Embed Size (px)
Citation preview

Acute Respiratory Distress Acute Respiratory Distress Syndrome (ARDS)Syndrome (ARDS)
Yuan Zhiming Department of Emergency Medicine
The General Hospital
Tianjin Medical University

● General Considerations
● Etiology
● Pathogenesis
● Pathophysiology
● Pathology
● Clinical Presentation
● Diagnosis
● Treatment
● Prognosis
Contents


Respiration
ventilation
diffusion
circulation
oxygen extraction and utilization
(1)(1)
(2)(2)
(3)(3)
(4)(4)

General considerations
Definitions Retrospect Incidence

ARDS denotes acute hypoxemic respiratory failure following a systemic or pulmonary insult without evidence of heart failure. It is the most severe form of acute lung injury(ALI) and is characterized by bilateral, widespread radiographic pulmonary infiltrates, normal pulmonary capillary wedge pressure (PCWP) (<18 mmHg) and Pa02/Fi02 < 200 mmHg .
Definitions

ALI is a syndrome of inflammation and increased permeability that is associated with a constellation of clinical, radiologic, and physiologic abnormalities that cannot be explained by, but may coexist with, left atrial or pulmonary capillary hypertension.
Exclusion of left atrial hypertension as the primary cause of hypoxemia is critical to this definition

The distinction between ALI and ARDS is the degree of hypoxemia
ALI: Pa02/Fi02 < 300 mmHg ARDS: Pa02/Fi02 < 200 mmHg

Retrospect ARDS was first reported by Ashbaugh in 1967.
Petty and Ashbaugh renamed it as adult respiratory distress syndrome in 1971 in order to distinguish them from neonate respiratory distress syndrome.
The American-European Consensus Committee on ARDS standardized the definition in 1994 and renamed it acute rather than adult respiratory distress syndrome because it occurs at all ages.

Incidence
Incidence : 12.6 to 18 per 100,000 persons annually
Controversy still exists about the correct incidence because of differing criteria used to define ARDS

Risk Factors (common)
Direct lung injuryPneumoniaAspiration of gastric contentsInhalation injury Near drowning Lung contusion Fat embolism
Indirect lung injurySepsis ShockSevere traumaAcute pancreatitis Massive transfusionsCardiopulmonary bypassDrug overdose

PathogenesisThe pathogenesis of ARDS is not well known The pathogenesis of ARDS is not well known
inflammatory cells stimulated
damage of capillary endothelial cells and alveolar epithelial cells
vascular permeability surfactant
interstitial and alveolar pulmonary edema
risk factors
pro-inflammatory cytokines and mediators released
hypoxemia
alveolar collapse

Pathophysiology

Pathology
In ARDS, the injured lung go through three phases: exudative, proliferative, and fibrotic, but the course of each phase and the overall disease progression is variable, and the three phases don’t have a definite borderline, they overlap partly.

damage to the alveolar epithelium (type I alveolar cells mainly) and vascular endothelium
Exudative phase(<7d):
leakage of water, protein, and inflammatory and red blood cells into the interstitium and alveolar lumen; producing hyaline membranes

Proliferative phase (1-3wk):
Type II cells proliferate with some epithelial cell regeneration, fibroblastic reaction, and remodeling.
Injury to the surfactant-producing type II cells alveolar collapse

Fibrotic phase ( > 3wk):
Collagen deposition in alveolar, vascular, and interstitial beds with development of microcysts.

Nondescript very heavy and poorly aerated lungs. Each lung in ARDS usually weighs over 1000 grams. (A normal lung weighs 200-300 grams)

Heavy, red lungs showing congestion and edema.

3-4 weeks after onset of ARDS, extensive interstitial fibrosis developed.

Photomicrograph shows ARDS in the exudative stage. Note the hyaline membranes and loss of alveolar epithelium in this early stage.

Photomicrograph shows ARDS in the early proliferative stage. Note the type 2 pneumocytic proliferation, with widening of the septa and interstitial fibroblast proliferation.

Photomicrograph shows ARDS in the late proliferative stage. Note the extensive fibroblast proliferation, with incorporation of the hyaline membranes.

Diffuse Alveolar DamageHyaline membranes are lining the alveolar ducts and alveolar septa.

Clinical Presentation
Rapid onset of profound dyspnea that usually occurs 12-48 h after the initiating event. Labored breathing, tachypnea, intercostal retractions, and crackles. Marked hypoxemia that is refractory to treatment with supplemental oxygen.
Many patients demonstrate multiple organ failure.

Chest radiography:
In nondirect insults, the initial radiograph may be nonspecific or similar to congestive heart failure with mild effusions (interstitial pulmonary edema with diffuse infiltrates); As the disease progresses, the characteristic bilateral diffuse alveolar and reticular opacities become evident.
In patients with direct pulmonary insults, focal changes may be evident early.
Characterized by diffuse or patchy bilateral Characterized by diffuse or patchy bilateral pulmonary infiltratespulmonary infiltrates

Chest radiograph shows an endotracheal tube, left subclavian central venous catheter into the superior vena cava, and bilateral patchy opacities in mostly the middle and lower lung zones.
The patient had been in respiratory failure for 1 week with the diagnosis of ARDS.

chest radiographic findings in a patient with ARDS that evolved over approximately 1 week

chest radiographic findings in a patient with ARDS that evolved over approximately 1 week

CXR shows bilateral opacities suggestive of ARDS.

Typical patterns of ARDS with diffuse internal infiltrates

Early phase of ARDS showing interstitial changes and patchy infiltrates

Late stage of ARDS showing bilateral and diffuse alveolar and reticular opacification

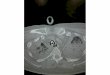
CT scan of the chest showing diffuse infiltrates, ground glass appearance, and air bronchograms.
ARDS

a small right pleural effusion, consolidation with air-bronchograms, and some ground-glass appearing opacities. The findings indicate an alveolar process, in this case, alveolar damage. High-resolution computed tomographic
(HRCT) image in a patient with ARDS

Diagnosis
New, bilateral, diffuse, patchy or homogeneous pulmonary infiltrates on radiograph. Occurring in the appropriate clinical setting with one or more recognized risk factors. Without clinical evidence of heart failure, fluid overload or chronic lung disease (PCWP<18 mmHg). Impaired oxygenation defined as Pa02/Fi02 < 200 mmHg.
In 1994, the American-European Consensus Conference

Treatment
There is no specific therapy for ARDSThere is no specific therapy for ARDS Treatment must include treatment of the underlying precipitating and secondary conditions.
supportive care
mechanical ventilation
pharmacologic treatment

Supportive care
fluid management: maintain PCWP at the lowest level compatible with adequate CO.
nutrition support: preferably administered by the enteral route is recommended .

Mechanical ventilation
Treatment of the hypoxemia usually requires tracheal intubation and positive pressure ventilation. Initial settings commonly used are the assist- control mode with provision of adequate positive end-expiratory pressure (PEEP).
A detailed volume ventilation protocol that employs small tidal volume(<6ml/kg of body weight) resulted in the lowest mortality (31%).

Positive end-expiratory pressure
Advantages: Increases functional residual capacityRecruits additional lung units improving complianceReduces pulmonary shunt fractionAllows for a decrease in FIO2 Can decrease preload in congestive heart failure

Disadvantages:
Increase mean airway pressure leading to reduced venous returnCan increase pulmonary vascular resistance and right-heart dsyfunction Altered renal blood flow with increase in ADH(antidiuretic hormone) release Barotrauma caused by increased pressure

Pharmacologic treatment
Corticosteroids: not indicated in the early course, to use in late-phase might be beneficial .
Antibiotics Stress ulcer and thromboembolic prophylaxis Other drugs: like prostacyclin, nitric oxide, prostaglandins, and receptor antagonists to various cytokines, etc.

Prognosis Mortality rate: greater than 50% between 1979 and 1994, more recent studies show a decline in mortality to be 35%~40%
If ARDS is accompanied by sepsis, the mortality rate may reach 90%. The major causes of death in ARDS are the primary illness and secondary complications such as MODS or sepsis.
Most survivors of ARDS are left with some pulmonary symptoms (cough, dyspnea, sputum production), which tend to improve over time

Summarization ARDS denotes acute hypoxemic respiratory failure following a systemic or pulmonary insult without evidence of HF,and is the most severe form of ALI.
Provision of supplemental oxygen, lung rest, and supportive care are the fundamentals of therapy, endotracheal intubation and mechanical ventilation are frequently required, Timely correction of the inciting clinical condition is essential for preventing further injury.
It is characterized by dyspnea, profound hypoxemia, decreased lung compliance, and diffuse bilateral infiltrates on chest radiography.

Emphases
Definition of ARDS
Pathophysiology
Clinical presentation & diagnosis of ARDS
The principles of treatment of ARDS