Embed Size (px)
Citation preview

Approach to Anemias
Verdah SabihHouse OfficerMU-2 BBH

DEFINITION: The World Health Organization (WHO) defines
anemia as a hemoglobin level <130 g/L(13 g/dL) in men and <120 g/L (12 g/dL) in women.
The critical elements of erythropoesis are used for the initial classification of anemia. EPO production Iron availability Proliferative capacity of the bone marrow Effective maturation of red cell precursors

HOW DO THE PATIENT PRESENTS…. most often recognized by abnormal screening
laboratory tests. less commonly present with advanced anemia
and its attendant signs and symptoms. Acute Anemia blood loss or hemolysis –
Hb/HCT does not reflect the volume of blood loss
Mild – No symptoms. Enhanced oxygen delivery by changes in pH and increased CO2
10-15% - hypotension and decreased organ perfusion >30% - postural hypotension, tachycardia >40% - hypovolemic shock: confusion, dyspnoea,
diaphoresis hypotension &tachycardia

Acute hemolysis Intravascular hemolysis: acute back pain, free
hemoglobin in plasma and urine, renal failure Moderate anemia S/S
Fatigue Loss of stamina Breathlessness Tachycardia on physical exertion Symptoms may not appear in young, healthy
patients until hemoglobin is 7-8 g/dL Diseases in which patient presents with
anemia Infections Rheumatoid Arthritis Cancer Lymphoproliferative disorders (CLL, B cell
neoplasm)

EVALUATION OF PATIENT…… HISTORY:
Is the patient bleeding?Actively? In past?
Is there evidence of hemolysis? Is the patient nutritionally deficient? Pica? medication review, toxin exposure Symptoms of known diseases causing anemia:
Gastric ulceration Rheumatoid arthritis Renal failure
Duration of symptoms: Hemoglobinopathies in longer duration
Treatment history Medications for pain, hematinics
Nutritional history family history of anemia

PHYSICAL EXAMINATION…. Build, nourishment Signs of disease Vitals – fever, tachycardia, blood pressure Pallor Koilonychia,hair loss, glossitis,stomatitis Jaundice(hemolysis) Lymphadenopathy Bone tenderness Petechiae CVS: forceful heartbeat, strong peripheral pulses,
and a systolic “flow” murmurs RESP: Dyspnoea Abdomen: Splenomegaly


HOW TO INVESTIGATE….. I. Complete blood
count (CBC) A. Red blood cell count
1. Hemoglobin 2. Hematocrit 3. Reticulocyte count
B. Red blood cell indices 1. Mean cell volume (MCV) 2. Mean cell hemoglobin
(MCH) 3. Mean cell hemoglobin
concentration (MCHC) 4. Red cell distribution
width (RDW)
C. White blood cell count 1. Cell differential 2. Nuclear segmentation
of neutrophils D. Platelet count E. Cell morphology/
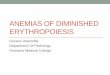
Peripheral smear 1. Cell size 2. Hemoglobin content 3. Anisocytosis 4. Poikilocytosis 5. Polychromasia

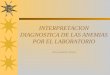
Normal smear
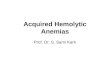
Severe Iron defeciency anemiaAnisocytosis (size), Poikilocytosis (shape
MacrocytosisMacrocytes, Ovalocytes
ThallassemiaTarget cells

II. Iron supply studies A. Serum iron 50–150
µg/dL B. Total iron-binding
capacity 300–360 μg/dL
C. Serum ferritin(also an acute phase reactant) 15-20 µg/dL – Lack of
Iron stores Women: ~30 µg/dL Men: ~ 100 µg/dL 200 µg/dL – adequate
iron stores Serum Transferrin
saturation: 25-50%
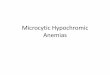
III. Marrow examination
A. Aspirate 1. M/E ratioa 2. Cell morphology 3. Iron stain
B. Biopsy 1. Cellularity 2. Morphology
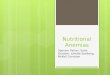
Normal iron stain

FURTHER INVESTIGATIONS……Microcytic anaemias
Haemoglobin electrophoresis Search for evidence of underlying infective, inflammatory or neoplastic disorder (blood cultures, ESR, C-reactive protein, ANA, CXR etc.)
Normocytic anaemias
Renal function, Haemolysis screen (if not already performed), Immunoglobulins and paraprotein screen, Search for evidence of underlying infective, inflammatory or neoplastic disorder
Macrocytic anaemias
Thyroid function tests, Liver function tests, Haemolysis screen (if not already performed)Serum Vit B12 & folic acid level

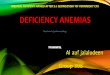
HOW TO CLASSIFY…..


YOU HAVE REACHED THE DIAGNOSIS NOW TREAT IT!.... Iron deficiency anemia: Transfusions: Only if there is hemodynamic
compromise or acute hemorrhage Oral:150-200 mg of iron daily 1 hour before meal
in divided doses (ferrous sulfate, ferrous gluconate) Continue for:
14 days + (Hb required level – Hb current level) x 4 half of the dose 6 – 9 months to restore iron
reserve Absorption
is enhanced: vit C(250 mg before taking iron), meat, orange juice, fish
is inhibited: cereals, tea, milk

Parentral iron subsitution:Bad oral iron tolerance (nausea, diarrhoea) &Necessity of quick management (CHD, CHF) 50 - 100 mg daily I.v only in hospital (risk of anaphylactic shock) I.m in outpatient department Total dose by iv infusion: iron to be injected (mg) = (15 - Hb g ) x body
weight (kg) x 3Iron dextran (IV or IM)Ferric gluconate (IV)iron sucrose (IV)Ferumoxytol(in adults with CKD)

ANEMIA OF CHRONIC DISEASE: Treat the underlying disorder (if possible) Transfusion rarely indicated Darbepoietin/EPO Goal is to not exceed hemoglobin values of 12
g/Dl THALASSEMIA: Thalassemia trait: None indicated β-Thalassemia intermedia, β-thalassemia major,
&Hgb H: Chronic transfusion Splenectomy Treatment for iron overload Management of complications, including leg
ulcers,pulmonary hypertension, gallstones, aplasia

SIDEROBLASTIC ANEMIAS: Hereditary:
fairly stable anemia. Iron overload develops in all patients because of inc. iron absorption.
Treat iron overload with phelebotomy or chelation. Acquired:
Iron overload does not respond to treatment with pyridoxine
Reversible: alcohol, isoniazid, and chloramphenicol removal of the drug
Lead poisoning: edetate disodium (EDTA) chelation

ANEMIA OF RENAL INSUFFICIENCY OR FAILURE: subcutaneous or IV ESA(erythropoietin or
darbepoietin) Goal is to maintain Hct between 33% and 36%
(Hgb between 11 and 12 g/dL) Iron therapy indicated for ferritin levels below 100
mg/L APLASTIC ANEMIA:
Withdraw the offending agent (if identified) Support with transfusions as needed; mild forms of
disease may not need definitive treatment Bone marrow transplantation (BMT) is the
treatment of choice in all patients under the age of 45 years with severe aplastic anemia when there is a human leukocyte antigen–matched donor
Immunosuppression with antithymocyte globulin plus cyclosporine plus corticosteroids is used when BMT not possible

PURE RED CELL APLASIA: Initial treatment is supportive with transfusions, if
needed Cases caused by parvovirus infection may respond to
IV immune globulin Cases caused by thymoma may respond to tumor
removal Immunosuppressive drugs are used in refractory
cases (e.g.corticosteroids, cyclosporine, cyclophosphamide)
MEGALOBLASTIC ANEMIA: Intramuscular vitamin B12 injections are usually the
initial treatment of choice for pernicious anemia Oral vitamin B12 can be equally effective in raising
serum levels. Must be given in very large doses (1–2 mg/day) in patients with pernicious anemia
Lower oral doses (250 μg/day) may be sufficient to treat food-cobalamin malabsorption

FOLATE DEFICIENCY: oral folic acid (1–2 mg/day is usually sufficient)
MYELODYSPLASTIC SYNDROMES: Supportive care Careful blood count monitoring with transfusion
support Iron overload can occur with repeated
transfusions---- Iron chelation Growth factor support with Erythropoietin
(EPO)& Granulocyte colony-stimulating factor Allogeneic stem cell transplantation Only
curative approach to treatment Hypomethylating agents (azacitidine or
decitabine) Lenalidomide Conventional chemotherapy (cytarabine based)

IMMUNE HEMOLYTIC ANEMIA Initial: Support with blood transfusions plus
prednisone 1 mg/kg/day with or without IV immune globulin (IgG)
Splenectomy: If refractory to prednisone Immunosuppressives and/or cytotoxic agents: If
refractory to splenectomy and prednisone G6PD deficiency
Supportive Sickle cell disorders (SS, Sβ-thal, SC)
Pain crises: Hydration and analgesics (avoid meperidine); transfusion usually not needed
Acute chest syndrome: Antibiotics, oxygen, exchange transfusion
Stroke: Exchange transfusion Hematopoietic cell transplantation may be
potentially curative,

REFRENCES…. Harrison's Principles of Internal Medicine, 19E The Johns Hopkins Internal Medicine Board
Review, 4th Edition