Embed Size (px)
DESCRIPTION
Citation preview

National HIV Prevention ConferenceAugust 16, 2011
Antiretroviral Medication Adherence
Division of HIV/AIDS PreventionNational Center for HIV/AIDS, Viral Hepatitis, STD , and TB Prevention
Cindy Lyles, PhDPrevention Research Branch,
Division of HIV/AIDS Prevention, CDC

Thanks toAdherence Writing Group
CDC: Linda Beer, Nicole Crepaz, Linda Koenig,
Cindy Lyles, Khiya Marshall, Rebecca Morgan,
David Purcell, Paul Weidle
HRSA: Brian Feit, Anna Huang

Outline
RationaleMethods Evidence Recommendations

Rationale for ART Adherence ART reduces viral burden, prolongs survival
and quality of life ART is now key for treatment & prevention health benefits for the PLWH Preventing sexual transmission of HIV
Adherence is critical for treatment success Positively associated with longer survival, lower
HIV viral load, greater viral suppression Declines/slips associated with treatment failure Suboptimal adherence can lead to viral resistance
& limited future trt options

Rationale for ART Adherence Success of HPTN 052 trial RCT: efficacy of early treatment (vs trt as usual) Both arms received couples risk reduction
counseling Early initiation of ART led to a 96% reduction in
risk of transmitting HIV to uninfected sexual partners
In combination w/ ART, regular, intense adherence counseling & support was provided
• Regular monthly visits
• Provided to both the index patient and the partner
• Provided by both the physician and an adherence counselor

Context for Promoting ART Adherence
Critical to help achieve NHAS goals Key activity in DHAPs strategic plan & in the
new Enhanced Comprehensive HIV Prevention Plan (ECHPP) Project
Expanded testing & early treatment more critical to focus on adherence

Methods (page 1)
Recommendations based on: Reviewed existing published recommendations Review of Reviews – Previously published
literature reviews, systematic reviews, and meta-analyses
Two types of reviews:
• Efficacy of HIV medication adherence interventions
• Correlates of HIV medication adherence
Published cost-effectiveness literature

Methods (page 2)
Recommendations based on: Results of CDC’s Prevention Research Synthesis
(PRS) Efficacy Review• Systematic review of all U.S.-based intervention evaluation
studies
• Identify specific interventions shown to be efficacious in improving adherence or reducing viral load
• Compendium of Evidence-based HIV Prevention Interventions (http://www.cdc.gov/hiv/topics/research/prs/)

Methods (page 3)
Recommendations based on: Other published literature, with emphasis on
specific topics:• Measurement & monitoring
• Current adherence levels & status of adherence interventions
• Barriers to implementation
• Special considerations & special populations

Evidence – What are Current Adherence Levels?
Adherence levels tend to be sub-optimal; tend to decrease over time
Estimates vary; 20% - 80% Data sources/methods vary greatly Study design (e.g. drug trials, cohort studies, surveys)
Study sample (e.g. target, eligibility)
How to measure/calculate adherence• Method of measurement (e.g. EDM, S-R, pharmacy)• Recall or time periods• Calculation (mean #; mean %; cutoff >90%)

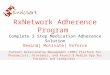
Evidence – What are Current Adherence Levels?
Percent of individuals w/ >90% adherence to ART (n=84 studies)
50 55 60 65 70 75 80
Worldwide
North America
Meta-analysis (Ortego, 2011)
62%
59%

Evidence – Correlates of Adherence
Treatment regimen factors
Individual-level factors Patient-Provider factors

Evidence – Correlates of Adherence
Treatment regimen factors: Complexity of regimen – Pill burden, dosing frequency,
dietary restrictions
Frequency and severity of side effects

Evidence – Correlates of Adherence
Individual-level factors: Co-morbidity factors –substance abuse, alcohol abuse;
mental health issues, including depression, anxiety, other psychological symptoms
Psycho-social factors – Attitudes, beliefs, fear, stigma, & denial related to HIV disease; quality of life/life satisfaction; social support

Evidence – Correlates of Adherence
Individual-level factors: Adherence cognitions/competencies – Understanding
of ART regimen, ART benefits; Attitudes & beliefs about ART efficacy; Self-efficacy of adherence; poor self-management/adherence skills
Other – daily schedule issues; homelessness; income/financial issues

Evidence – Correlates of Adherence
Patient-Provider factors: Quality of relationship; provider support; shared
decision-making

Evidence – Adherence Interventions
Interventions are efficacious in improving adherence Several rigorous meta-analyses
Moderate magnitude of effects
Slightly weaker findings, in general, for clinical outcomes (viral suppression; CD4 cell count)
Stronger effects during the intervention or short follow-up; weaker effects over time

Evidence – Adherence Interventions
Interventions are cost-effective & beneficial to long-term survival of the individual No systematic reviews; handful of studies
Varied by study design, type of intervention, etc.

Evidence – Adherence Interventions
Key Intervention Elements Improving knowledge about treatment
Discussing/addressing cognitive barriers
Providing patient-centered or individual-level approach
Targeting medication management skills
Providing support (provider, group, peer, family)
Longer intervention duration
Robust findings with regards to: Deliverer; Setting; Delivery unit; Risk group; ART
naïve/exp

Adherence Recommendations –Patient Issues
Assess patient’s readinessEducate on importance of adherence to ARTAddress misconceptions or other concernsAddress barriers by linking patients to appropriate services Structural: homelessness, transportation, insurance Co-morbidities: depression, mental health,
drug/alcohol abuse

Adherence Recommendations –Regimen Issues
Simplify treatment regimen: reduce pill burden, dosing frequency, and dietary restrictions Involve the patient in decision makingTailoring schedule to the patient’s lifestyle, linking activities to “cues” as reminders, clarify instructions using a personal treatment plan Encouraging pill sorting and storage devices to fit with daily routinePrepare for, assess, and manage side effects at each visit

Recommendations – Maintaining Adherence
Provide adherence reminder devices or memory aides –alarms, diaries, pill boxes, beepersEmploy an adherence team to provide ongoing support -nurse practitioner, case manager, social worker, pharmacist, counselor, peer support person, family memberAssess adherence at each visit, in a non-judgmental way with open-ended questions to allow patient to disclose problems or barriersInvolve patient in problem-solving activities

Summary
We need to focus on every element in the care continuum, including adherence, in order to maximize TRT benefits
Expanding testing
Initiating ART
Linking to care
Adherence to ART

The findings & conclusions in this report are those of the authors & do not necessarily represent the official position of the Centers for Disease Control and Prevention
Thank You!
Cindy [email protected]