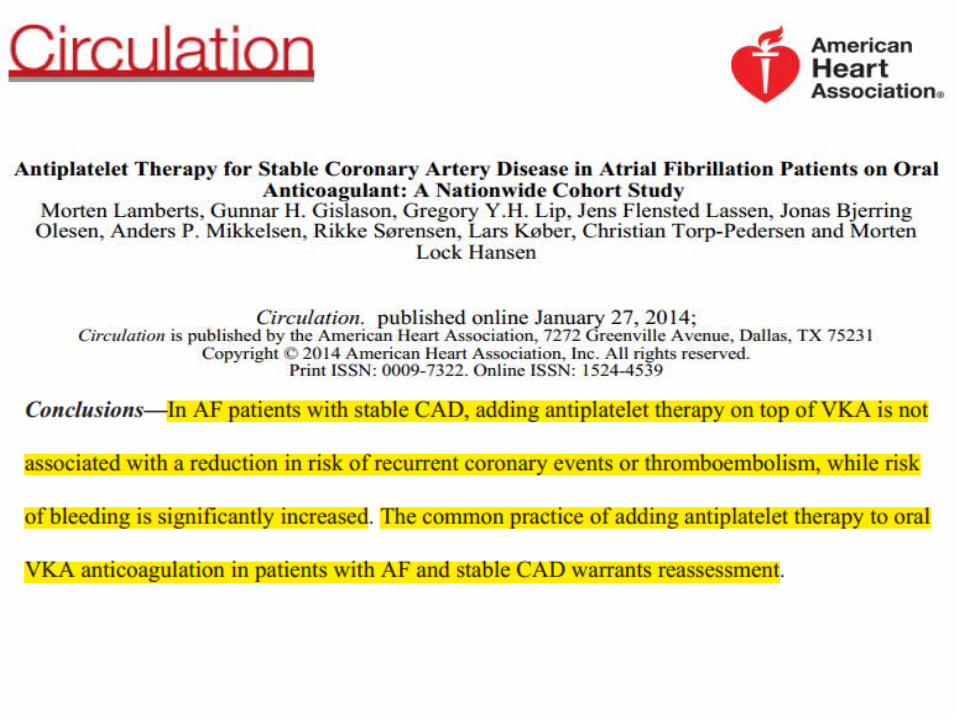
Combination therapy with oralanticoagulants and antiplatelets

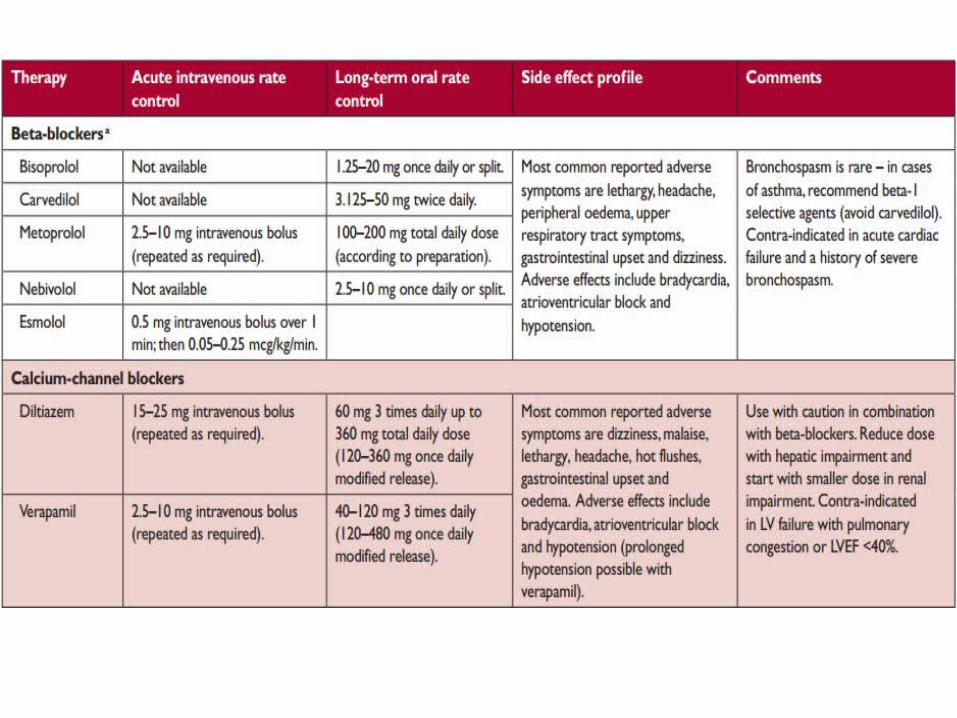
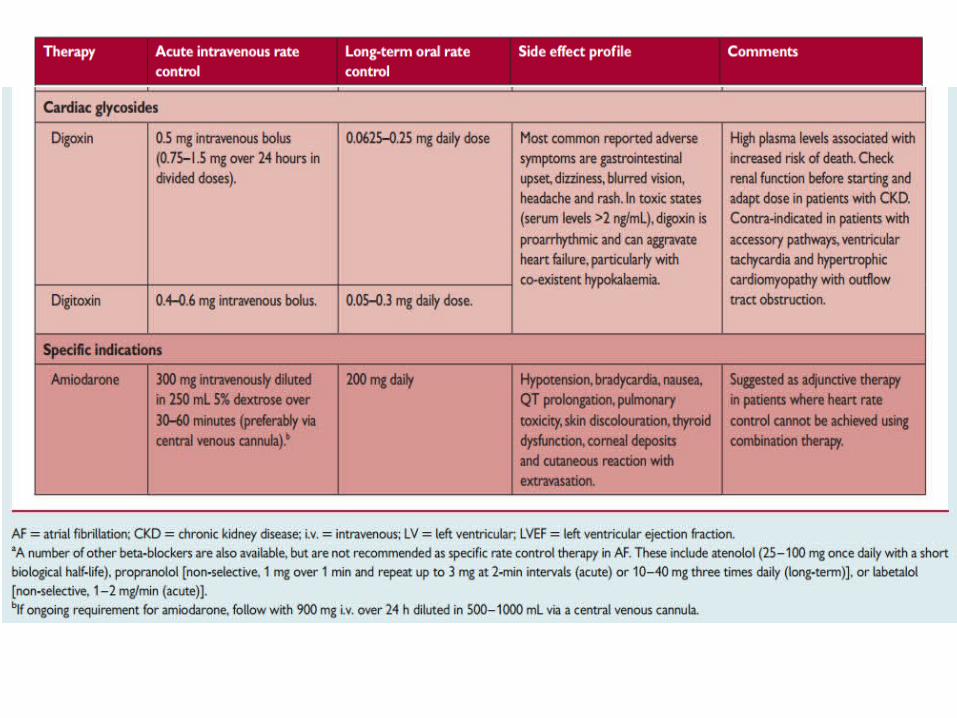
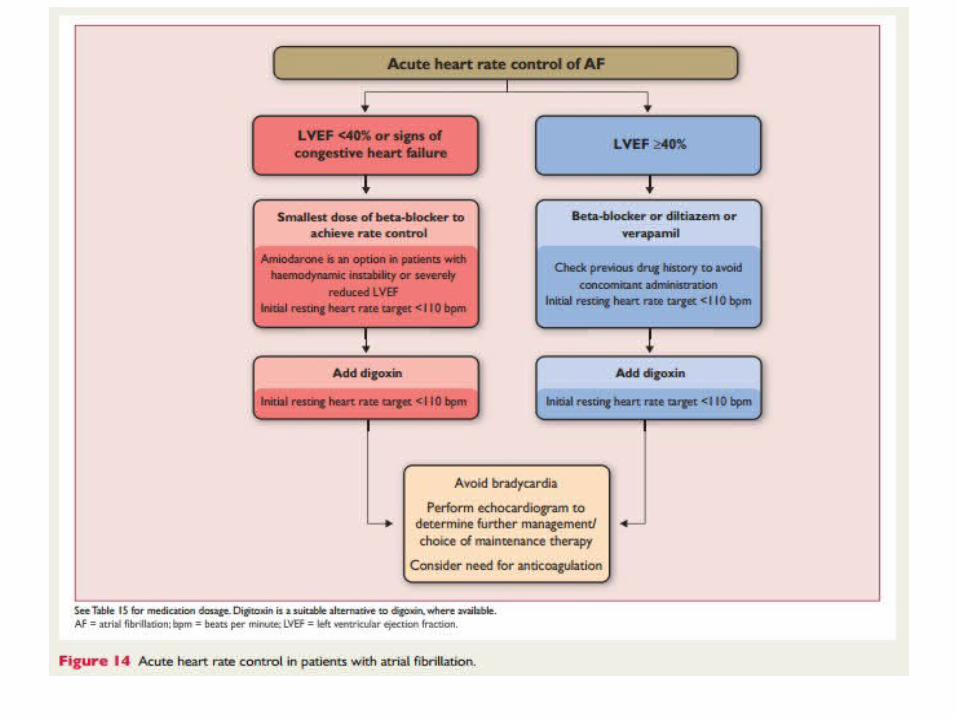
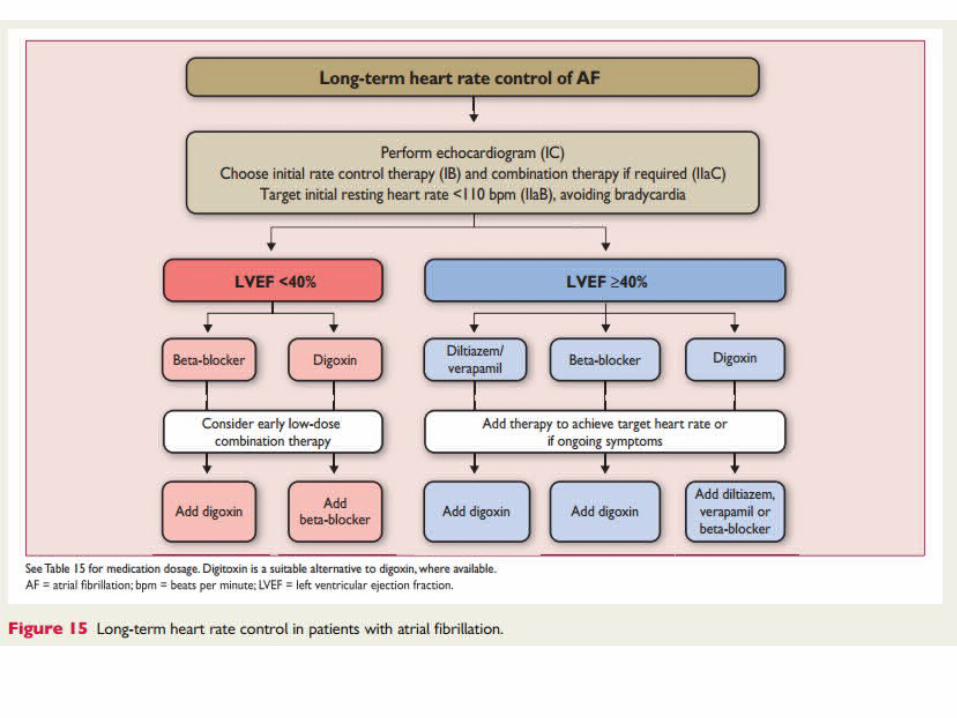
2.Rate control therapy in atrialfibrillation
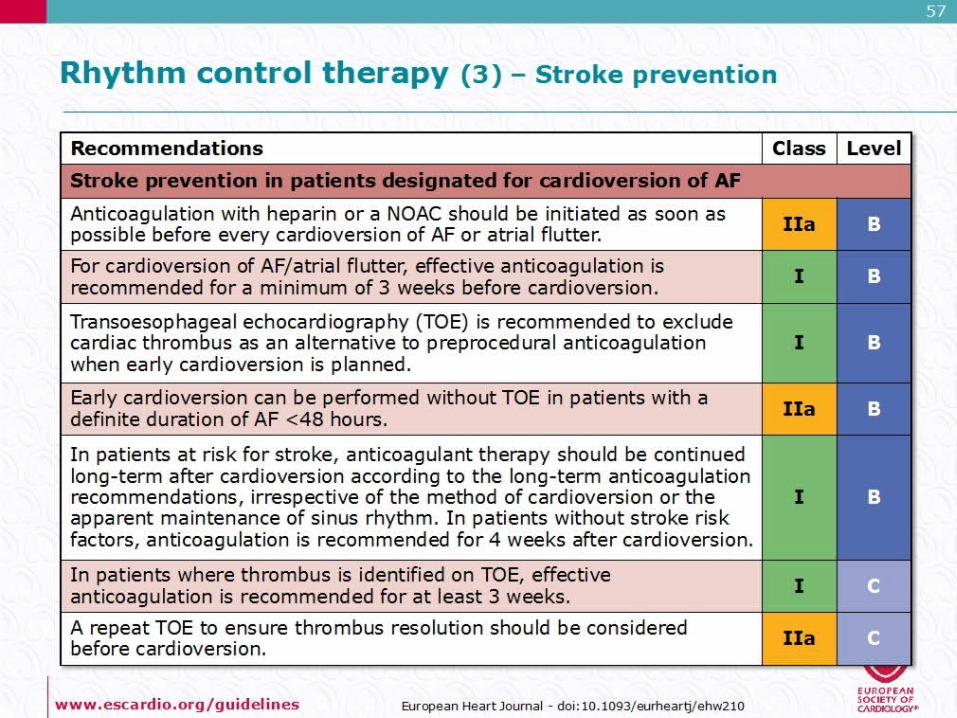
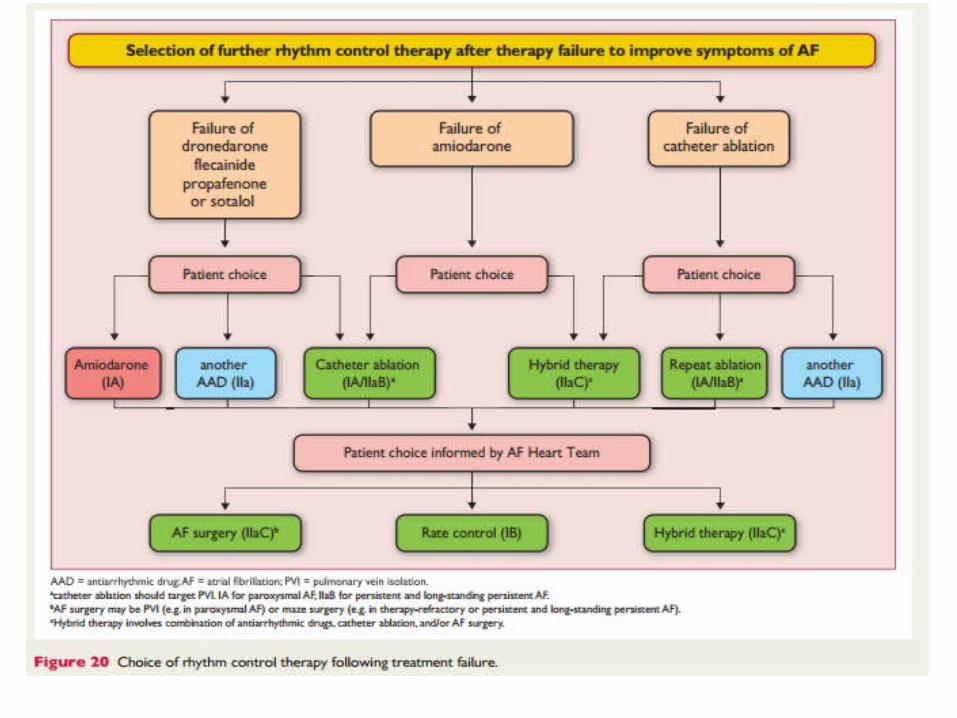
3. Rhythm control therapy inatrial fibrillation
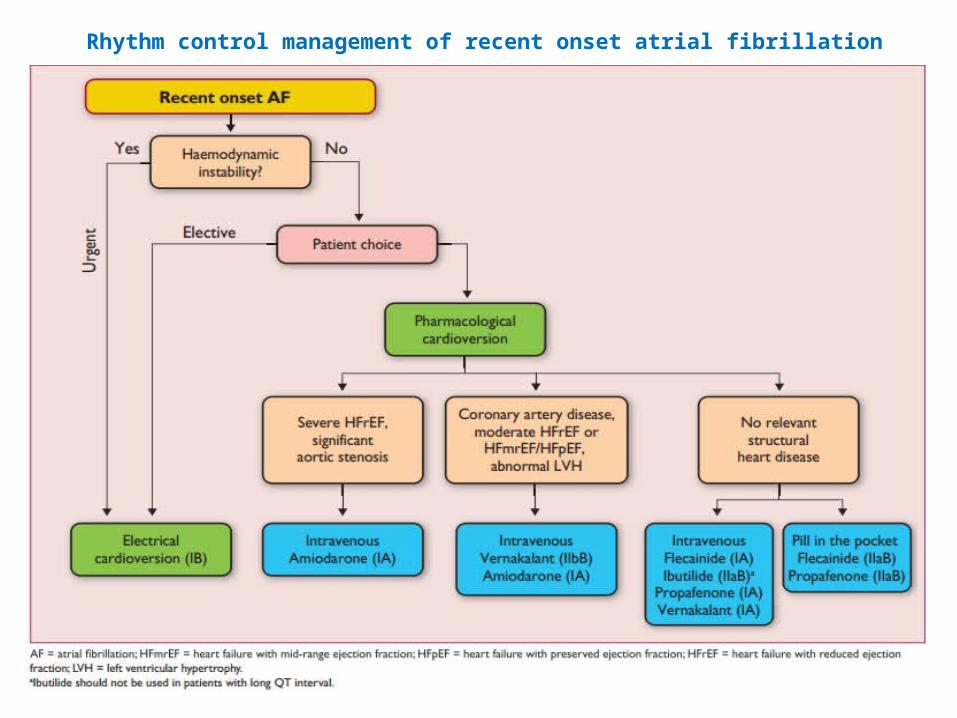
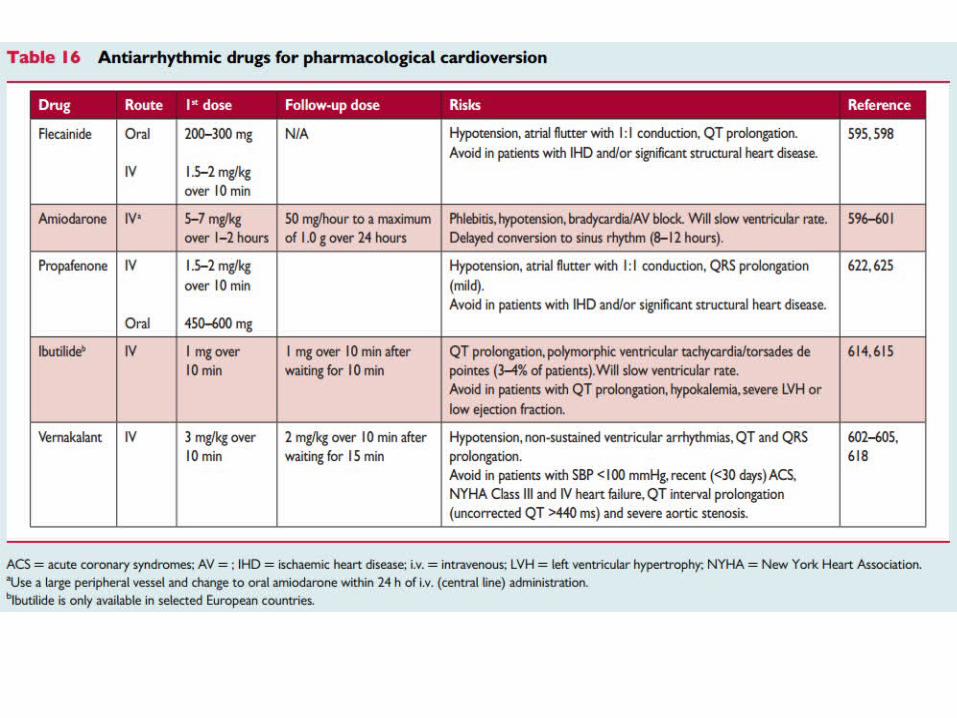
Rhythm control management of recent onset atrial fibrillation
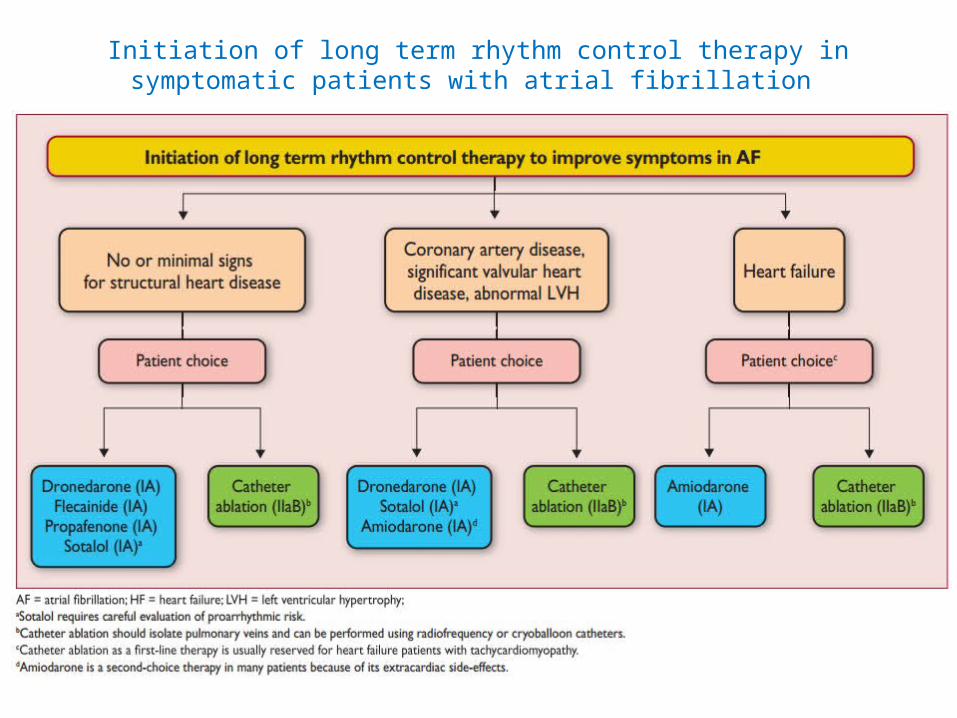
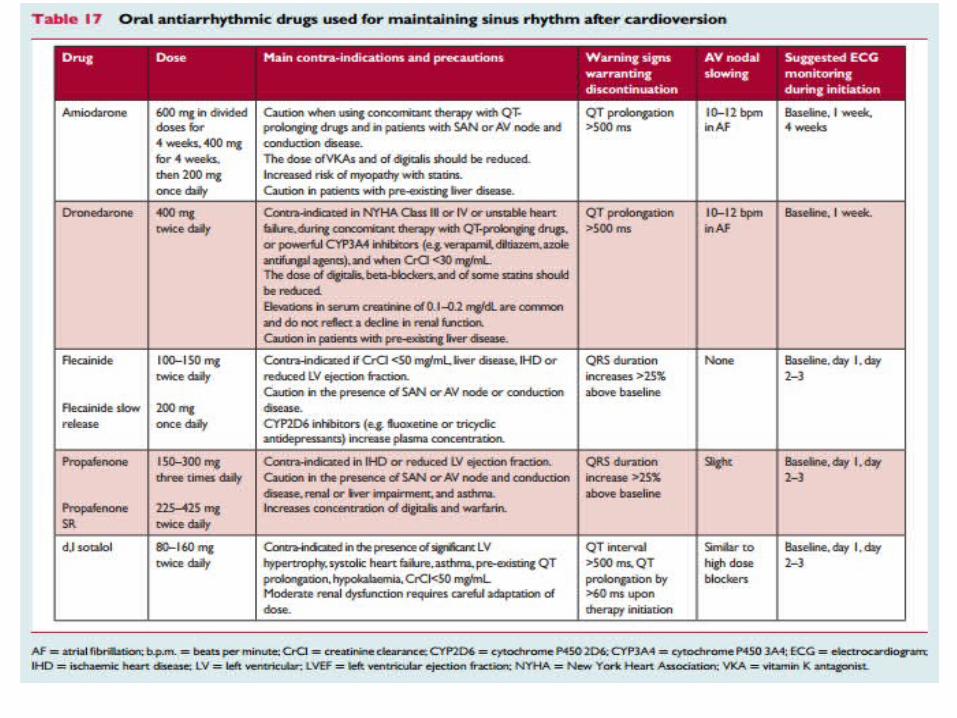
Initiation of long term rhythm control therapy in symptomatic patients with atrial fibrillation
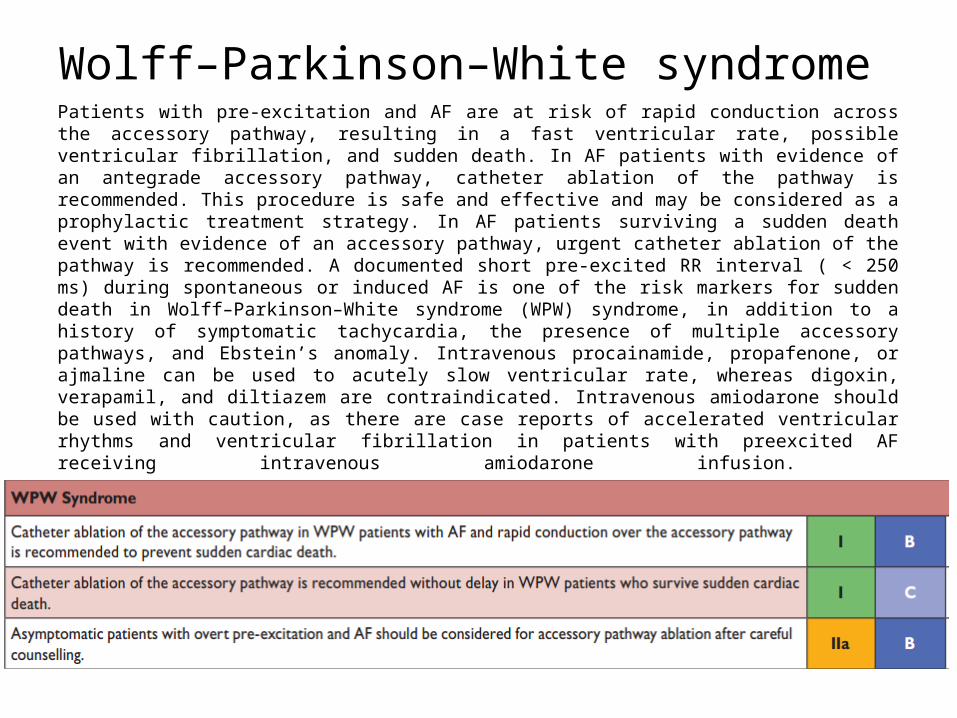
Wolff–Parkinson–White syndrome Patients with pre-excitation and AF are at risk of rapid conduction across the accessory pathway, resulting in a fast ventricular rate, possible ventricular fibrillation, and sudden death. In AF patients with evidence of an antegrade accessory pathway, catheter ablation of the pathway is recommended. This procedure is safe and effective and may be considered as a prophylactic treatment strategy. In AF patients surviving a sudden death event with evidence of an accessory pathway, urgent catheter ablation of the pathway is recommended. A documented short pre-excited RR interval ( < 250 ms) during spontaneous or induced AF is one of the risk markers for sudden death in Wolff–Parkinson–White syndrome (WPW) syndrome, in addition to a history of symptomatic tachycardia, the presence of multiple accessory pathways, and Ebstein’s anomaly. Intravenous procainamide, propafenone, or ajmaline can be used to acutely slow ventricular rate, whereas digoxin, verapamil, and diltiazem are contraindicated. Intravenous amiodarone should be used with caution, as there are case reports of accelerated ventricular rhythms and ventricular fibrillation in patients with preexcited AF receiving intravenous amiodarone infusion.