Embed Size (px)
Citation preview
Assessment of CAP Severity
by Pneumonia Scores
Gamal Rabie Agmy, MD, FCCP Professor of Chest Diseases , Assiut University

Pneumonia
Scores

Clinical prediction rule recommended
by the British Thoracic Society that has
been validated for predicting mortality
in community acquired pneumonia and
therefore helps predict inpatient vs
outpatient treatment.
CURB-65

Each risk factor scores one point with a
maximum score of 5.
Confusion of new onset
Urea > 7 mmol/L
Respiratory rate >30/min or greater
Blood pressure <90 mmHg systolic or <65
mmHg diastolic
Age >65 years
CURB-65

The risk of death at 30 days increases as
the score increases:
0 - 0.7%
1 - 3.2%
2 - 13.0%
3 - 17.0%
4 - 41.5%
5 - 57.0%
CURB-65

Disposition recommendations based on
score:
0-1: Treat as an outpatient
2-3: Consider a short stay in hospital or
watch very closely as an outpatient
4-5: Requires hospitalization, consider ICU
admission
CURB-65

7
CURB 65 Rule – Management of CAP
CURB 65
Confusion
BUN > 30
RR > 30
BP SBP <90
DBP <60
Age > 65
CURB 0 or 1 Home Rx
CURB 2 Short Hosp
CURB 3 Medical Ward
CURB 4 or 5 ICU care

Each risk factor scores one point with a
maximum score of 4.
Confusion of new onset
Respiratory rate >30/min or greater
Blood pressure <90 mmHg systolic or <65
mmHg diastolic
Age >65 years
CRB-65

9
CRB 65 Rule – Management of CAP
CRB 65
Confusion
RR > 30
BP SBP <90
DBP <60
Age > 65
CRB 0 or 1 Home Rx
CRB 2 Short Hosp
CRB 3 Medical
Ward
CRB 4 ICU care

Each risk factor scores one point with a
maximum score of 8.
Confusion of new onset
Urea > 7 mmol/L
Respiratory rate >30/min or greater
Blood pressure <90 mmHg systolic or <65
mmHg diastolic
Age >65 years
LDH > 230 u/L
Albumin <3.5 g/dL
Platelet count <100 × 109/L
Expanded CURB-65

The expanded-CURB-65 score was
categorized into three classes as follows:
0–2 as low risk, 3–4 intermediate risk, and
5–8 high risk. Accordingly, patients with
one of three tiers of scores should be
treated either as outpatient, or inpatients in
hospital ward or ICU, respectively.
Expanded CURB-65

0–2 2.57% mortality
3–4 14.89% mortality
5–8 41.76% mortality
Expanded CURB-65

This is a more complex scoring system
which stratifies patients into low, moderate
or high risk, advocating outpatient
treatment for those in the low risk group.
Pneumonia Severity Index (PSI)

A patient can only be in the low risk group if they
satisfy the following criteria:
1-Age >50,
2-No malignancy, CCF, cerebrovascular, renal or
liver disease,
3-Normal mental state,
4-Satisfactory vital signs: HR<125, RR <30,
systolic BP >90 mmHg, temp 35-40C
Pneumonia Severity Index (PSI)

15
PORT Scoring – PSI
Clinical Parameter Scoring
Age in years Example
For Men (Age in yrs) 50
For Women (Age -10) (50-10)
NH Resident 10 points
Co-morbid Illnesses
Neoplasia 30 points
Liver Disease 20 points
CHF 10 points
CVD 10 points
Renal Disease (CKD) 10 points
Clinical Parameter Scoring
Clinical Findings
Altered Sensorium 20 points
Respiratory Rate > 30 20 points
SBP < 90 mm 20 points
Temp < 350 C or > 400 C 15 points
Pulse > 125 per min 10 points
Investigation Findings
Arterial pH < 7.35 30 points
BUN > 30 20 points
Serum Na < 130 20 points
Hematocrit < 30% 10 points
Blood Glucose > 250 10 points
Pa O2 10 points
X Ray e/o Pleural Effusion 10 points
Pneumonia Patient Outcomes
Research Team (PORT)
16
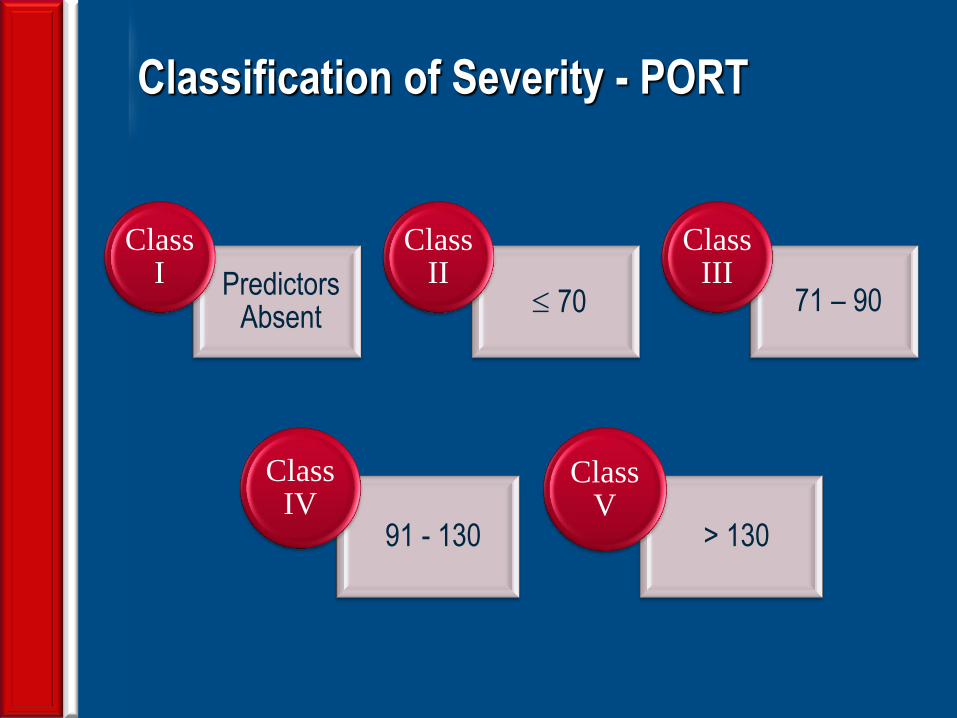
Classification of Severity - PORT
Predictors Absent
Class I
70
Class II
71 – 90
Class III
91 - 130
Class IV
> 130
Class V
17
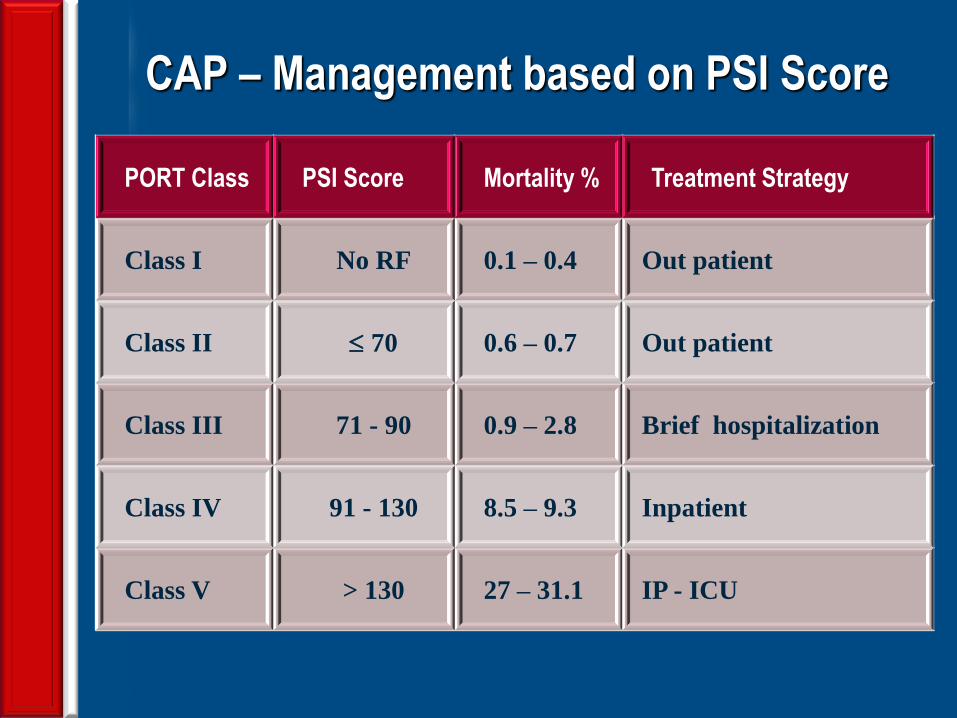
CAP – Management based on PSI Score
PORT Class PSI Score Mortality % Treatment Strategy
Class I No RF 0.1 – 0.4 Out patient
Class II 70 0.6 – 0.7 Out patient
Class III 71 - 90 0.9 – 2.8 Brief hospitalization
Class IV 91 - 130 8.5 – 9.3 Inpatient
Class V > 130 27 – 31.1 IP - ICU

Recent Australian studies have developed
severity scoring systems (eg CORB,
SMART-COP) that are based on predictors
of requirement for intensive respiratory or
inotrope support, in addition to
mortality. The CORB score is simpler and
does not rely on investigation results
however it is less sensitive than SMART-
COP.
CORB and SMART-COP

Confusion (acute)
Oxygen saturation 90% or less
Respiratory rate > 30 breaths per minute
Blood pressure < 90 mm Hg (systolic) or <
60 mm Hg (diastolic)
'Severe CAP' is defined as the presence
of at least two of these features and has a
sensitivity of 81% and specificity of 68%
for predicting need for IRVS.
CORB

SMART-COP

SMART-COP
Interpretation of SMART-COP score:
0 to 2 points—low risk of needing intensive
respiratory or vasopressor support (IRVS)
3 to 4 points—moderate risk (1 in 8) of needing
IRVS
5 to 6 points—high risk (1 in 3) of needing
IRVS
7 or more points—very high risk (2 in 3) of
needing IRVS
Severe CAP = a SMART-COP score of 5 or
more points

SMART-COP
0–2 5.48 % mortality
3–4 22.75 % mortality
5–8 60.87 % mortality

A-DROP
It was developed in Japan
Age, Dehydration, Respiratory failure,
Orientation disturbance, Systolic blood
pressure.
0-1 Low risk Home treatment
2 Intermediate risk Hospitalization
3-5 High risk ICU admission

A-DROP
0–1 4.76 % mortality
2 16.07 % mortality
3-5 41.77 % mortality

Indications for admitting CAP patients to ICU
Major Criteria(1/2 sufficient)
• Acute respiratory failure(mechanical ventilation)
• Severe sepsis or septic shock(need of vasopressors)
Minor Criteria (ICU admission
recommended if ≥3) • Respiration rate ≥ 30/min • Multi lobar involvement
• PaO2:FiO2 ≤250 +/-SaO2 <90% with 6 L O2
• Confusion/ disorientation • Uremia BUN ≥20 mg/dl
• Leukopenia WBC < 4 x 109/L
• Thrombocytopenia Tc < 100.000 / mm3
• Hypothermia core temp< 36°
• Hypotension requiring aggressive fluid resuscitation






























