Embed Size (px)
DESCRIPTION
Dr Anne Boyter
Citation preview

Educational Solutions for Workforce Development
PharmacyAsthma
Dr Anne Boyter
School of Pharmacy
Strathclyde Institute of Pharmacy & Biomedical Sciences
University of Strathclyde

Introduction

Guideline History
– 1990 – 5 pages – 4 references– 1993 – 24 pages – 80 references– 2003 –Collaboration SIGN / BTS
• 92 pages – 517 references (inc evidence tables) SIGN 63
– 2004 – 2007 – living guideline– May 2008 – reissue Thorax & SIGN 101
• 121 pages – 766 references (inc evidence tables)
– June 2009 – on-line update

Other guidelines
GINA– Global Initiative for Asthma– Multinational collaboration– Last updated 2008

Asthma definition
• a chronic inflammatory disorder of the airways …… in susceptible individuals, inflammatory symptoms are usually associated with widespread but variable airflow obstruction and an increase in airway response to a variety of stimuli. Obstruction is often reversible, either spontaneously or with treatment.
ATS

Asthma definition
• Diagnosis of asthma is a clinical one….there is no standardised definition of the type, severity or frequency of symptoms, nor of the findings on investigation.
• Presence of symptoms…wheeze, cough, breathlessness, chest tightness… airway hyperresponsiveness…airway inflammation…
SIGN 101

Diagnosis

Diagnosis
Children– Lung function cannot be reliably used to
guide asthma management in children under the age of 5

Diagnosis -adults
Based on probability of asthma• High / Intermediate / Low
PEFR• Not recommended for diagnosis
Spirometry• Preferred initial test to assess airflow
obstruction

High or low probability
High probability– Trial of treatment– Reserve further testing for those with poor
responseLow probability
– Investigate & manage alternative diagnosis– Reconsider asthma in patients who don’t
respond

Intermediate probability
• Carry out further investigation• Trial of treatment for a specified length of
time• Confirm diagnosis
– TREATMENT

Reference steroid

Reference steroid
• Until May 2009– BDP given by CFC –MDI
• BDP CFC phased out– BDP – HFA equivalent– Reference doses remain the same
• Equivalence table in the guideline

Steroid Equivalent dose >12 years 5 – 12 years
<5 years
Beclometasone dipropionate CFC 400mcg No longer available
Budesonide
Turbohaler
400mcg
Metered dose inhaler Over age 2
Easyhaler Over age 6
Novolizer Over age 6
Symbicort Over age 6
Symbicort (regular and as required dosing)
Over age 18
Fluticasone
MDI (HFA)
200mcg
Over age 4
Accuhaler Over age 4
Seretide HFA Over age 4
Seretide (Accuhaler) Over age 4

Aims of treatment

Aim of management
• Aim of asthma management is to control the disease
• Control is defined as– No daytime symptoms– No night time wakening due to asthma– No need for rescue medication– No exacerbations– No limitations on activity including exercise– Normal lung function
• FEV1 and /or PEFR >80% predicted or best

Patient aims of treatment
• May have different goals• Balance
– Aims of treatment – Potential side effects– Inconvenience of medication

Stepwise management of asthma
• Abolish symptoms as soon as possible• Optimise peak flow by starting treatment
at a level to achieve this• Start treatment at a step to achieve
control appropriate to symptoms• Achieve early control• Maintain control
– Step up when necessary– Step down when control is good

Underlying principles of management
Before initiating drug treatment check
– Compliance with existing treatment
– Inhaler technique– Eliminate trigger
factors

Stepwise management


Adults

Step 1
• Short acting bronchodilator– Inhaled SABA– Inhaled ipratropium– Beta agonist tablets or syrup– Theophyllines
• Inhaled SABA works more quickly and/or with fewer side effects


Inhaled steroids
• Should be considered in patients with any of– Exacerbation of asthma in the last 2 years– Using inhaled SABA three times a week or
more– Symptomatic three times a week or more– Waking one night a week

Starting dose of inhaled steroid
• Start at a dose appropriate to severity of disease• Adults – 400 microg BDP a day• Children – 200 microg BDP a day• Children under 5 – may need higher doses if
problems with inconsistent drug delivery• Titrate dose of steroids to the lowest effective
dose
• Dose steroids twice a day

Other preventer therapies
• Inhaled steroids are the first choice– Chromones– LTRA
• Effective in children under 5 unable to take ICS
– Theophyllines
• Antihistamines and ketotifen are ineffective


Add on therapy
• No absolute threshold for introduction of add on therapy
• Addition has been investigated at doses from 200 – 1000mcg BDP in adults and up to 400mcg in children
• Add on therapy should be considered in all patients

Add on therapy
• First choice in adults and children over 5– LABA
• Consider before going above BDP 400mcg/day• Improves lung function and exacerbations• Reduces exacerbations
• Children under 5– LTRA

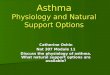
Step 3: Add-on therapyStep 3: Add-on therapyInadequate control on low dose inhaled
steroids
If control still inadequate go to Step 4
Add inhaled long-acting ß2 agonist (LABA)
Benefit from LABA but control still inadequate:• Continue LABA and• Increase inhaled steroid dose to
800mcg/day (adults) and 400mcg/day (children 5-12 years)
Control still inadequate:Trial of other add-on therapy,
e.g. leukotriene receptor antagonist or theophylline
If control still inadequate go to Step 4
Assess control of asthma
No response to LABA:• Stop LABA• Increase inhaled steroid dose
to 800mcg/day (adults) and 400mcg/day (children5-12 years)
Pharmacological management. SIGN 101 May 2008
Good response to LABA:Continue LABA

Regular and as required dosing of combination products• Selected adult patients
– Poorly controlled at step 3– Step 2 above 400mcg/day BDP & poorly controlled– Budesonide/formoterol in a single inhaler– Used as preventer and rescue inhaler– Maintenance dose of ICS should not be reduced
• BUD 200 or 400 mcg twice a day• Patients taking rescue medication once a day or more
should be reviewed• Careful education


Addition of a fourth drug
• ICS (BDP 800mcg) + LABA + SABA– Increase ICS to 2000 mg a day (adults) / 800 mcg a
day (children)– LTRA– Theophylline– Slow release beta agonist
• No controlled trials to indicate best options• Theophyllines and beta agonist tablets have
highest potential for side effects


Step 5
• Refer patients to specialist care – especially children
• Continuous or frequent use of oral steroids
• Small number of patients• Use steroid tablets in the lowest dose
possible

Steroid sparing medication
• Inhaled steroids are the most effective oral steroid sparing drug
• Limited evidence for other asthmatic therapy to reduce oral steroid requirement– If trialled they effectiveness should be assessed at 6
weeks• Immunosuppressants may be given as a
3 week trial• Risks and benefits need to be discussed
with the patient

Adverse effects

Safety of inhaled steroids• Balance of risks and benefits• Steroid warning cards at higher doses• Take other delivery routes into consideration
• Adults– Little evidence that doses <800mcg day cause any
short term side effects except dysphonia or oral candida
– One systematic review – no effect on bone density at doses up to 1mg
– Significance of small biochemical changes in adrenocortical function is unknown

Safety of inhaled steroids
• Children– Monitor height regularly– Use lowest dose possible– Written advice should be given to parents of
children on >800mcg BDP daily– Consider steroid warning card for these
children– Should be under specialist paediatric care

LABA
MHRA report• Review of risks & benefits
• LABA should only be started in patients already taking an ICS

Frequent or continuous oral steroids• Risk of systemic side effects
– Monitor• Blood pressure• Urine or blood sugar• Cholesterol• Bone density• Growth (height and weight) in children• Cataracts in children

Non-pharmacological management

Smoking cessation“Smoking is a custom loathsome to the eye, hateful to the nose, harmful to the brain, dangerous to the lungs, and in the black, stinking fume thereof nearest resembling the horrible Stygian smoke of the pit that is bottomless”
James VI & I (1604)
Current and previous smoking reduces the effect of ICS – may be overcome with increasing doses

Non-pharmacological management
• Lack of evidence for– Allergen avoidance– Nutritional supplements– Immunotherapy– House dust mite avoidance– Air pollution– Dietary manipulation– Acupuncture – Herbal medicines– Physical exercise therapy

Non-pharmacological management
• Some evidence for– Immunotherapy– Avoidance of smoke and other pollutants– Food allergen avoidance– Sub-cutaneous immunotherapy– Weight reduction in obese patients– Buteyko breathing techniques

Pharmaceutical Care

© Imperial College London
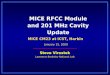
Assessment: Royal College of Assessment: Royal College of Physicians of London three questionsPhysicians of London three questions
Outcomes and audit. Thorax 2003; 58 (Suppl I): i1-i92
• Applies to all patients with asthma aged 16 and over.• Only use after diagnosis has been established.
IN THE LAST WEEK / MONTH
YES NO
“Have you had difficulty sleeping because of your asthma symptoms (including cough)?”
“Have you had your usual asthma symptoms during the day (cough, wheeze, chest tightness or breathlessness)?”
“Has your asthma interfered with your usual activities(e.g. housework, work, school, etc)?”
Date / / /

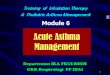
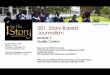
1.1. In the past 4 weeks, how much of the time did your asthma keep you from getting as much done at work, school or In the past 4 weeks, how much of the time did your asthma keep you from getting as much done at work, school or at home?at home?
2.2. During the past 4 weeks, how often have you had shortness During the past 4 weeks, how often have you had shortness of breath?of breath?
3.3. During the past 4 weeks, how often did your asthma symptoms (wheezing, coughing, shortness of breath, During the past 4 weeks, how often did your asthma symptoms (wheezing, coughing, shortness of breath, chest tightness or pain) wake you up at night, or earlier than usual in the morning?chest tightness or pain) wake you up at night, or earlier than usual in the morning?
4.4. During the past 4 weeks, how often have you used your rescue During the past 4 weeks, how often have you used your rescue inhaler or nebulizer medication (such as salbutamol)?inhaler or nebulizer medication (such as salbutamol)?
5.5. How would you rate your asthma control during the past How would you rate your asthma control during the past 4 weeks?4 weeks?
ScoreScore
Patient Total ScorePatient Total ScoreCopyright 2002, QualityMetric Incorporated.Copyright 2002, QualityMetric Incorporated.Asthma Control Test Is a Trademark of QualityMetric Incorporated.Asthma Control Test Is a Trademark of QualityMetric Incorporated.
Asthma Control Test™ (ACT)