Embed Size (px)
Citation preview
New guideline on Treatment of Blood Cholesterol
to reduce ASCVD risk
Dr. Kamal modi
Biochemistry dept.
Points of New ATP iv guidlines
Focus on ASCVD risk reduction
New perspective on LDL-C & Non-HDL-C treatment goals
Global risk assesment for Primary prevention
Safety recommendation
Role of Biomarkers and Non-invasive tests
Future updates to the blood cholesterol guidelines
Focus on ASCVD risk reduction
Classified into 4 statin benefit groups:
1. Individuals with clinical ASCVD 2. Individuals with primary elevation of LDL–C > 190 mg/dl 3. Individuals 40- 75 years of age with diabetes with LDL-C 70- 189 mg/dl 4. Individuals without clinical ASCVD or diabetes who are 40 – 75 years of age with LDL-C 70-189 mg/dl and an estimated 10 year ASCVD risk of 7.5 % or higher.
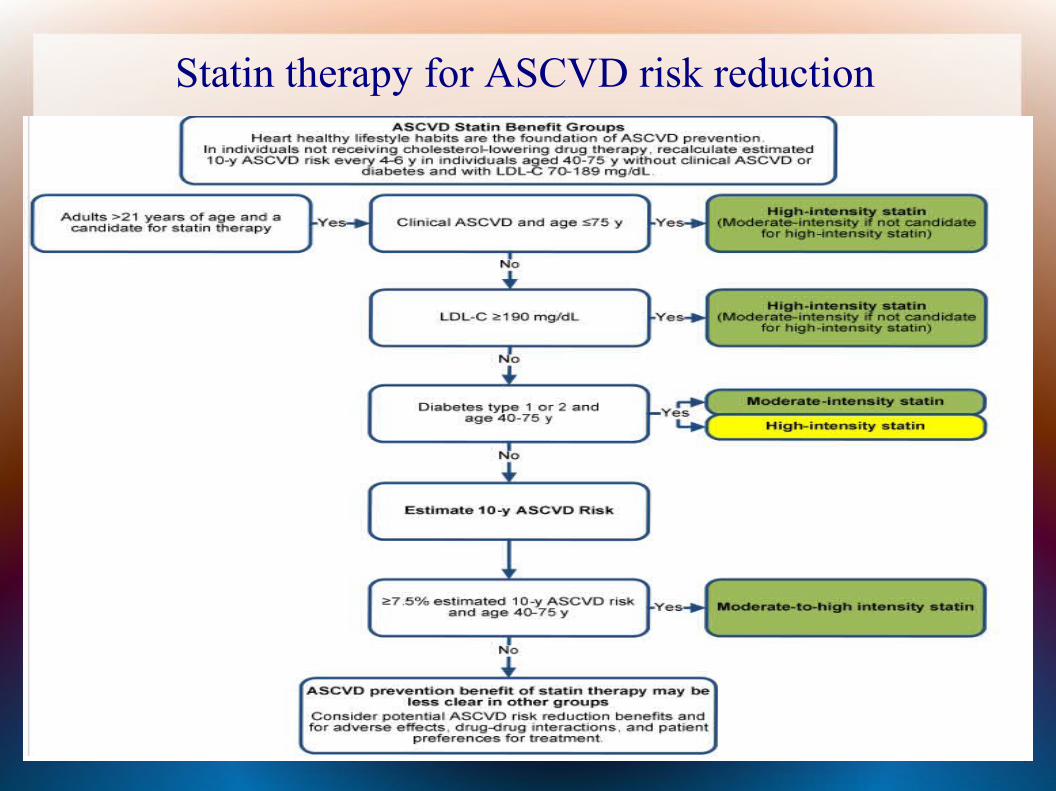
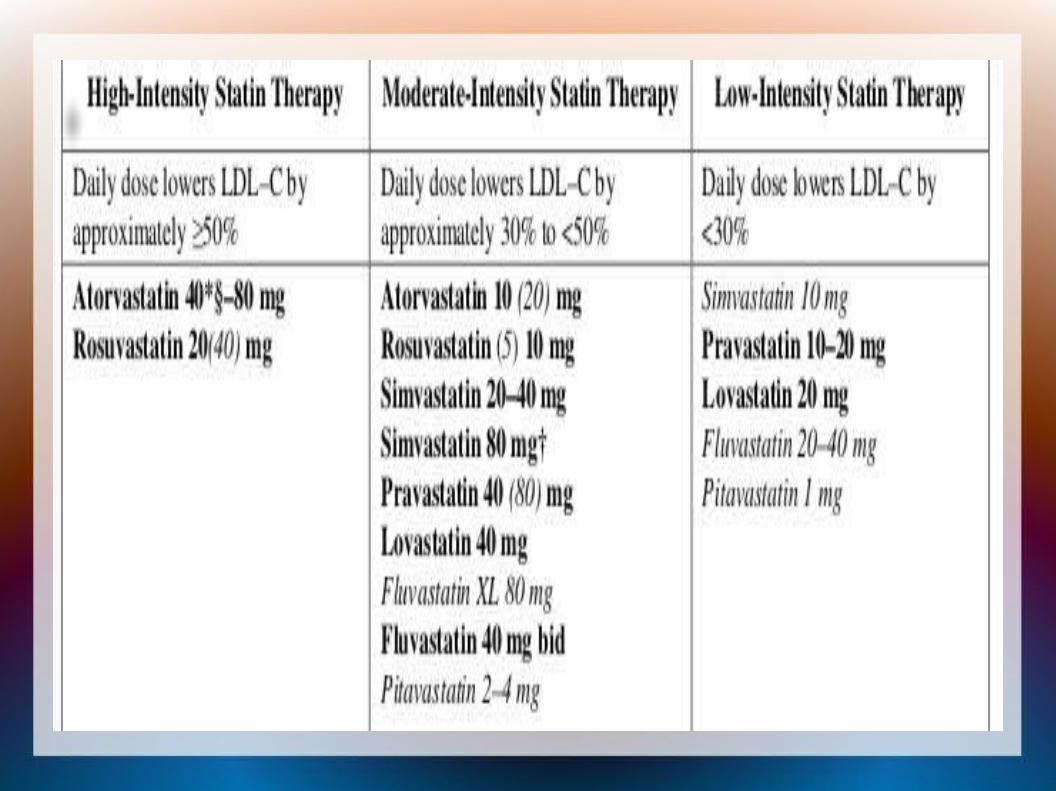
Statin therapy for ASCVD risk reduction
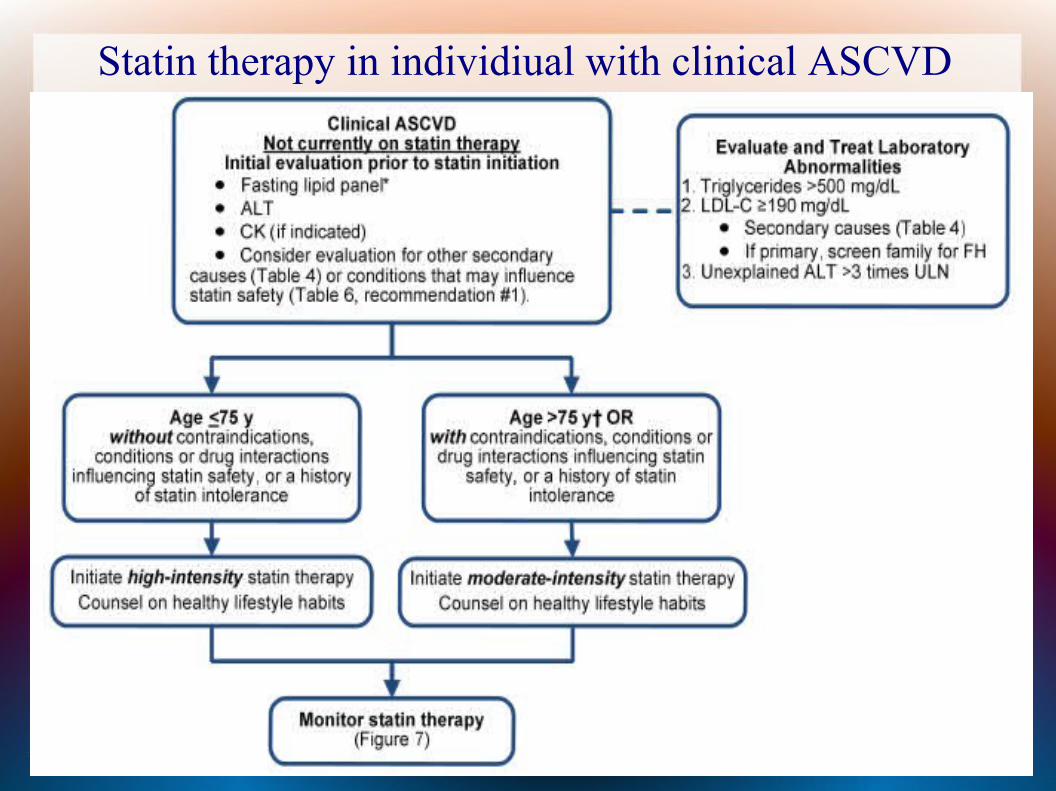
Statin therapy in individiual with clinical ASCVD
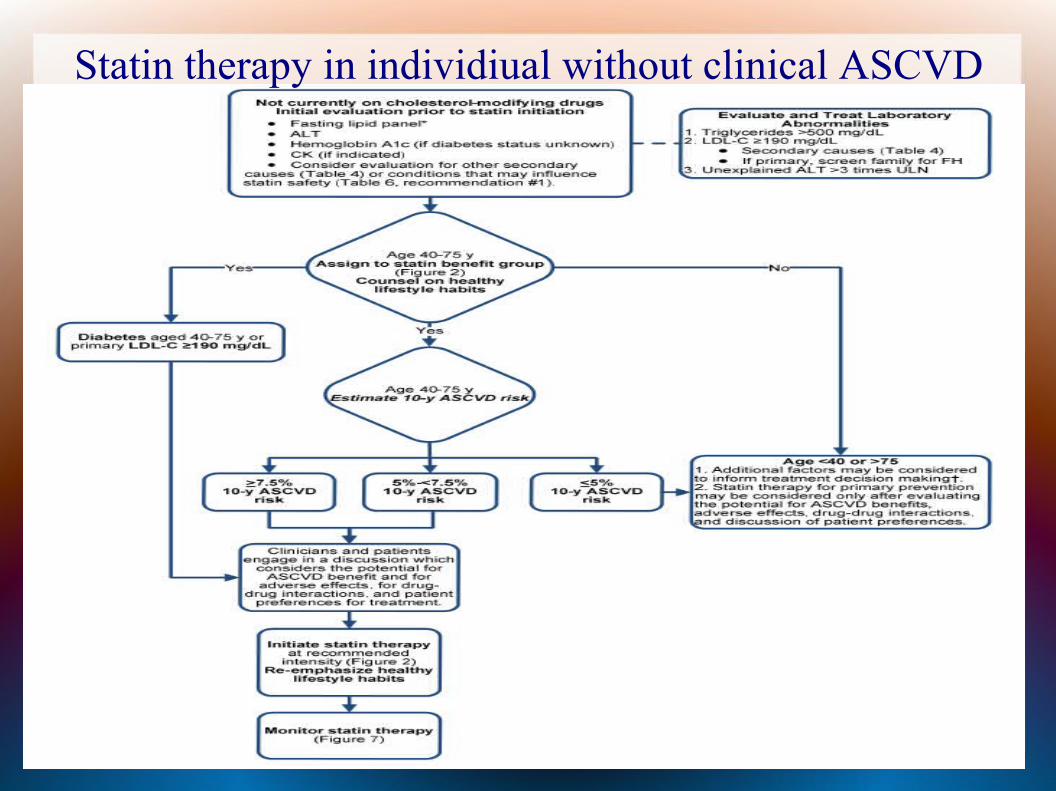
Statin therapy in individiual without clinical ASCVD
Role of Biomarkers and Non-invasive tests
For treatment decision in selected individuals who are not included in the 4 statin benefit groups.
Other factors:
1. Primary LDL-C > 160 mg/dl2. Genetic hyperlipidemias3. Family history of premature ASCVD with onset
<55 years of age in first degree male relative or < 65 years of age in first degree female relative
4. C-reactive protein > 2 mg/dl5. CAC score > 300 Agaston units or > 75
percentile for age , sex and ethnicty6. Ankle brachial index < 0.97. Elevated lifetime risk of ASCVD
Limitation
• Younger adults (< 40 years) who have low estimated 10 year ASCVD risk but high lifetime ASCVD risk
• Persons with serious comorbidities :
Rheumatologic or inflammatory disease,
HIV positive
Solid organ transplant
• No ASCVD risk reduction with statin therapy in individuals with class ii – iv heart failure or undergoing hemodialysis .
New perspective on LDL-C & Non-HDL-C treatment goals
Appropriate intensity of statin therapy should be used.
Non-Statin therapies do not provide acceptable benefits compared to their adverse effects in routine prevention of ASCVD.

Non-Statin drug therapy
• Niacin
• Bile acid sequestrants : cholestyramine, colestepol , colesevalam
• Fibric acid derivatives: gemfibrozil, fenofibrate, clofibrate
Safety recommendation
Identifies important safety considerations
Facilitates understanding of the net benefit from statin therapy
Provides guidance on management of statin associated adverse effects
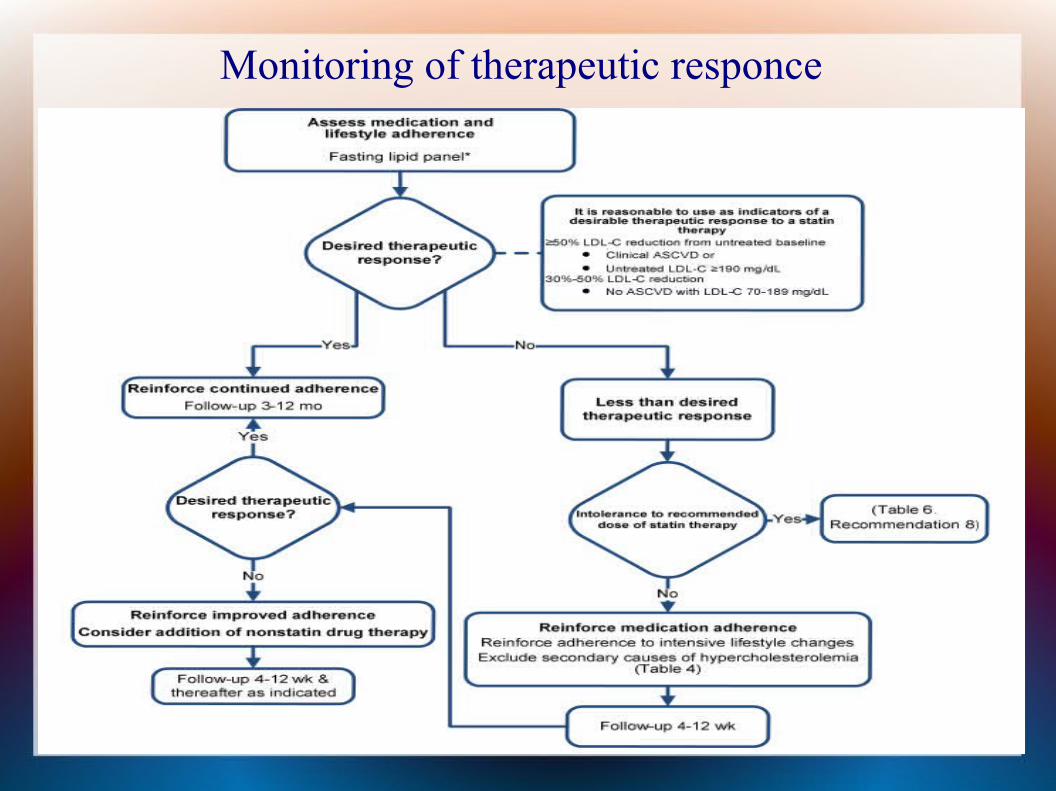
Monitoring of therapeutic responce
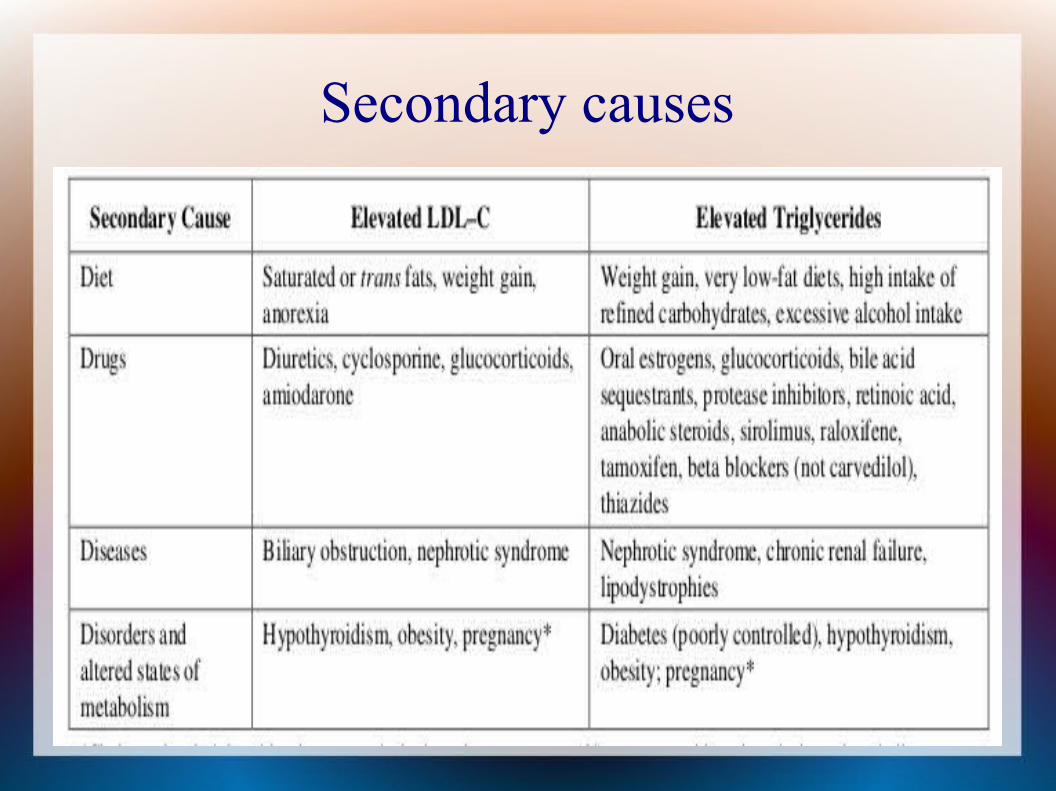
Secondary causes
Global risk assessment for Primary prevention
Use of the new pooled cohort equation is recommended to estimate 10 year ASCVD risk in both white and black men and women who do not have clinical ASCVD.
Available at “my.americanheart.org”
Future updates to the blood cholesterol guidelines
• To provide expert guidance on management of complex lipid disorders and refinements in risk stratification based on critical review of emerging data.
RCTs comparing alternate treatment stratigies are needed in order to inform future evidence based
guidelines for optimum ASCVD risk reduction approach.
• Guidelines for individuals with class ii – iv heart failure or undergoing hemodialysis that might benefit from statin therapy.
• Whether on treatment markers such as ApoB, Lp(a), LDL particles are useful for guiding treatment decisions
• How lifetime risk should be used to inform treatment decisions and the optimal age for initiating statin therapy to reduce lifetime risk of ASCVD.
• Efficacy and safety of statins in patents with HIV positive or solid organ transplant.
Thank you…..