Embed Size (px)
Citation preview
APPROACH TO FATIGUE
Raheef Alatassi
5th Year Medical Student
Family Medicine
WHAT IS FATIGUE ??
Definition
• A sensation of exhaustion during or after usual activities, or a feeling of inadequate energy to begin these activities.
• Fatigue can be manifested as difficulty or inability initiating activity (perception of generalized weakness); reduced capacity maintaining activity (easy fatigability); and difficulty with concentration, memory, and emotional stability (mental fatigue).
• Fatigue is defined as the subjective complaint of tiredness or diminished energy level to the point of interfering with normal or usual activities.
Cont.
Duration of fatigue can be:
• Recent (less than one month),
• Prolonged (more than one month)
• Chronic (over six months).
• The presence of chronic fatigue does not necessarily imply the presence of the chronic fatigue syndrome, which is discussed separately.
WHAT IS THE DIFFERENCE BETWEEN FATIGUE,
DYSPNEA AND MUSCLE WEAKNESS ?
What is the difference between Fatigue, dyspnea and muscle weakness ?Dyspnea
A subjective experience of breathing discomfort that is comprised of qualitatively distinct sensations that vary in intensity.
Muscle weakness
A. Primary or true muscle weakness
B. Muscle tiredness (ASTHENIA)
EPIDEMIOLOGY
• A major symptom
• Found in all populations and associated with multiple factors.
• It is one of the top 10 chief complaints leading to family practice office visits
• Fatigue occurs in up to 20% of patients seeking care
• Higher in women than in men.
• Psychiatric illness is present in 60 to 80 % of patients with chronic fatigue.
• The three major psychiatric illnesses were major depression (58 percent), panic disorder (14 percent), and somatization disorder (10 percent).

What is the difference between the CFS, chronic fatigue & idiopathic chronic fatigue?
Type Definition
chronic fatigue syndrome
(Based on CDC 2006)
Clinically evaluated, unexplained, persistent or relapsing fatigue.that is of new or definite onset.is not the result of ongoing exertion;is not alleviated by rest;Cause reduction in previous levels of occupational, educational, social, or personal activities
chronic fatigue The presence of fatigue for longer than six months.
idiopathic chronic fatigue No medical or psychiatric explanation can be found .persists for over six months and is debilitating.but does not meet the criteria for the chronic fatigue syndrome.

ETIOLOGY
• Psychological ?
• Pharmacologic ?
• Endocrine-metabolic ?
• Hematologic ?
• Infectious ?
• Malignancy
• Cardiopulmonary ?
• Disturbed sleep

ETIOLOGY
EVALUATION
• History
• Physical examination
• Laboratory studies
History
• The history is the most important component of the evaluation of chronic fatigue.
• The physical examination and laboratory studies provide supporting data.
• Fatigue that is due to an underlying medical or psychiatric disorder usually presents as one of several reported symptoms.
• The clinician should rely upon open-ended questions ?
• Patients with organ-based medical illness often Associate their fatigue with activities they are unable to complete.
• In contrast, patients with fatigue that is not organ-based are tired all the time; their fatigue is not necessarily related to exertion.
• Nor does it improve with rest.
History
• ID: Age, Gender, Nationality, occupation.
• CC.:
• HPI:
o Onset - abrupt or gradual, related to event or illness?
o Course - stable, improving or worsening?
o Duration and daily pattern
o Factors that alleviate or exacerbate symptoms
o Impact on daily life - ability to work
o Accommodations that patient/family has made to adjust to fatigue symptoms

History
• P.M Hx. ??
• P.S Hx.
• Family Hx.
• Social Hx. ??
• Drug Hx. ???
• Allergy Hx.
• Systemic review
Physical examination
• General appearance: level of alertness, psychomotor agitation or retardation, grooming (psychiatric disorder)
• Presence of lymphadenopathy: a possible sign of chronic infection or malignancy.
• Evidence of thyroid disease: goiter, thyroid nodule, ophthalmologic changes
• Cardiopulmonary examination: signs of congestive heart failure and chronic lung disease
• Neurologic examination: muscle bulk, tone, and strength; deep tendon reflexes; sensory and cranial nerve evaluation
Specific clinical signs of organic disease associated with fatigue include the following:
• Pallor, tachycardia, systolic ejection murmurs: anaemia
• Blue sclera: iron deficiency
• Jaundice, palmar erythema, Dupuytren's contracture: chronic liver disease
• Goitre or thyroid nodule, dry skin, delayed deep tendon reflexes, peri-orbital puffiness, ophthalmological changes: hypothyroidism
• Weight loss, hyper-reflexia, tachycardia, atrial fibrillation, fine tremor, goitre: hyperthyroidism
• Hypotension, pigmentation in skin creases, scars, and buccal mucosa: Addison's disease
• Pulmonary stasis, elevated jugular venous pressure, ankle oedema: heart failure
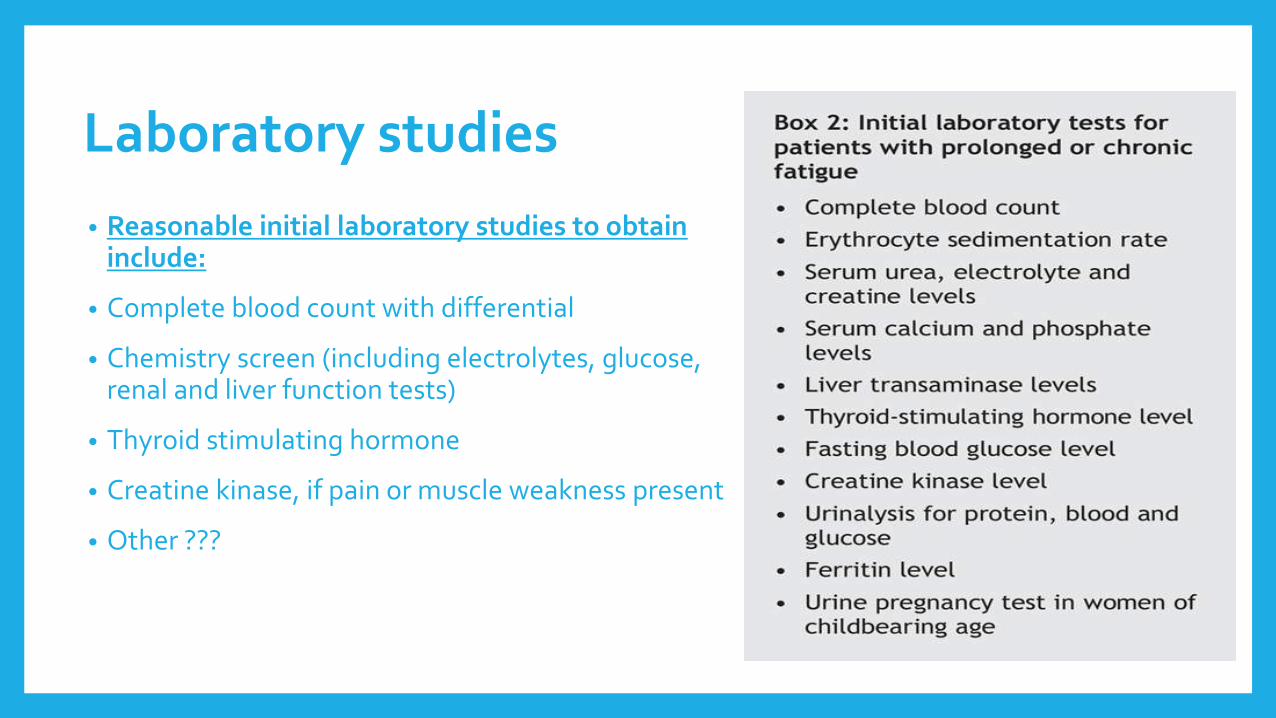
Laboratory studies
• Reasonable initial laboratory studies to obtain include:
• Complete blood count with differential
• Chemistry screen (including electrolytes, glucose, renal and liver function tests)
• Thyroid stimulating hormone
• Creatine kinase, if pain or muscle weakness present
• Other ???
TREATMENT
• The doctor-patient relationship is of profound importance.
The physician will act as a guide in establishing therapeutic goals:
o Accomplishing the activities of daily living
o Returning to work
o Maintaining interpersonal relationships
o Performing some form of daily exercise
• Brief regularly scheduled appointments
TREATMENT
• Treat the underlying cause
• Antidepressants :
patients whose illness has features of depression.
response to antidepressant therapy ????
Antidepressants may themselves provoke or exacerbate fatigue.
• Cognitive behavioral therapy
Is effective in patients with CFS and idiopathic chronic fatigue.
• Graded exercise therapy
Is effective in patients with CFS and idiopathic chronic fatigue.
TREATMENT
Other measures
• Provision of general sleep hygiene advice and discouraging over-sleeping
• Provision of patient education brochures and other materials, discussion of various aspects of chronic fatigue, and referral to support groups
• Iron therapy in non-anemic patients with low serum ferritin may improve symptoms of fatigue
CHRONIC FATIGUE SYNDROME
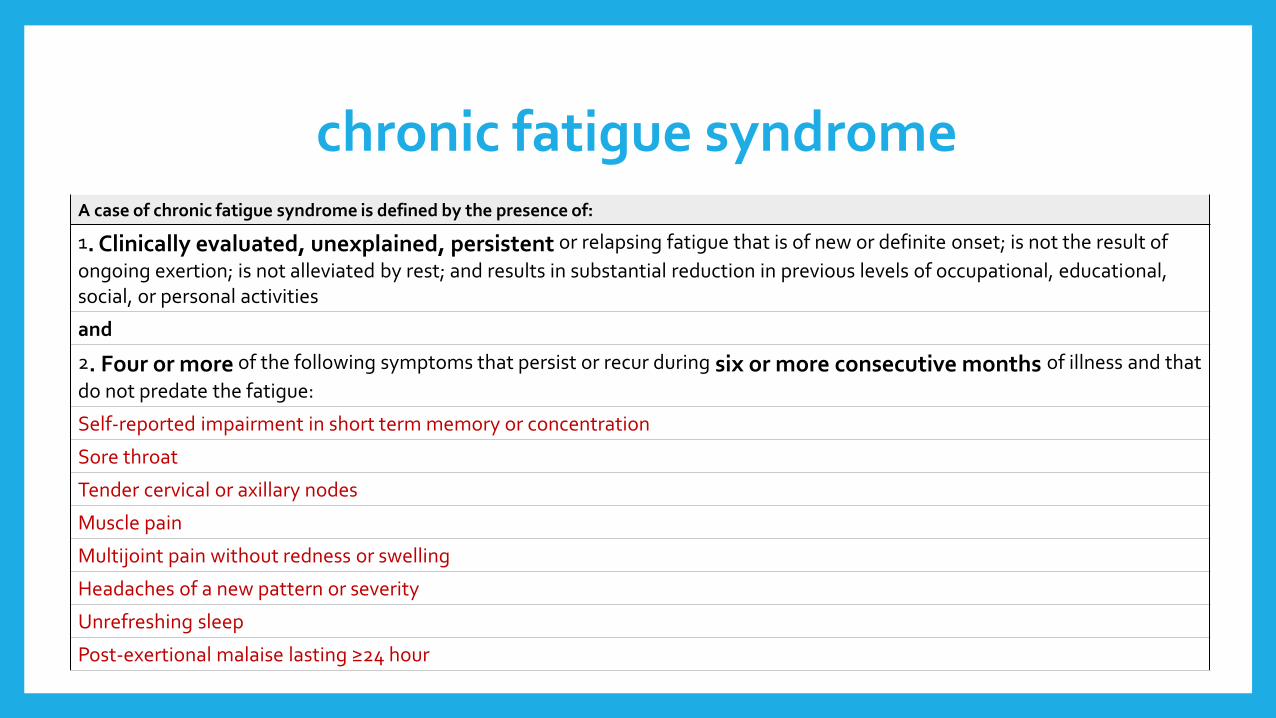
chronic fatigue syndrome A case of chronic fatigue syndrome is defined by the presence of:
1. Clinically evaluated, unexplained, persistent or relapsing fatigue that is of new or definite onset; is not the result of
ongoing exertion; is not alleviated by rest; and results in substantial reduction in previous levels of occupational, educational, social, or personal activities
and
2. Four or more of the following symptoms that persist or recur during six or more consecutive months of illness and that
do not predate the fatigue:
Self-reported impairment in short term memory or concentration
Sore throat
Tender cervical or axillary nodes
Muscle pain
Multijoint pain without redness or swelling
Headaches of a new pattern or severity
Unrefreshing sleep
Post-exertional malaise lasting ≥24 hour
EPIDEMIOLOGY
• Is an extremely common complaint
• Represents a very small subset of those who complain of chronic fatigue < 5%.
• Disorder of young to middle aged adults ( at 30 years)
• CFS is about twice as common in women
• More in Caucasians

ETIOLOGY
• Idiopathic
• Infection
Epstein-Barr virus (EBV), xenotropic murine leukemia related virus (XMRV), and others (retroviruses, human herpesvirus type 6 (HHV-6), enteroviruses, coxsackie B virus)
• Immune dysfunction
• Endocrine-metabolic dysfunction
Low serum cortisol levels, under secretion of corticotropin-releasing hormone, enhanced serum levels of insulin-like growth factor.
• Depression
• Sleep disruption

Clinical presentation
• Sudden onset of fatigue associated with a typical infection such as an upper respiratory infection.
• Altered sleep and cognition.
• Excessive physical activity exacerbates the symptoms
• Numerous other subjective features of CFS fluctuate with time but do not appear to progress
• Once the inciting illness (if any) is resolved, the physical examination typically is normal
SymptomPercent
of patients
Easy fatiguability 100
Difficulty concentrating 90
Headache 90
Sore throat 85
Tender lymph nodes 80
Muscle aches 80
Joint aches 75
Feverishness 75
Diagnosis
• History
• Physical examination
• Laboratory testing
• The diagnosis of CFS is one of exclusion
It is generally made if the patient has a typical history, and no abnormality can be detected on physical examination or in the screening tests.
TREATMENT
Promote sleep hygiene.
Non pharmacological:
Regular physical activity.
Optimal diet.
Psychotherapy: CBT, GET, family therapy.
Pharmacological:
To relieve the symptoms: antidepressant, NSAID, antimicrobial, Rituximab, acyclovir,
KEY POINTS
Fatigue occurs in up to 20% of patients seeking care.
Psychological causes should be at the top of the differential diagnosis for all patients presenting with fatigue, as the majority of cases have psychiatric causes.
The history can help in determining a psychiatric versus organic cause and thus aid in directing the evaluation of fatigue.
References
1- http://www.uptodate.com/contents/approach-to-the-adult-patient-with-fatigue#H10
2- http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-chronic-fatigue-syndrome?source=see_link#H15
3- http://www.uptodate.com/contents/treatment-of-chronic-fatigue-syndrome?source=see_link&anchor=H4#H6
4- http://www.cmaj.ca/content/174/6/765.full
5- http://bestpractice.bmj.com/best-practice/monograph/571/diagnosis.html

Thank you