Embed Size (px)
Citation preview
Arthroscopic Repair
Peter J. Millett, MD, MScDirector of Shoulder Surgery
The Steadman ClinicVail, CO
AANA/AOSSM/ASES Specialty Day
March 28, 2015
Las Vegas, Nevada
Disclosures
Peter J. Millett, MD, MScRelevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within this presentation are as follows:
Consultant and Royalties: Arthrex, Inc.
Consultant: Myos
Stock and Stock Options: GameReady, VuMedi
Research activities supported by the Steadman Philippon Research Institute (SPRI).
Corporate sponsorships for SPRI : Smith & Nephew, Arthrex, Siemens, Össur
Case Presentation
• 48 y/o M overhead worker
• Increasing pain
• Supraspinatus tear with Grade 2
atrophy and acute infraspinatus tear
–Treatment???
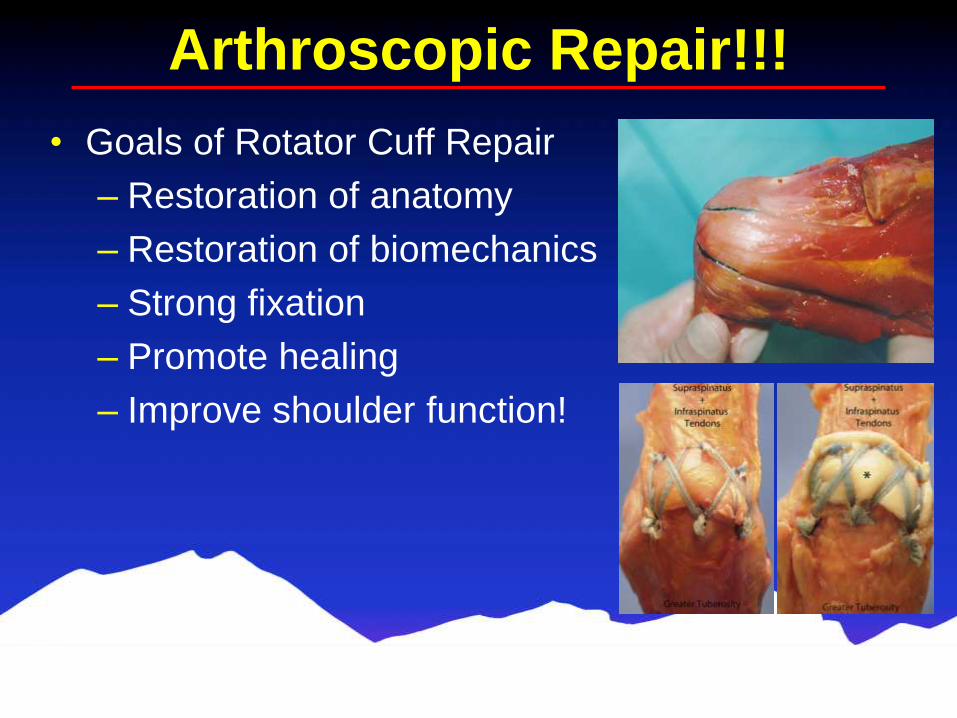
Arthroscopic Repair!!!
• Goals of Rotator Cuff Repair
– Restoration of anatomy
– Restoration of biomechanics
– Strong fixation
– Promote healing
– Improve shoulder function!
Arthroscopic Repair!!!
• Advantages
–Address concomitant pathologies
• SLAP, biceps pathology etc..
–Lower complication rates than RTSA
and tendon transfer
– Improved functional outcomes
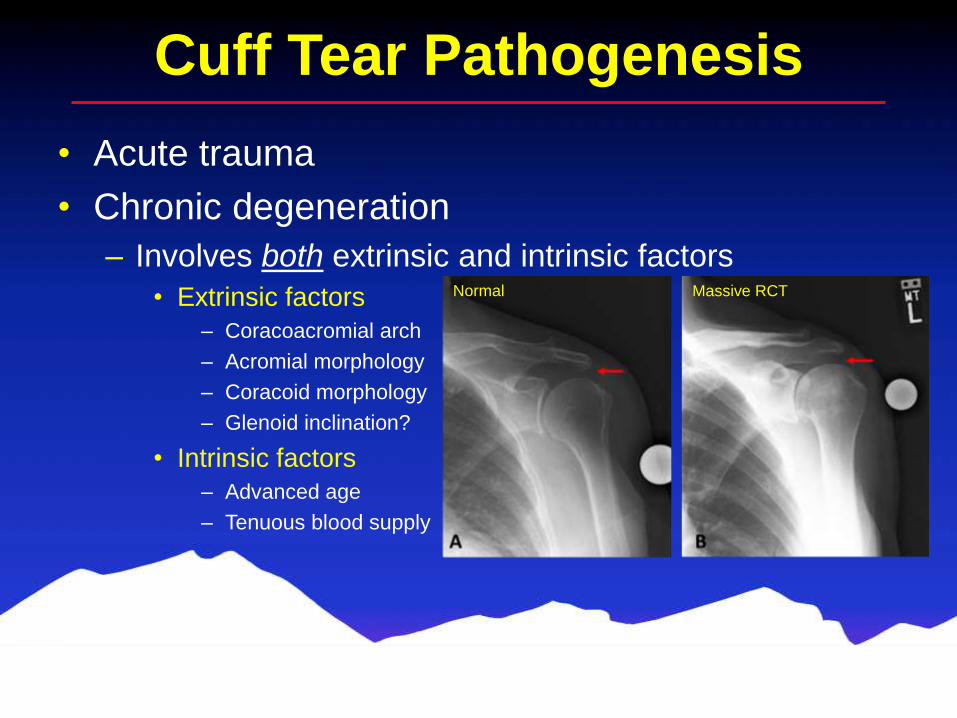
Cuff Tear Pathogenesis
• Acute trauma
• Chronic degeneration
– Involves both extrinsic and intrinsic factors
• Extrinsic factors
– Coracoacromial arch
– Acromial morphology
– Coracoid morphology
– Glenoid inclination?
• Intrinsic factors
– Advanced age
– Tenuous blood supply
Normal Massive RCT
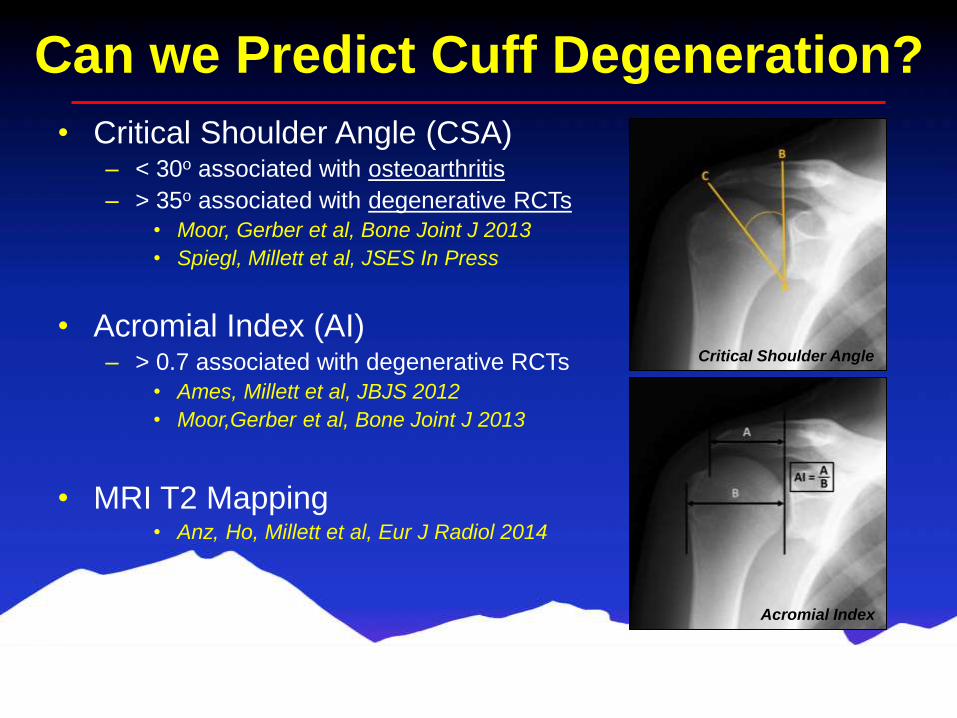
Can we Predict Cuff Degeneration?
• Critical Shoulder Angle (CSA)– < 30o associated with osteoarthritis
– > 35o associated with degenerative RCTs
• Moor, Gerber et al, Bone Joint J 2013
• Spiegl, Millett et al, JSES In Press
• Acromial Index (AI)– > 0.7 associated with degenerative RCTs
• Ames, Millett et al, JBJS 2012
• Moor,Gerber et al, Bone Joint J 2013
• MRI T2 Mapping• Anz, Ho, Millett et al, Eur J Radiol 2014
Critical Shoulder Angle
Acromial Index
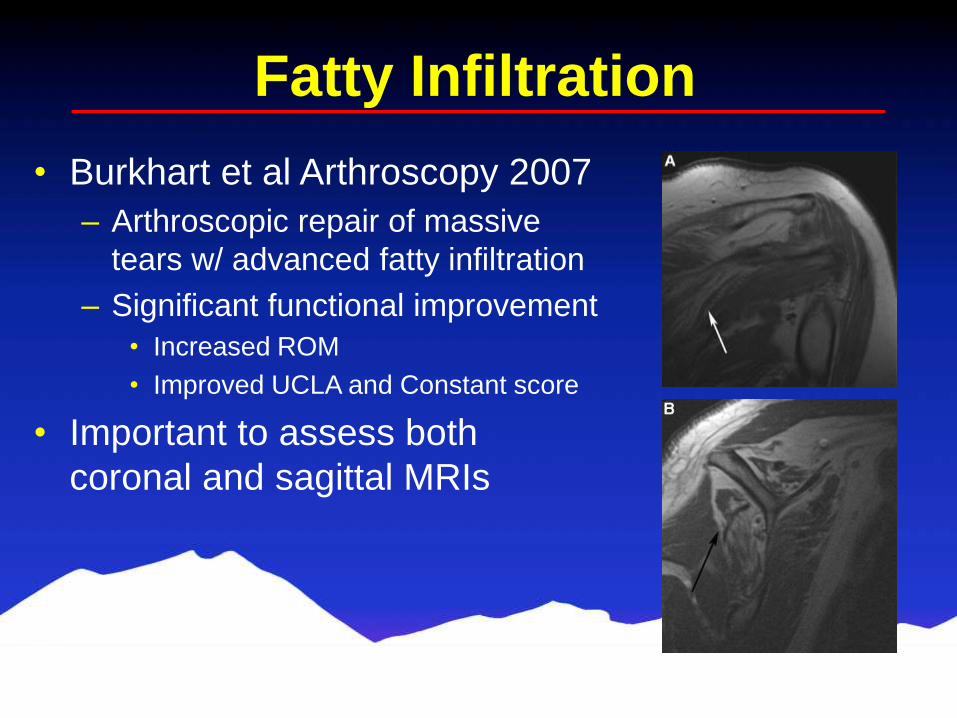
Fatty Infiltration
• Burkhart et al Arthroscopy 2007
– Arthroscopic repair of massive
tears w/ advanced fatty infiltration
– Significant functional improvement
• Increased ROM
• Improved UCLA and Constant score
• Important to assess both
coronal and sagittal MRIs
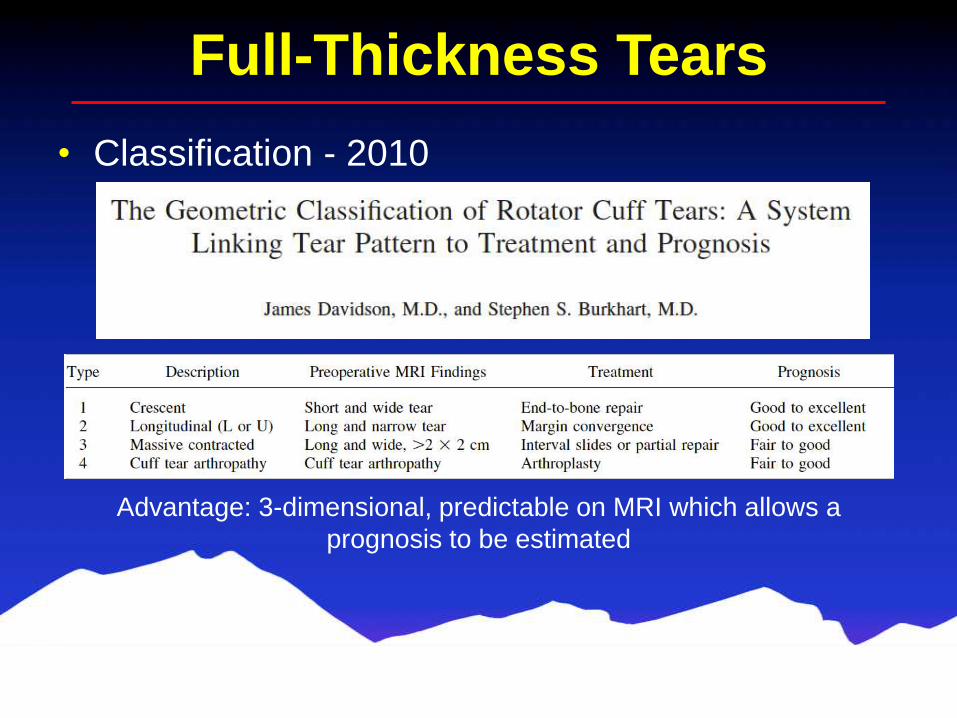
Full-Thickness Tears
Advantage: 3-dimensional, predictable on MRI which allows a
prognosis to be estimated
• Classification - 2010
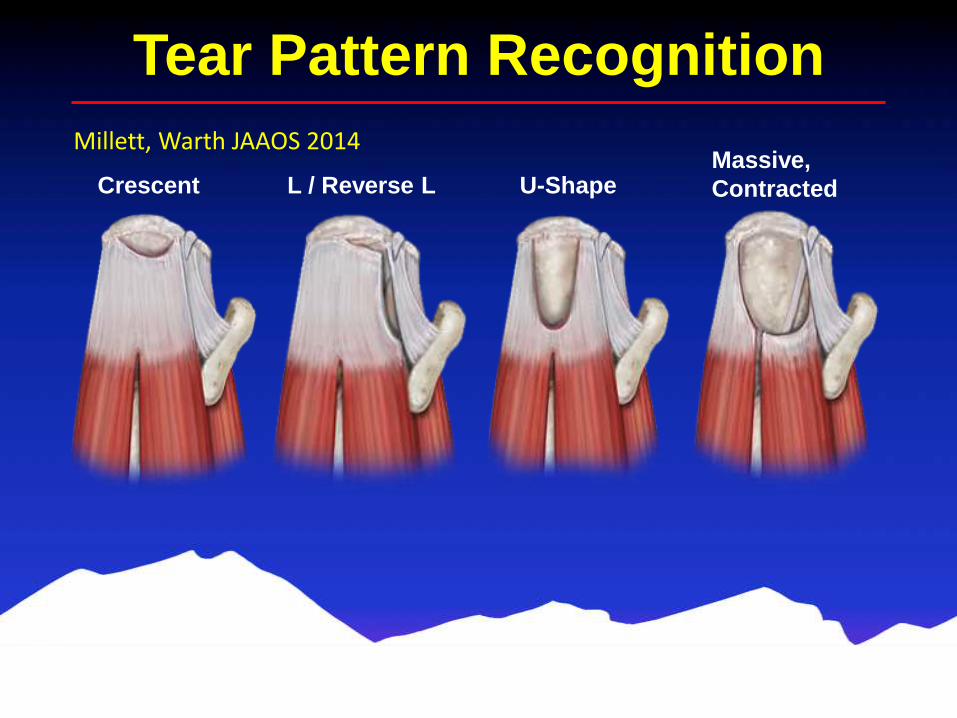
Tear Pattern Recognition
Crescent L / Reverse L U-ShapeMassive,
Contracted
Millett, Warth JAAOS 2014
Importance of Tear Patterns
• Three-dimensional tear pattern recognition is
required for modern arthroscopic rotator cuff
repair…
– Facilitates anatomic restoration
– Optimizes biomechanical properties
– Optimizes tendon biology
– Decreases failure rate
– Improves clinical outcomes!
Extended Speedbridge
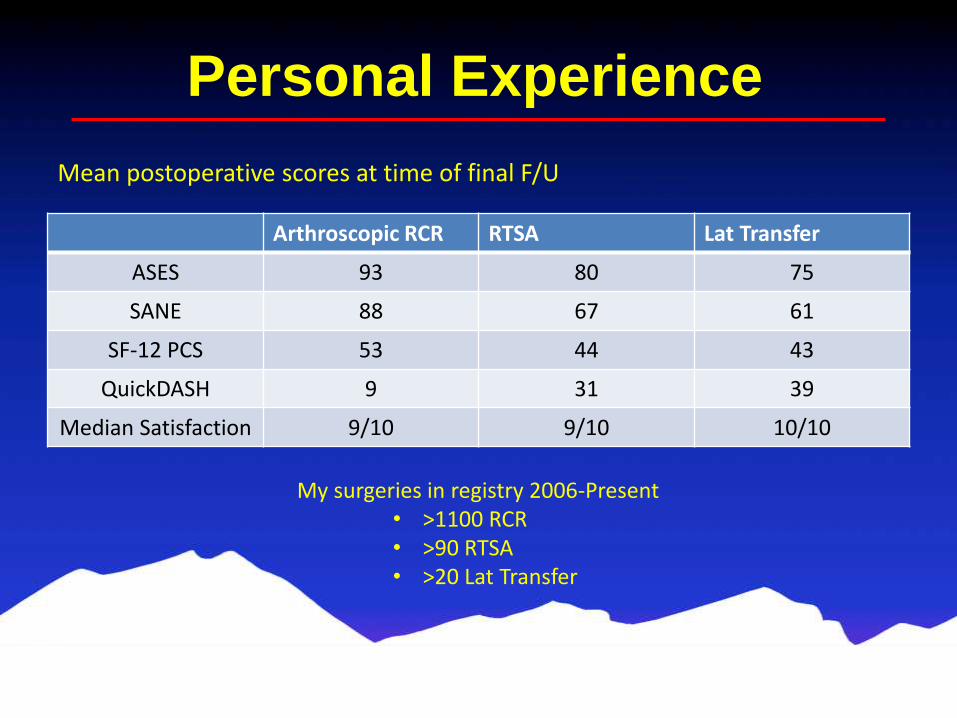
Personal Experience
Arthroscopic RCR RTSA Lat Transfer
ASES 93 80 75
SANE 88 67 61
SF-12 PCS 53 44 43
QuickDASH 9 31 39
Median Satisfaction 9/10 9/10 10/10
Mean postoperative scores at time of final F/U
My surgeries in registry 2006-Present• >1100 RCR• >90 RTSA• >20 Lat Transfer
2 Years s/p Repair of Massive Tear
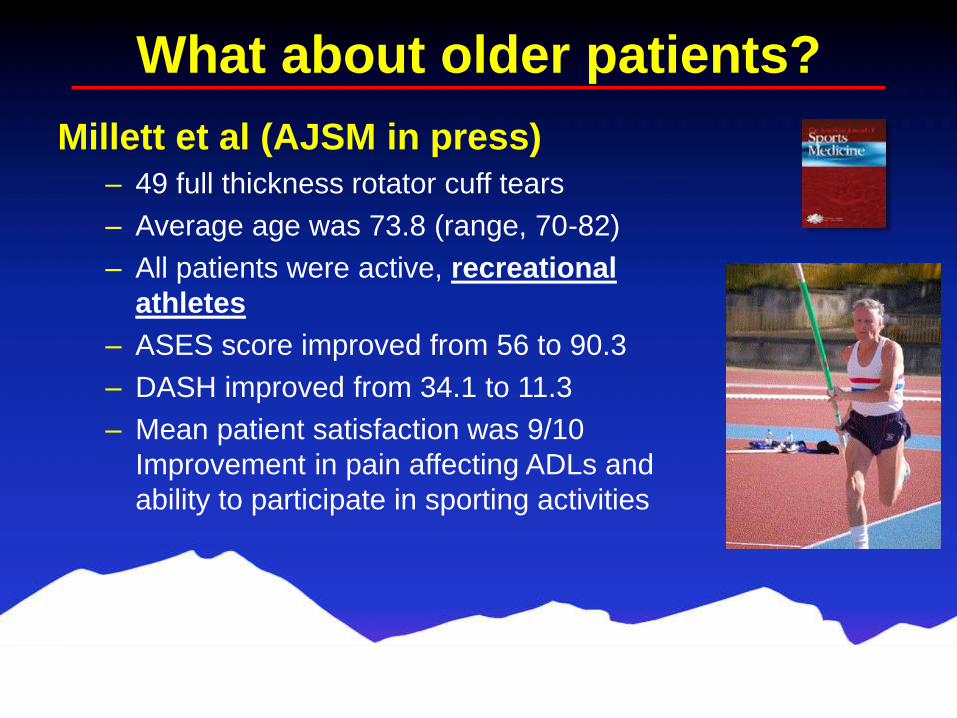
What about older patients?
Millett et al (AJSM in press)
– 49 full thickness rotator cuff tears
– Average age was 73.8 (range, 70-82)
– All patients were active, recreational
athletes
– ASES score improved from 56 to 90.3
– DASH improved from 34.1 to 11.3
– Mean patient satisfaction was 9/10
Improvement in pain affecting ADLs and
ability to participate in sporting activities
Conclusions
• Arthroscopic RCR is the best option in this
patient
• Proven to improve function and decrease
pain, even in the elderly
• Low complication rates

Thank you!!