Embed Size (px)
Citation preview

Histopathologic Evaluation of High Grade Brain Tumors Infiltration Using High Order Diffusion Tensor Imaging
T. Stefani, B. Pereira, A. Coste, T. Khalil, E. Chabert, J.L. Kemeny, L. Boyer, B. Jean.
eP-72 University Hospital, Neuroradiology Dept. 58 rue Montalembert, 63003 Clermont-Ferrand, FRANCE Email: [email protected]

Summary • 1 Purpose • 2 Materials and Methods • 3 Results • 4 Discussion
• 5 Conclusion
• 6 Bibliography
The authors of this study have no conflict of interest to disclose.

1 Purpose • Delineation of high grade brain tumors is critical for treatment
planning, follow up and prognosis. Diffusion Weighted Imaging is widely used in neuro oncology for this purpose [1-3].
• High grade brain tumors are heterogeneous and infiltrative lesions. Tumoral cell dissemination is known to be found beyond from the tumor visible margins therefore analysis of the Brain Adjacent to Tumor (BAT) remains challenging with conventional MRI sequences [4].
• Diffusion Tensor Imaging (DTI) is sensitive to changes in white matter fiber bundles microstructure [8].
• The aim of this study was to evaluate the peripheral white matter infiltration of high grade brain tumors using high order Diffusion Tensor Imaging.

2 Materials and Methods • Monocentric prospective study, from April 2012 to April 2013. • Local IRB approval and informed consent from all patients were obtained. • All patients from 18 to 85 years of age having a suspected cerebral high grade tumor
(WHO III-IV) on CT scans were screened to be included the protocol. • Exclusion criteria: MRI contraindication, severe renal failure, cerebral biopsy
contraindication, pregnancy.
Total Total 17 patients screened
Included Included 7 patients
Biopsy Refusal Biopsy Refusal 2 patients
Post-CT Surgical Post-CT Surgical Treatment 3 patients
Not WHO III-IV Not WHO III-IV 5 patients
(1 WHO II, 2 metastasis, 1 lymphoma,
1 atypical meningioma)
Biopsy Biopsy 12 patients
Diffusion Tensor MRI Diffusion Tensor MRI 14 patients
excluded
excluded
excluded

2 Materials and Methods
• Seven patients were prospectively included and underwent 3 T clinical MRI scans (Signa MR750, GE Medical Systems, Milwaukee, Wis). – Usual diagnostic MRI protocol included :
• 3D-T1GE (Repetition Time (TR) 8.8 ms, Echo Time (TE) 3.54 ms, 1x1x1.2mm3) before and after contrast media injection
• T2-SE (TR 4923 ms, TE 100.23 ms, 1x1x4mm3)
• Diffusion (TR 8500 ms, TE minimum, 1x1x2mm3, b0-b500-b1000 s/mm2)
• T2 FLAIR (TR 11000 ms, TE 142.97 ms, Inversion Time (TI) 2350 ms, 1x1x4mm3)
• Perfusion Weighted (Echo Planar Imagine (EPI), TR 2000 ms, TE 14.4 ms, 2x2x4mm3)
• Multivoxel Spectroscopy (Point Resolved Spectroscopy (PRESS), TE 144 ms and TE 35ms, 2x2x2cm3)
– Diffusion Tensor Sequence : • Diffusion Tensor Imaging 20 directions (EPI, TR 8000, TE minimum,
1x1x2mm3, b0-b1000 s/mm2, sequence duration: 8 minutes).
• Diffusion Tensor Imaging 60 directions (EPI, TR 8000, TE minimum, 1x1x2mm3, b0-b3000 s/mm2 sequence duration: 16 minutes).
• The 20 directions sequence was done prior to the 60 directions sequence to decrease the probability of bad sequences associated with motion artifacts, or premature termination of examination.

2 Materials and Methods
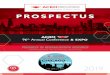
• Patients then underwent surgical CT guided stereotactic tumor biopsy targeted with Leksell frame (Iplan Stereotaxy 3.0.2,Brainlab), according to standard procedure, maximum 1 week after MRI procedure (mean delay = 4 days).
• An extra biopsy (10mm length, 1mm diameter) was performed in normal-appearing white matter adjacent to the tumor along the biopsy pathway 3 to 8 mm away from the enhancement area.
• The coordinates of the center of the biopsy window were noted.
Fig. 1. CT guided stereotactic biopsy planning. Target is located along
the biopsy pathway, 3 to 4 mm away from the enhancement area.

2 Materials and Methods • Biopsies were fixed with formaldehyde. • Histopathologic analysis :
– WHO classification of the tumor.
• Using immunohistochemical markers : – MAP2 (microtubule associated protein 2), Ki67.
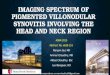
• Semi quantitative estimation of tumor infiltration percentage (IP): – Number of atypical cells / Total number of cells in the field of view. – (Field 1mm x 2mm, Magnification x10).
Fig. 2. Brain adjacent to tumor biopsy sample, field
1x2mm, magnification 10. Ki67 immunologic marker
showing moderate proliferative rate.

2 Materials and Methods
• Analysis of DT-MRI datasets was done using in-house software using MATLAB scripts (R2012a.
Natick, Massachusetts: The MathWorks Inc) courtesy of Angelos Barmpoutis, PhD [5].
– Fourth order tensor resolution :
• 9 x 9 Matrix diagonalisation : 6 Eigenvalues i 6 Eigenvectors Ui
Fig. 3. Fourth order tensor and its eigenvalues/vectors orientation distribution
fonction (ODF).

2 Materials and Methods – Computation of the tensor scalars [6], at the biopsy locus (MRI and biopsy CT images
coregistration, 1x1x1mm3 precision, EPI spatial distortions correction using Iplan Stereotaxy 3.0.2,Brainlab) • GA (Generalized Anisotropy)
• GV (Variance)
• MD (Mean Diffusion)
with
Fig. 4. Fourth order tensor scalar computation at the biopsy
locus (blue dot).

2 Materials and Methods
• Statistical analysis (Spearman’s rank correlation) was done using STATA 10.0 (Stata Corporation, College Station, TX, USA). – 30 subjects needed (risk = 5%, statistical power = 90%).
• Primary analysis: – Correlation coefficient was evaluated between the 4th order diffusion Generalized
Anisotropy (GA) distribution and the tumor infiltration percentage (TI).
• Secondary analysis:
– Correlation coefficient was evaluated between the 4th order diffusion tensor metrics
distributions (GV, MD) and the tumor infiltration percentage.

3 Results
• 7 prospective patients (3M, 4F).
• Age ranging from 52 to 86 year old (mean age value = 63).
• Homogeneous population of glioblastoma multiforme (GBM).
• Tumor Infiltration Percentage (TI) values : – Mean TI value= 0.16 [0;1].
• Tensor scalars mean values: – GA (biopsy) = 0.36 [0.18;0.68].
– GV (biopsy)= 0.0028 [0.0009;0.0086].
– MD (biopsy)= 0.00065 [0.00035;0.00075].

3 Results
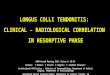
• We observed a significant correlation between :
– GA and tumor infiltration percentage (TI) (r=-0.98 p=0.006).
– GV and tumor infiltration percentage (TI) (r=-0.98 p=0.006).
• MD showed no significant correlation (r=0.11 p=0.76) with TI.
Fig. 5. GA maps.
Left: (patient number: 03) Right frontoparietal
glioblastoma showing low GA signal in a
peripheral ROI (red arrow) and 0% TI on
histology.
Right: (patient number: 07) Left parietal
glioblastoma showing high GA signal in a
peripheral ROI (yellow arrow) and an 10% TI
on histology.

4 Discussion • In this study we introduced 4th order diffusion tensor which offers an
alternative model to conventionnal 2nd order tensor (3 x 3 matrix). – Jayachandra et al [7], showed that anisotropy could be estimated more accurately for
complex microstructure with 4th order DTI compared to 2nd order DTI.
– Simpler modelisation compared to other techniques (Qball, High Angular Resolution DTI).
• Provenzale et al [8] showed that there is a significant difference in Fractional Anisotropy (FA) decrease for peritumoral NAWM between gliomas and meningiomas but not for peritumoral regions (hyperintense areas on T2-weighted MR images), showing that DTI may be sensitive to subtle microstructure changes.
• Stadlbauer et al [9] showed FA is better than MD for assessment and delineation of different degrees of pathologic changes (ie, TI) in glioma but their retrospective population was heterogeneous (WHO Grade II and III gliomas).
• Ellingson et al [10] showed limitations of conventional 2nd order DTI compared to 4th order DTI when evaluating glioblastomas but needed careful tissue validation as they didn’t correlate their results to a biopsy with cell quantification.

4 Discussion
• In our study we showed that GA and GV were significatively correlated to Tumor Infiltration Percentage in glioblastoma.
• But this study has some limitations: – Few subjects : only 7 patients (this study is still recruiting).
– Non fixed distance from tumor to biopsy due to surgeon target choice.
– Semi quantitative estimation of percentage infiltration.
– Coregistration accuracy: 1mm accuracy (3mm diameter ROI and correction of EPI spatial distortions)
– 60 directions GA maps have a lower signal to noise ratio (SNR) compared to 20 directions sequence.

5 Conclusion
•These preliminary results despite the little number of inclusions, show that GA and GV measurements derived from high order diffusion tensor estimation are correlated (p=0.006, p=0.006) to tumor infiltration percentage of the local environment of glioblastoma.
GA derived from fourth order diffusion tensor could be used for assessment and delineation of different degrees of pathologic changes (ie, Tumor Infiltration Percentage) in glioblastoma.
•These results need to be confirmed at the end of the inclusion plan (30 patients completed with DTI and biopsy) in order to validate a clinical non invasive method to delineate real infiltration margins of GBM without the use of extra biopsy in the vicinity of high grade gliomas.

• 1. Chenevert, T.L., and al., Diffusion magnetic resonance imaging: an early surrogate marker of therapeutic efficacy in brain tumors. J Natl Cancer Inst, 2000. 92(24): p. 2029-36.
• 2. Khayal, I.S., and al., Evaluation of diffusion parameters as early biomarkers of disease progression in glioblastoma multiforme. Neuro Oncol, 2010. 12(9): p. 908-16.
• 3. Gerstner, E.R., and al., Infiltrative patterns of glioblastoma spread detected via diffusion MRI after treatment with cediranib. Neuro Oncol, 2010. 12(5): p. 466-72.
• 4. Hayat, M.A., Growth of Malignant Gliomas In Vivo: High-Resolution Diffusion Tensor Magnetic Resonance Imaging in Tumors of the Central Nervous System, Volume 4. 2012, Springer Science.
• 5. Barmpoutis A., and al., Symmetric positive 4th order tensors & their estimation from diffusion weighted MRI. Inf Process Med Imaging 2007; 20:308–319.
• 6. Ozarslan, E., B.C. Vemuri, and T.H. Mareci, Generalized scalar measures for diffusion MRI using trace, variance, and entropy. Magn Reson Med, 2005. 53(4): p. 866-76.
• 7. Jayachandra, M.R., et al., Fiber tracking of human brain using fourth-order tensor and high angular resolution diffusion imaging. Magn Reson Med, 2008. 60(5): p. 1207-17.
• 8. Provenzale, J.M., et al., Peritumoral brain regions in gliomas and meningiomas: investigation with isotropic diffusion-weighted MR imaging and diffusion-tensor MR imaging. Radiology, 2004. 232(2): p. 451-60.
• 9. Stadlbauer, A., et al., Gliomas: histopathologic evaluation of changes in directionality and magnitude of water diffusion at diffusion-tensor MR imaging. Radiology, 2006. 240(3): p. 803-10.
• 10. Ellingson, B.M., et al., High order diffusion tensor imaging in human glioblastoma. Acad Radiol, 2011. 18(8): p. 947-54.
6 Bibliography