Embed Size (px)
Citation preview

Aortic Dissection Aortic Dissection
Zahir Rahman MDZahir Rahman MD
10/14/0210/14/02

ED History – 9:55 A.M.ED History – 9:55 A.M.
46 y.o AA male with with no pmhx cc: of 46 y.o AA male with with no pmhx cc: of weakness lower extremities and weakness lower extremities and inability to walk. Pt said 6 to 7 hours inability to walk. Pt said 6 to 7 hours prior to arrival, he had sudden onset prior to arrival, he had sudden onset interscapular and abdominal pain which interscapular and abdominal pain which progressed to weakness. progressed to weakness.
Neurosurgery called by ED staff for Neurosurgery called by ED staff for acute onset paraplegia.acute onset paraplegia.

Neurosurgery PE – 10:30 Neurosurgery PE – 10:30 AMAM
VS: 122/70 P: 72 RR: 14 VS: 122/70 P: 72 RR: 14 Muscle Strength: 2/5 L foot, all Muscle Strength: 2/5 L foot, all
other LE muscle strength 0/5other LE muscle strength 0/5 Sensory level below T5, diminished Sensory level below T5, diminished
but can feel light touchbut can feel light touch Rectal Sphincter Tone: Rectal Sphincter Tone:

Neurosurgery A/PNeurosurgery A/P
W/u for aortic aneurysm/ W/u for aortic aneurysm/ dissection dissection
R/o Spinal Cord compressionR/o Spinal Cord compression Continue Solumedrol, send for Continue Solumedrol, send for
MRA. MRA.

MRA MRA
Pt. had MRA done at 11:30 A.M. Pt. had MRA done at 11:30 A.M. CICU resident called with result at 12:30 CICU resident called with result at 12:30
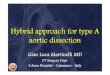
A.M. A.M. Patient was found to have a Type 1 Patient was found to have a Type 1
Aortic Dissection. No Pericardial Aortic Dissection. No Pericardial effusion. No Aortic Regurgitation effusion. No Aortic Regurgitation
Dissection from Proximal Aorta to below Dissection from Proximal Aorta to below the Renal arteries.the Renal arteries.
False Lumen was communicating with False Lumen was communicating with the Left Renal Artery.the Left Renal Artery.

RCA
RSC
LCA
INTIMA
TRUE LUMEN
FALSE LUMEN
PULMONARY TRUNK
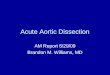
RSC

THROMBUS IN FALSE LUMEN
TRUE LUMEN

FALSE LUMEN
LRA
TRUE LUMEN


CV Fellow Called: 12:30 CV Fellow Called: 12:30 P.M.P.M.
46 y.o AA male from Liberia – No PMHx 46 y.o AA male from Liberia – No PMHx woke up at 3 AM with woke up at 3 AM with sudden onsetsudden onset 10/10 Anterior Chest Pain (Pressure like) 10/10 Anterior Chest Pain (Pressure like) and interscapular pain with radiation and interscapular pain with radiation down both arms. Over the course of the down both arms. Over the course of the next 6-7 hours, he developed diffuse next 6-7 hours, he developed diffuse abdominal pain, followed by numbness abdominal pain, followed by numbness from chest to feet which progressed to from chest to feet which progressed to bilateral weakness at which point he bilateral weakness at which point he called for an Ambulance. called for an Ambulance.

12:40 P.M. – pt complaining of CP 5/10 12:40 P.M. – pt complaining of CP 5/10 and abdominal pain, but no longer has and abdominal pain, but no longer has sensory or motor weakness of lower sensory or motor weakness of lower extremities.extremities.
PMHx: Pt says he has seen a doctor here PMHx: Pt says he has seen a doctor here and there and his bp was always fine. and there and his bp was always fine.
SHx: denies cocaine/drug useSHx: denies cocaine/drug use Exsmoker – quit 1 year ago. 10 pack Exsmoker – quit 1 year ago. 10 pack
year historyyear history FHx: No h/o sudden cardiac deaths. FHx: No h/o sudden cardiac deaths.
Mother and Father with HTN.Mother and Father with HTN.

PEPE
Vs: BP: R arm: 150/90 L arm: 154/90Vs: BP: R arm: 150/90 L arm: 154/90 Neck: No JVD, No BruitsNeck: No JVD, No Bruits Lungs: CTA b/lLungs: CTA b/l CV: RRR, S1,S2 nl, + S4, no murmursCV: RRR, S1,S2 nl, + S4, no murmurs ABD: Diffuse tenderness, no rebound, ABD: Diffuse tenderness, no rebound,
normal BS.normal BS. EXT: Pulses equal and symmetric B/LEXT: Pulses equal and symmetric B/L NEURO: No defecits, DTRs’ normal b/l NEURO: No defecits, DTRs’ normal b/l

Labs: 7/30/02 9:35 AM Labs: 7/30/02 9:35 AM
Bun/Cr: 29/2Bun/Cr: 29/2 AST: 41 AST: 41 ALT: 39 ALT: 39 AP: 70AP: 70 CK: 257 CK: 257 MB: 2.4 MB: 2.4 Trop: 0.3Trop: 0.3

EKGEKG

ManagementManagement
Pt was immediately bolused with Pt was immediately bolused with esmolol and titrated gradually to a esmolol and titrated gradually to a bp of approximately 122/70.bp of approximately 122/70.
Pt was transferred for surgery at Pt was transferred for surgery at 1:20 PM to SIUH1:20 PM to SIUH

Intraoperative TEE Ascend Intraoperative TEE Ascend AortaAorta

Intraoperative TEE – Aortic Intraoperative TEE – Aortic ArchArch

Descend Aorta – Descend Aorta – Communication back into Communication back into
true lumentrue lumen

Descend Aorta – Multiple Descend Aorta – Multiple Intimal FlapsIntimal Flaps

Intraoperative TEEIntraoperative TEE
NO AI, NO EffusionNO AI, NO Effusion Proximal Dissection – Not involving Proximal Dissection – Not involving
sinus of valsalvasinus of valsalva Concentric LVHConcentric LVH Multiple Dissection Flaps in Multiple Dissection Flaps in
Ascending and Descending AortaAscending and Descending Aorta

Surgery Surgery
Dissected Ascending Aorta was Dissected Ascending Aorta was dissected and replaced with a #22 dissected and replaced with a #22 mm Dacron interposition graft with mm Dacron interposition graft with a circumferential bypassa circumferential bypass
Pt. was hemodynamically stable Pt. was hemodynamically stable post surgery.post surgery.
Troponin at 21:51 - 1.28 (cutoff Troponin at 21:51 - 1.28 (cutoff 0.5 for AMI)0.5 for AMI)

Course: Course:
Labs: Labs: 7/31: CK: 666 / 35637/31: CK: 666 / 3563 7/31: Troponin: 4.5 7/31: Troponin: 4.5 7/31: MB: 25/ 27.97/31: MB: 25/ 27.9

Hospital CourseHospital Course Pt. was in ICU and became septic, ARF Pt. was in ICU and became septic, ARF
progressed to ESRD, Acute Liver Failure, progressed to ESRD, Acute Liver Failure, developed mesenteric ischemiadeveloped mesenteric ischemia
Pt. was managed with pressors (Levophed) Pt. was managed with pressors (Levophed) and was made DNR by family.and was made DNR by family.
On 8/10: CT scan showed large pericardial On 8/10: CT scan showed large pericardial effusion and dissecting aneurysm of the effusion and dissecting aneurysm of the thoracic aorta.thoracic aorta.
Bun/Cr: 155/12.1Bun/Cr: 155/12.1 AST/ALT: 2360/1500AST/ALT: 2360/1500 Patient coded, went into EMD and died. Patient coded, went into EMD and died.

Aortic Dissection Aortic Dissection
Zahir Rahman MDZahir Rahman MD
10/14/0210/14/02

ClassificationsClassifications
Acute: when diagnosis is made Acute: when diagnosis is made within 2 weeks of initial onset of within 2 weeks of initial onset of symptomssymptoms
Chronic: >2 weeks of symptomsChronic: >2 weeks of symptoms One third of patients fall into the One third of patients fall into the
chronic category.chronic category.

Common Classification SystemsCommon Classification Systems
Braunwald

Common Classifications of Aortic Common Classifications of Aortic
DissectionDissection

Variants of Aortic Variants of Aortic DissectionDissection

Predisposing FactorsPredisposing Factors Men/Female Ratio 2:1 to 5:1Men/Female Ratio 2:1 to 5:1 Chronic Systemic HTN (62-78%)Chronic Systemic HTN (62-78%) Proximal Dissection: Proximal Dissection:
– Peak age 50-55 yearsPeak age 50-55 years– MC on initial presentation to have HTN 70%MC on initial presentation to have HTN 70%
Distal Dissection: Distal Dissection: – Peak Age 60-70 yearsPeak Age 60-70 years
Direct Iatrogenic Trauma: 5% of casesDirect Iatrogenic Trauma: 5% of cases Indirect Trauma (eg sudden deceleration)Indirect Trauma (eg sudden deceleration)

Predisposing FactorsPredisposing Factors Hereditary Connective Tissue DiseasesHereditary Connective Tissue Diseases
– Marfan SyndromeMarfan Syndrome– Ehler Danlos SyndromeEhler Danlos Syndrome
Chromosomal AberrationsChromosomal Aberrations– Turners SyndromeTurners Syndrome– Noonans SyndromeNoonans Syndrome
Aortic DiseasesAortic Diseases– Aortic DilatationAortic Dilatation– Aortic AneurysmAortic Aneurysm– Anuloaortic ectasiaAnuloaortic ectasia– Aortic ArteritisAortic Arteritis– Bicuspid Aortic ValveBicuspid Aortic Valve

Predisposing FactorsPredisposing Factors
Females in 3Females in 3rdrd Trimester Pregnancy Trimester Pregnancy or 1or 1stst Stage of Labor Stage of Labor
Case Reports of:Case Reports of:– Cocaine Cocaine (Perron et al. Am J Emerg Med 1992)(Perron et al. Am J Emerg Med 1992)
– Abrupt Discontinuation of Beta Abrupt Discontinuation of Beta Blockers Blockers (Eber et al. Cardiology 1993; 83:128-131)(Eber et al. Cardiology 1993; 83:128-131)
– Probably Secondary to rapid rise in Probably Secondary to rapid rise in first derivative of pressure (dp/dt) on first derivative of pressure (dp/dt) on aortic wall.aortic wall.

Cystic Medial Cystic Medial DegenerationDegeneration
Medial Degeneration predisposes Medial Degeneration predisposes dissection by decreasing cohesiveness dissection by decreasing cohesiveness of layers of aortic wallof layers of aortic wall– More extensive in patients with:More extensive in patients with:
HTNHTN Marfan SyndromeMarfan Syndrome Bicuspid Aortic ValvesBicuspid Aortic Valves
– But, even in other causes of dissection, But, even in other causes of dissection, medial degeneration is much greater than medial degeneration is much greater than expected with normal aging.expected with normal aging.

PathogenesisPathogenesis
Intimal tears occur in regions of Intimal tears occur in regions of aorta subjected to greatest dp/dt aorta subjected to greatest dp/dt and pressure fluctuations.and pressure fluctuations.
MC sites for initiation of intimal MC sites for initiation of intimal tear: tear: – Ascending AortaAscending Aorta– 11stst Portion Descending Aorta Portion Descending Aorta

Proposed Mechanism of Initiation of Proposed Mechanism of Initiation of DissectionDissection

Natural HistoryNatural History Hydrodynamic forces propagate the dissection Hydrodynamic forces propagate the dissection
until rupture occurs either:until rupture occurs either:– Back into the lumen of the aortaBack into the lumen of the aorta– Through the adventitia (causing death)Through the adventitia (causing death)
Mortality Rates if untreated:Mortality Rates if untreated:– 1-3% per hour 1-3% per hour – 90% within 3 months90% within 3 months
Death usually caused by: Death usually caused by: – Acute aortic regurgitationAcute aortic regurgitation– Major branch vessel obstruction Major branch vessel obstruction – Aortic Rupture ( into pericardium, L pleural cavity, or Aortic Rupture ( into pericardium, L pleural cavity, or
mediastinum)mediastinum)

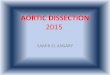
Symptoms of Aortic Dissection Symptoms of Aortic Dissection According to a report on 464 patients from the International According to a report on 464 patients from the International
Registry of Acute Aortic Dissection.Registry of Acute Aortic Dissection.(Hagan et al. Jama 2000; 283:897-903)(Hagan et al. Jama 2000; 283:897-903)
0
20
40
60
80
100AbdominalPain
Back Pain
Ant. ChestPain
ClassicTearing
Sharp Pain
Abrupt Onset
Column 1

Clues to Proximal Clues to Proximal DissectionDissection
Substernal chest painSubsternal chest pain Neck, jaw, throat or face painNeck, jaw, throat or face pain Aortic InsufficiencyAortic Insufficiency Decreased pulse or blood pressure in R armDecreased pulse or blood pressure in R arm Decreased R carotid pulse Decreased R carotid pulse Pulse abnormalities are seen in 50% of Pulse abnormalities are seen in 50% of
proximal dissectionsproximal dissections Ischemic EKG changesIschemic EKG changes AMI – Inferior (5%)AMI – Inferior (5%) Marfans SyndromeMarfans Syndrome Hypotension Hypotension Syncope – 12% Syncope – 12% CVA – 5-10% CVA – 5-10%

Aortic RegurgitationAortic Regurgitation
AR in 18-50% casesAR in 18-50% cases Diastolic murmur reported in 25% Diastolic murmur reported in 25%
pts.pts. Acute Severe AR – 2Acute Severe AR – 2ndnd MC cause of death MC cause of death
AD.AD. Murmur can wax and wane and intensity Murmur can wax and wane and intensity
will vary with BPwill vary with BP 3 possible mechanisms for acute AR in 3 possible mechanisms for acute AR in
dissectiondissectionHagan et al. IRAD. JAMA 2000;283:897-903.

Mechanisms of Aortic Mechanisms of Aortic Regurgitation in Proximal ADRegurgitation in Proximal AD

Hypotension with Proximal Hypotension with Proximal DissectionDissection
Cardiac tamponadeCardiac tamponade Severe acute Aortic regurgitation Severe acute Aortic regurgitation
with cardiogenic shockwith cardiogenic shock Myocardial Infarction with resultant Myocardial Infarction with resultant
LV systolic dysfunction – usually LV systolic dysfunction – usually RCA.RCA.
Acute Aortic Rupture.Acute Aortic Rupture. Pseudohypotension by involving Pseudohypotension by involving
brachiocephalic artery brachiocephalic artery

Predicting Death in Type A Predicting Death in Type A Aortic Dissection Aortic Dissection (Mehta et al. Circulation. (Mehta et al. Circulation.
2002;105:200-206)2002;105:200-206)
Evaluated 547 patients enrolled in IRAD Evaluated 547 patients enrolled in IRAD from Jan 1996 to Dec 1999.from Jan 1996 to Dec 1999.
In hospital mortality was 32.5%, 26.9% In hospital mortality was 32.5%, 26.9% in surgically treated patients vs. 56.2% in surgically treated patients vs. 56.2% in medically treated patientsin medically treated patients
Rupture accounted for 33.3% of deathsRupture accounted for 33.3% of deaths Neurological defecit - 13.9 % of deathsNeurological defecit - 13.9 % of deaths Visceral ischemia/kidney failure (11.5%)Visceral ischemia/kidney failure (11.5%) Cardiac Tamponade (7.9%)Cardiac Tamponade (7.9%)

Clinical Variables Associated with Clinical Variables Associated with High In-Hospital Mortality Rates.High In-Hospital Mortality Rates.
(Mehta et al. Circulation. (Mehta et al. Circulation. 2002;105:200-206)2002;105:200-206)

Interscapular painInterscapular pain HTN less commonly associated about 35%HTN less commonly associated about 35% Left Pleural effusionLeft Pleural effusion Pulse defecits are less frequent about Pulse defecits are less frequent about
15%15% Usually involve femoral or left subclavianUsually involve femoral or left subclavian Spinal Cord Ischemia (10%) Spinal Cord Ischemia (10%)
– Transverse MyelitisTransverse Myelitis– ParaplegiaParaplegia– QuadriplegiaQuadriplegia
Clues to Distal DissectionClues to Distal Dissection

Clinical Prediction of Acute Clinical Prediction of Acute Aortic DissectionAortic Dissection (von Kodolitsch et al, Arch Intern (von Kodolitsch et al, Arch Intern
Med 2000;160:2977-2982)Med 2000;160:2977-2982)
Jan 1 1988 to Dec 31, 1996 41,495 Jan 1 1988 to Dec 31, 1996 41,495 presented to ED at Univ Hosp Eppendorf, presented to ED at Univ Hosp Eppendorf, Hamburg, Germany.Hamburg, Germany.
250 constituted study group250 constituted study group– CP, back pain or both within last 2 weeksCP, back pain or both within last 2 weeks– ACS or another diagnosis excludedACS or another diagnosis excluded– Of remaining patients, considered if suspicious Of remaining patients, considered if suspicious
for AD by 2 ED physicians.for AD by 2 ED physicians. 26 Clinical Variables to find any 26 Clinical Variables to find any
independent clinical predictors of independent clinical predictors of dissection.dissection.

(von Kodolitsch et al, Arch Intern Med 2000;160:2977-2982)(von Kodolitsch et al, Arch Intern Med 2000;160:2977-2982)

(von Kodolitsch et al, Arch Intern Med 2000;160:2977-2982)(von Kodolitsch et al, Arch Intern Med 2000;160:2977-2982)

Aortic Pain: Aortic Pain: immediate onset, immediate onset, tearing or ripping tearing or ripping character or both.character or both.
Mediastinal Mediastinal WideningWidening
Pulse DifferentialsPulse Differentials
(von Kodolitsch et al, Arch Intern Med (von Kodolitsch et al, Arch Intern Med 2000;160:2977-2982)2000;160:2977-2982)

EKGEKG
EKG: 1/3 exhibit LVHEKG: 1/3 exhibit LVH EKG is important to rule out any EKG is important to rule out any
ischemic changes or MI which ischemic changes or MI which would lead to an alternate would lead to an alternate diagnosisdiagnosis
EKG may display infarction EKG may display infarction EKG – usually shows nonspecific EKG – usually shows nonspecific
ST-T wave changes.ST-T wave changes.

CXR CXR
Widened Mediastinum suggestive Widened Mediastinum suggestive but not diagnostic.but not diagnostic.
Seen Anywhere from 50% in most Seen Anywhere from 50% in most reports.reports.
And in one report of 236 cases as And in one report of 236 cases as high as: 90% high as: 90% (Spittell,(Spittell, Mayo Clinic Proc 68:642,1993.)Mayo Clinic Proc 68:642,1993.)

Normal Aorta in CXR 3 years Normal Aorta in CXR 3 years PriorPrior

Enlargement of the Aortic Enlargement of the Aortic KnobKnob
A Case of Proximal Aortic Dissection A Case of Proximal Aortic Dissection

Comparison of Imaging Comparison of Imaging ModalitiesModalities
(Braunwald)

AortographyAortography
Sensitivity: 86-88%Sensitivity: 86-88% Specificity: 75-94%Specificity: 75-94% False negatives if intramural False negatives if intramural
hematoma or thrombosis of false hematoma or thrombosis of false lumenlumen
Good at detecting branch vessel Good at detecting branch vessel involvement and Coronary Artery involvement and Coronary Artery invovlvement.invovlvement.

Thoracic Aortagram in AP Thoracic Aortagram in AP viewview

CTCT Sensitivity 83-94% Sensitivity 83-94% Specificity of 100%Specificity of 100% Spiral CT increased sensitivity to 96%Spiral CT increased sensitivity to 96% Non-invasive with rapid availability Non-invasive with rapid availability (MC (MC
initial imaging modality in IRAD pts)initial imaging modality in IRAD pts)
Needs contrast to be effectiveNeeds contrast to be effective Disadvantages:Disadvantages:
– Cannot Detect ARCannot Detect AR– Does not detect Site of Intimal Tear wellDoes not detect Site of Intimal Tear well– Cannot detect Coronary Artery InvolvementCannot detect Coronary Artery Involvement

Contrast-Enhanced CT at Contrast-Enhanced CT at level of Ventriclelevel of Ventricle

Left Anterior Oblique View Contrast Enhanced CTLeft Anterior Oblique View Contrast Enhanced CTIntimal Flap originates beyond Left SC ArteryIntimal Flap originates beyond Left SC Artery

TEETEE Non-Invasive, Performed Quickly at Non-Invasive, Performed Quickly at
BedsideBedside Sensitivity 98 – 99%Sensitivity 98 – 99% Specificity: 94 – 95% Specificity: 94 – 95% (biplane or multiplane TEE)(biplane or multiplane TEE)
Good at detecting Coronary Artery Good at detecting Coronary Artery InvolvementInvolvement
Disadvantage: does not evaluate Disadvantage: does not evaluate distal ascending aorta and proximal distal ascending aorta and proximal arch arch (because of the interposition of air filled trachea and (because of the interposition of air filled trachea and main stem bronchus)main stem bronchus)

Descend Aorta – Descend Aorta – Communication back into Communication back into
true lumentrue lumen

MRIMRI Gold Standard for DiagnosisGold Standard for Diagnosis Sensitivity and Specificity of 98-100% Sensitivity and Specificity of 98-100% Disadvantages: Disadvantages:
– Limited AvailabilityLimited Availability– Limit the presences of monitoring and Limit the presences of monitoring and
support devicessupport devices– Relatively CI in unstable patients. Relatively CI in unstable patients. – CI:CI:
PacemakersPacemakers Certain types of vascular clipsCertain types of vascular clips Older metallic heart valvesOlder metallic heart valves

RCA
RSC
LCA
INTIMA
TRUE LUMEN
FALSE LUMEN
PULMONARY TRUNK
RSC

Practical Assessment of Practical Assessment of Imaging ModalitiesImaging Modalities

Smooth Muscle Myosin Heavy Smooth Muscle Myosin Heavy ChainChain
AD causes extensive damage to the AD causes extensive damage to the smooth muscle cells of the media smooth muscle cells of the media releasing smooth muscle heavy chain into releasing smooth muscle heavy chain into the circulation. the circulation.
Serum Values: Serum Values: – 95 AD pts: 22.4 +/- 40.4 ug/L95 AD pts: 22.4 +/- 40.4 ug/L– 131 Volunteers: 0.9 +/- 0.4 ug/L131 Volunteers: 0.9 +/- 0.4 ug/L– 48 AMI pts: 2.1 +/- 1.6 ug/L48 AMI pts: 2.1 +/- 1.6 ug/L– 33 pts presented within 3 hrs of onset of AD: 33 pts presented within 3 hrs of onset of AD:
51+/-52.3 ug/L 51+/-52.3 ug/L Serum Levels > 10 ug/L showed 100% Serum Levels > 10 ug/L showed 100%
specificity for Aortic Dissection. specificity for Aortic Dissection. (Suzuki et al. Circulation 1996;93:1244-1249)(Suzuki et al. Circulation 1996;93:1244-1249)

MANAGEMENTMANAGEMENT Therapy is targeted at halting the Therapy is targeted at halting the
progression of the dissectionprogression of the dissection It is the course of the tear not the It is the course of the tear not the
tear itself that leads to compromise of tear itself that leads to compromise of vasculature or rupturevasculature or rupture
Goal:Goal:– Reduction of SBP (100-120) Reduction of SBP (100-120) – Dimunition of dp/dt (reflects force of LV Dimunition of dp/dt (reflects force of LV
ejection) through use of a beta blocker.ejection) through use of a beta blocker.

Sodium NitroprussideSodium Nitroprusside
Sodium Nitroprusside for acute Sodium Nitroprusside for acute reduction starting 10 – 20 mcg/min reduction starting 10 – 20 mcg/min and titrated upwardand titrated upward
Must initiate BB prior to instituion of Must initiate BB prior to instituion of Nipride due to its effect on raising Nipride due to its effect on raising dP/dT when used alonedP/dT when used alone
Adding IV BB prior until desired effect Adding IV BB prior until desired effect such as HR 60 – 80s (propranolol 1 such as HR 60 – 80s (propranolol 1 mg Q 3-5 minutes max 10 mg) mg Q 3-5 minutes max 10 mg)
Then Q 4-6 hrs at a dose of 2 – 6 mgThen Q 4-6 hrs at a dose of 2 – 6 mg

LabetololLabetolol
Effectively lowers dP/dT as well as Effectively lowers dP/dT as well as reducing arterial pressurereducing arterial pressure
Initial dose is 20mg followed by 40 to 80 Initial dose is 20mg followed by 40 to 80 mg Q 10 – 15 minutes (max 300mg IV)mg Q 10 – 15 minutes (max 300mg IV)
Once BP controlled maintenance by Once BP controlled maintenance by continuous infusion continuous infusion
Infusion at 2mg/min titrating up to 5 –10 Infusion at 2mg/min titrating up to 5 –10 mg/min mg/min

EsmololEsmolol Ultra short acting BB for those with Ultra short acting BB for those with
labile blood pressure or those that are labile blood pressure or those that are surgical candidates. surgical candidates. (Long acting medications (Long acting medications may affect intraoperative bp management)may affect intraoperative bp management)
Load with 500 mcg/kg bolusLoad with 500 mcg/kg bolus Infusion starts @ 50mcg/kg/min titrate Infusion starts @ 50mcg/kg/min titrate
to 200 mcg/kg/min for controlto 200 mcg/kg/min for control Controls dP/dT as well as blood pressureControls dP/dT as well as blood pressure Can be used in patients with uncertain Can be used in patients with uncertain
risk for bronchospasmrisk for bronchospasm

Contraindications to BBContraindications to BB Patients with severe Brady or AV block or Patients with severe Brady or AV block or
bronchospasm BB may be CIbronchospasm BB may be CI Calcium channel blockers specifically Calcium channel blockers specifically
Cardizem and Diltiazem can be used if Cardizem and Diltiazem can be used if bronchospasmbronchospasm
Provide negative Inotrope and Provide negative Inotrope and Chronotropic effects Chronotropic effects
If Dissection involves the renal arteries If Dissection involves the renal arteries patients may develop high renin HTNpatients may develop high renin HTN
Treat with IV enalaprilTreat with IV enalapril

Other ConsiderationsOther Considerations Hypotension must ensure if its true or Hypotension must ensure if its true or
falsefalse May be secondary to compromise of May be secondary to compromise of
artery by dissection artery by dissection (pseudohypotension) so check both arms(pseudohypotension) so check both arms
If true hypotension may indicate rupture If true hypotension may indicate rupture or tamponadeor tamponade
Fluids first then use levophed Fluids first then use levophed (norepinephrine)(norepinephrine) or phenylephrine or phenylephrine (neosynephrine)(neosynephrine)
Dopamine should be avoided since it can Dopamine should be avoided since it can raise dP/dT unless used at low doses for raise dP/dT unless used at low doses for renal perfusionrenal perfusion

Cardiac TamponadeCardiac Tamponade
Pericardiocentesis may be harmfulPericardiocentesis may be harmful Retrospective study of 7 patients (6 Retrospective study of 7 patients (6
hypotensive, 1 normotensive)hypotensive, 1 normotensive)– 3 of 4 with successful 3 of 4 with successful
Pericardiocentesis died w/in 5-40 Pericardiocentesis died w/in 5-40 minutes of the procedure due to acute minutes of the procedure due to acute EMDEMD
– 0 of 3 w/o pericardiocentesis died prior 0 of 3 w/o pericardiocentesis died prior to surgeryto surgery
Isselbacher et al, Circulation 1994: 90;2375-2378.

Cardiac TamponadeCardiac Tamponade
Increase in Intraaortic pressure after Increase in Intraaortic pressure after pericardiocentesis causing a reopening pericardiocentesis causing a reopening of the closed communication between of the closed communication between the false lumen and pericardial space, the false lumen and pericardial space, leading to lethal cardiac tamponade.leading to lethal cardiac tamponade.
Prudent to do Pericardiocentesis in AD Prudent to do Pericardiocentesis in AD only if in EMD or marked hypotension, only if in EMD or marked hypotension, and aspirate only enough pericardial and aspirate only enough pericardial fluid to raise bp. fluid to raise bp.

Indications for Definitive Indications for Definitive Surgical and Medical Therapy Surgical and Medical Therapy
in ADin AD

Surgical Repair of Proximal Surgical Repair of Proximal DissectionsDissections

SurgerySurgery Preop mortality 3% if expedited and Preop mortality 3% if expedited and
increases to 20% if prolongedincreases to 20% if prolonged Objectives of surgery are to remove Objectives of surgery are to remove
the most severely damaged the most severely damaged segments of the aorta and to segments of the aorta and to obliterate the false lumen by obliterate the false lumen by suturing the most proximal segmentsuturing the most proximal segment
Long term survival is not effected Long term survival is not effected by failure to resect intimal tear by failure to resect intimal tear (Miller et (Miller et
al. Journal Thoracic CV Surg 78:365;1979.al. Journal Thoracic CV Surg 78:365;1979.

Surgery with ARSurgery with AR In certain cases valve can be In certain cases valve can be
preserved by removing tear and preserved by removing tear and resuspending leafletsresuspending leaflets
It avoids long term anticogulationIt avoids long term anticogulation However if repair is unsuccessful However if repair is unsuccessful
or if patient had pre-existing or if patient had pre-existing valvular disease need AVRvalvular disease need AVR
In patients with Marfans need AVRIn patients with Marfans need AVR

Endovascular techniquesEndovascular techniques For treating high risk patients ( i.e. renal or For treating high risk patients ( i.e. renal or
visceral involvement) which carry a high visceral involvement) which carry a high operative mortality (>50%)operative mortality (>50%)
Balloon fenestration flow back to true lumen Balloon fenestration flow back to true lumen decompressing false lumendecompressing false lumen
Stenting of branch vessels compromised by Stenting of branch vessels compromised by dissection.dissection.
Intraluminal stent – grafts to close off the site Intraluminal stent – grafts to close off the site of entry into false lumen and promote of entry into false lumen and promote thrombosis. thrombosis.
30 Day mortality for Proximal Dissections of 30 Day mortality for Proximal Dissections of intraluminal stents reported around 25%.intraluminal stents reported around 25%.
At present, about 13% of patients with AD get At present, about 13% of patients with AD get endovascular stenting. endovascular stenting.

Long Term Long Term Survival in PAD s/p repair who survive their Survival in PAD s/p repair who survive their
hospital stay is:hospital stay is:– 65-80% at 5 years65-80% at 5 years– 50% at 10 years50% at 10 years
MC cause of death in long-term survivors:MC cause of death in long-term survivors:– Rupture of the Aorta due to subsequent Rupture of the Aorta due to subsequent
dissection or aneurysm formation. dissection or aneurysm formation. Long Term Management: Long Term Management:
– Optimal BP control with Beta blockersOptimal BP control with Beta blockers– Periodic clinical and imaging assessments of Periodic clinical and imaging assessments of
AortaAorta

Intramural Hematoma (H)Intramural Hematoma (H)

Crescenteric Hematoma that does not Enhance Crescenteric Hematoma that does not Enhance confirming a intramural Hematoma that does not confirming a intramural Hematoma that does not
communicate with the Aortic Lumen.communicate with the Aortic Lumen.

Evolution of a Penetrating Evolution of a Penetrating atherosclerotic Ulcer of Aortaatherosclerotic Ulcer of Aorta