Embed Size (px)
Citation preview

ANTIRETROVIRALDRUGS
Dr.Vijay bhushanam

Virus
• Ultra microscopic infectious particle• Does not have components of a cell• Unable to replicate outside of a living host cell• Parts of a virus particle (Virion) ….
Genome
(Nucleic acid consisting of either DNA or RNA, not both)
+
Capsid
(Protein shell that surrounds and protects the nucleic acid)
+
Envelope
(Lipoprotein membrane)

Virus
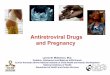
A virus infecting a bacterium.

Classification of Viruses
• DNA viruses • E.g: Papillomavirus (warts), Parvovirus (erythema
infectiosum, aplastic anemia), Poxvirus (smallpox), Herpesvirus (Herpes), Hepadenovirus (serum hepatitis), Adenovirus (sore throat, conjunctivitis) etc
• RNA viruses• E.g: Arbovirus (Yellow fever), Arenavirus (Meningitis),
Bunyavirus (encephalitis), Coronavirus (URTI), Orthomyxovirus (Influenza), Paramyxovirus (Measles, Mumps), Picornavirus (Polio, Meningitis, URTI), Rhabdovirus (Rabies), Retrovirus (AIDS, Leukemia) etc

Retroviridae
• Genome: Plus-sense RNA• Capsid: Protein• Envelop: Lipid, Glycoproteins• Enzymes:
• Reverse transcriptase
• Integrase enzyme• Protease enzyme
• E.g: HTLV-I (Human T-cell lymphotropic virus I). and………

Human Immunodeficiency Virus (HIV)
• Human immunodeficiency virus (HIV) is a single stranded RNA retrovirus that causes Acquired immunodeficiency syndrome (AIDS), a condition in which individuals are at increased risk for developing certain infections and malignancies.
• The virus is found in two major forms: • HIV-1, the most prevalent worldwide, and • HIV-2, the most common in western Africa
• HIV is a typical retrovirus.• The nucleocapsid contains 2 copies of RNA genome
(capped & polyadenlyated)

Human Immunodeficiency Virus (HIV)

Human Immunodeficiency Virus (HIV)
• AIDS remains a serious threat because of the expense and inaccessibility of antiretroviral agents in the developing countries in which the disease is most prevalent.
• In addition, the effectiveness of antiretroviral drugs has been diminished by the emergence of multidrug- resistant virus

Classification of Anti-Retroviral drugs (Anti-HIV drugs):
• The Anti-HIV drugs can be classified into
1. Nucleoside reverse transcriptase inhibitors (NRTIs): Zidovudine, Stavudine, Lamivudine, Abacavir, Zalcitabine, Emtricitabine, Didanosine.
2. Non nucleoside reverse transcriptase inhibitors (NNRTIs): Efavirenz, Nevirapine, Delaviridine.
3. Nucleotide reverse transcriptase inhibitors (NTRTIs): Tenofovir
4. Protease inhibitors (PIs): Saquinavir, Indinavir, Nelfinavir, Amprenavir, Fosamprenavir, Ritonavir, Lopinavir, Atazanavir.
5. Entry/Fusion inhibitors: Enfuvirtide

Nucleoside reverse transcriptase inhibitors (NRTIs)
• E.g: Zidovudine, Stavudine, Lamivudine, Abacavir, Zalcitabine, Emtricitabine, Didanosine.
• Mechanism of action: • They act by incorporating themselves into the DNA of the
virus (competing with natural nucleotides), thereby stopping the building process of transcription from RNA to DNA. The resulting DNA is incomplete and cannot create a new virus.
• Block the HIV replication, block the infection of new cells• No effect on already infected cells.

Nucleoside reverse transcriptase inhibitors (NRTIs)
• Pharmacokinetics:Drug Oral
bioavailability
Distribution metabolism Renal Excretion
T1/2
Zidovudine 60-65 All tissues, CSF, PB 35%
Hepatic 15, FD 1-3
Stavudine 85-90 Good, CSF, Negligible PB
Minor 40, FD 1.2
Lamivudine 85-90 CSF 20%, PB 35% Minor 72, FD 5-7
Abacavir 83 CSF 33%, PB 50% Liver, AD Metabolites, 1 FD
1.5
Zalcitabine >80 CSF 20%, PB <4% Minor 60 FD 2
Emtricitabine 93 <4% PB Liver 13% 86 FD 10
Didanosine 42 CSF 20%, <5% PB Purine metabolic pathway
18 FD 1.5

Nucleoside reverse transcriptase inhibitors (NRTIs)
• Therapeutic uses: • Generally used in combination with other drugs to
avoid development of resistance for HIV.• HAART(Highly active antiretroviral therapy):
Synergistic combinations of NRTIs and Protease inhibitors
• Popular HAART combinations • NRTIs(2)+PI(1)• NRTIs(2)+NNRTI(1)• NRTIs(2)+Abacavir• NRTIs(2)+PI(1)+Ritonavir• NRTI(1)+NNRTI(1)+PI(1)• NRTI(1)+NNRTI(1)+PI(2)

Nucleoside reverse transcriptase inhibitors (NRTIs)
• Adverse effects:• Lactic acidosis, severe hepatomegaly, hepatic
steatosis.

Zidouvidine (AZT, ZDV)
• First antiviral drug used against HIV. • It is a thymidine analogue that is effective against HIV-1,
HIV-2, and HTLV I and II.• Zidovudine, in combination with one or more other
antiretroviral agents, is approved for the treatment of HIV infection in adults and children and for post-exposure prophylaxis. It is used alone or in combination for the prevention of prenatal and perinatal transmission to the baby by HIV-infected pregnant women.
• Adverse effects: Headache, nausea, vomiting, anorexia, fatigue, confusion, insomnia, malaise, hepatitis, myopathy, myositis, bone marrow toxicity, anaemia, neutropenia, and other haematological abnormalities.

Stavudine (D4T)
• It is a thymidine nucleoside analogue• Active against HIV-1 and HIV-2.• It is approved for the therapy of HIV infection as part
of a multidrug regimen and is also used for Postexposure prophylaxis.
• Adverse effects: Headache, diarrhoea, skin rash, nausea, vomiting, insomnia, anorexia, myalgia, peripheral neuropathy. Lactic acidosis occurs more frequently with Stavudine than with other NRTIs.

Lamivudine (3TC)
• It is a cytosine nucleoside analogue • Activite against HIV-1, HIV-2, and hepatitis B virus.• It is approved as part of a multidrug regimen for the
therapy of HIV infection in adults and children and has been used for HIV postexposure prophylaxis.
• Lamivudine is the best-tolerated NRTI.
• Adverse effects: Headache, malaise, fatigue, insomnia.

Abacavir (ABC)
• It is a guanosine nucleoside analogue• Indicated for the therapy of HIV-1 infection in adults
and children. It is used as part of a multidrug regimen . It is also used for Postexposure HIV infection prophylaxis.
• Adverse effects: Anorexia, nausea, vomiting, malaise, headache, and insomnia. A potentially fatal hypersensitivity reaction develops in approximately 5% of patients. Fever and rash are the most common symptoms of this reaction; malaise, respiratory symptoms, and gastrointestinal complaints may also occur.

Didanosine (DDI)
• It is an adenosine analogue • Active against HIV-1, HIV-2, and HTLV-I.• It is approved as part of a multidrug regimen for the
therapy of HIV infection and is also used as Postexposure HIV prophylaxis.
• Adverse effects: Diarrhea, abdominal pain, nausea, vomiting, anorexia and dose-related peripheral neuropathy, pancreatitis, hyperuricemia, bone marrow suppression, retinal depigmentation, and optical neuritis.

Non nucleoside reverse transcriptase inhibitors (NNRTIs):
• E.g: Efavirenz, Nevirapine, Delaviridine.
• Mechanism of action: • They act by stopping HIV production by binding directly
onto reverse transcriptase (non-competitively) and preventing the conversion of RNA to DNA.
• Do not require activation through phosphorylation.

Non nucleoside reverse transcriptase inhibitors (NNRTIs):
Drug Oral bioavailability
Distribution, Protein binding
Metabolism
Excretion T1/2
Nevirapine 90-95 Wide, CSF 45%,PB 60%
Hepatic CYP3A4
Renal 90% metabolites, FD 3%
25-30 Hrs
Efavirenz 50 CSF 1%, PB 99%
Hepatic CYP3A4, CYP2B6
Feces 30% FD Urine 25% metabolites, FD 5%
40-55 Hrs
Delaviridine 85 CSF 0.4%, PB 98%
Hepatic CYP3A4, CYP2D6
Feces 44% FD, Urine 5% FD, metabolites 51%
6Hrs

Non nucleoside reverse transcriptase inhibitors (NNRTIs):
• Therapeutic uses:• All NNRTIs are active against HIV-1 reverse
transcriptase only• Their use with NRTIs or protease inhibitors provide
synergistic effects against HIV due to sequential block at two different steps required for viral replication
• Adverse effects: • Skin rashes including Steven-Johnson syndrome• Elevation of liver enzymes

Efavirenz (EFV)
• It is approved for the therapy of HIV infection of adults and children and is also used for Post-exposure prophylaxis.
• It is the only NNRTI approved for once-daily dosing.
• Adverse effects: Rash, elevated liver enzymes and serum cholesterol also may occur. Central nervous system (CNS) effects in approximately half of patients may include dizziness, headache, insomnia, drowsiness, euphoria, agitation, impaired cognition, nightmares, vivid dreams, and hallucinations.
• Efavirenz should be avoided during pregnancy because primate studies have shown it to be teratogenic at doses near therapeutic levels.

Nevirapine (NVP)
• It is approved for the treatment of HIV infection in adults and children as part of a combination therapy.
• During the first 12 weeks of treatment, patients must be closely monitored for the development of potentially fatal hepatic toxicity (i.e., hepatitis, hepatic necrosis, and hepatic failure) and skin reactions (i.e., Stevens-Johnson syndrome, toxic epidermal necrolysis, and hypersensitivity reactions).
• Adverse effects: Mild to moderate rash, fever, nausea, fatigue, headache, and elevated liver enzymes.

Nucleotide reverse transcriptase inhibitors (NTRTIs):
• E.g. Tenofovir (TFV)
• Mechanism of action:• First gets hydrolysed in liver • Then gets phosphorylated to an active Tenofovir
diphosphate• This competitively inhibits HIV reverse transcriptase
enzyme and causes termination of chain elongation after getting incorporate into viral DNA

Nucleotide reverse transcriptase inhibitors (NTRTIs):
• Pharmacokinetics: • Oral bioavailability: 25% (fasting), 40% (after meals)• Distribution: PB is negligible (2-5%)• Plasma T1/2: 17 Hrs
• Excretion: Urine, 70-80% FD

Nucleotide reverse transcriptase inhibitors (NTRTIs):
• Therapeutic uses:• Used along with other anti-HIV drugs in the
treatment of HIV in adults.
• Adverse effects: • Nausea, vomiting, diarrhea, • Osteomalacia

Protease inhibitors (PIs):
• E.g. Saquinavir, Indinavir, Nelfinavir, Amprenavir, Fosamprenavir, Ritonavir, Lopinavir, Atazanavir
• Mechanims of action:• HIV protease is a viral enzyme responsible for the
cleavage of polyproteins into structural proteins and certain enzymes that are required for the final assembly of the new infectious virions.
• Protease inhibitors act by binding to the viral protease, in this way preventing the correct cleavage of viral proteins.
• Thus, they prevent HIV from being successfully assembled and released from the infected cells.

Protease inhibitors (PIs):
• Pharmacokinetics:Drug Oral
Bioavailability
Distribution Metabolism Excretion T1/2
Saquinavir-H 4 PB 97% CYP3A4, FPM Feces 85%, Urine 3% FD
8
Saquinavir-S 13 Wide, CSF nil, PB 97%
CYP3A4, FPM Feces 85%,Urine 3% FD
11
Ritonavir 75 PB 98% CYP3A4 Fecea 98%, Urine 1% FD
3-5
Lopinavir variable PB 98% CYP3A4 Mainly Feces, Urine 2% FD
5-6
Nelfinavir Variable PB 98% CYP3A4 Mainly Feces, Urine 2% FD
4-5
Indinavir 65 CSF 76%, PB 60%
CYP3A4 Feces, Urine 10% FD
1.8
Amprenavir 63 PB 90% CYP3A4 Feces 75%, Urine 15%
7-11
Atazanavir >70 CSF 3%, PB 86%
CYP3A4 Feces, Urine 7% FD
7

Protease inhibitors (PIs):
• Therapeutic uses:• Combination therapy wth Pis and other antiretroviral
drugs significantly improve the clinical efficacy by blocking HIV replication at different stages in the intracellular life cycle.
• Adverse effects: • Diarrhea, nausea, abdominal discomfort• Hyperglycemia, fat redistribution, hyperlipidemia• Bleeding episodes in hemophilics

Saquinavir (SQV)
• Saquinavir is a potent inhibitor of HIV-1 and HIV-2 protease.
• It is usually well tolerated and most frequently produces mild gastrointestinal side effects.

Ritonavir (RTV)
• Ritonavir is a potent inhibitor of HIV-1 and HIV-2 protease.
• It is not well tolerated in higher doses.• It is mainly used in low doses to increase blood
levels of other protease inhibitors and to extend their dosing interval.
• Adverse effects: Gastrointestinal side effects, altered taste sensation, paresthesias and hypertriglyceridemia.

Nelfinavir (NFV)
• It is probably the most commonly used protease inhibitor because of its low incidence of serious adverse effects.
• Adverse effetcs: Diarrhea and flatulence; these may resolve with continued use.

Entry/Fusion inhibitors:
• E.g. Enfuvirtide (T-20)
• Mechanism of action: • Binds to gp41 subunit of viral envelop glycoprotein• Thus prevents the entry of HIV-1 into CD4+ cells by
interfering with fusion of viral and cellular membrane

Entry/Fusion inhibitors:
• Pharmacokinetics:• Oral bioavailability: Poor, Hence give S/C• Distribution: PB 90%• Plasma T1/2: 3-4 Hrs
• Excretion:

Entry/Fusion inhibitors:
• Therapeutic uses:• Used along with other antiretroviral drugs for the
treatment of advanced HIV-1 infections (which is not managed despite other antiretroviral therapy)
• Adverse effects:• Local reaction (nodule) at injection site, skin rash,
eosinophilia, pneumonia like manifestation

Classification of Anti-Retroviral drugs (Anti-HIV drugs):
• The Anti-HIV drugs can be classified into
1. Nucleoside reverse transcriptase inhibitors (NRTIs): Zidovudine (AZT,ZDV), Stavudine (d4T), Lamivudine (3TC), Abacavir (ABC), Zalcitabine, Emtricitabine (FTC), Didanosine (ddI).
2. Non nucleoside reverse transcriptase inhibitors (NNRTIs): Efavirenz (EFV), Nevirapine (NVP), Delaviridine.
3. Nucleotide reverse transcriptase inhibitors (NTRTIs): Tenofovir (TDF)
4. Protease inhibitors (PIs): Saquinavir (SQV), Indinavir (IDV), Nelfinavir (NFV), Amprenavir, Fosamprenavir, Ritonavir (RTV), Lopinavir (LPV) , Atazanavir (ATV).
5. Entry/Fusion inhibitors: Enfuvirtide

WHO recommendations of ART
• WHEN TO START:• All adolescents and adults including pregnant women with
HIV infection and CD4 counts of ≤350 cells/mm3, should start ART, regardless of the presence or absence of clinical symptoms.
• Those with severe or advanced clinical disease (WHO clinical stage 3 or 4) should start ART irrespective of their CD4 cell count

WHO recommendations of ART
• WHAT TO START: • First-line therapy should consist of • NNRTI(1) + NRTIs (2), one of which should be zidovudine
(AZT) or tenofovir (TDF). • Take steps to progressively reduce the use of stavudine
(d4T) in first-line regimens because of its well-recognized toxicities.
• Second-line ART should consist of • A Ritonavir-boosted PI + NRTIs (2), one of which should
be AZT or TDF, based on what was used in first-line therapy.
• Ritonavir-boosted atazanavir (ATV/r) or lopinavir/ritonavir (LPV/r) are the preferred PIs.

HIV/TB co-infection
• ART should be initiated as soon as possible in all HIV/TB-co-infected patients with active TB
• In cases where a person needs TB and HIV treatment concurrently, first line treatment options include ZDV/3TC or D4T/3TC plus either an NNRTI or ABC.
• If an NNRTI-based regimen is used, EFV would be the preferred drug as its potential to aggravate the hepatotoxicity of TB treatment appears less than with NVP.
• Except for SQV/r, PIs are not recommended during TB treatment with Rifampicin.
• E.g: AZT or TDF (tenofovir disoproxil fumarate)
+ 3TC (or FTC(emtricitabine)) + EFV

HIV/HBV co-infection
• Irrespective of CD4 cell counts or WHO clinical stage, patients who require treatment for HBV infection should start ART.
• First-line and second-line regimens for these individuals should contain TDF and either emtricitabine (FTC) or lamivudine (3TC).
• E.g: TDF + 3TC (or FTC) + EFV

HIV+ pregnant women
• NRTIs (2) + NNRTI(1)• AZT preferred but TDF acceptable • EFV included as a NNRTI option (but do not initiate
EFV during first trimester) • Benefits of NVP outweigh risks where CD4 count is
250−350 cells/mm3
• E.g: AZT + 3TC + NVP

ART combinations that need to be avoided
• The following combinations should not be offered because of antagonism:
• AZT (Zidovudine)+ D4T (Stavudine)• DDC (Zalcitabine) + 3TC (Lamivudine)
• The following combinations should not be offered because of the overlapping toxicity profile:
• DDC (Zalcitabine) + D4T (Stavudine)• DDC (Zalcitabine) + DDI (Didanosine)

Classification of Anti-Retroviral drugs (Anti-HIV drugs):
• The Anti-HIV drugs can be classified into
1. Nucleoside reverse transcriptase inhibitors (NRTIs): Zidovudine (AZT,ZDV), Stavudine (d4T), Lamivudine (3TC), Abacavir (ABC), Zalcitabine, Emtricitabine (FTC), Didanosine (ddI).
2. Non nucleoside reverse transcriptase inhibitors (NNRTIs): Efavirenz (EFV), Nevirapine (NVP), Delaviridine.
3. Nucleotide reverse transcriptase inhibitors (NTRTIs): Tenofovir (TDF)
4. Protease inhibitors (PIs): Saquinavir (SQV), Indinavir (IDV), Nelfinavir (NFV), Amprenavir, Fosamprenavir, Ritonavir (RTV), Lopinavir (LPV) , Atazanavir (ATV).
5. Entry/Fusion inhibitors: Enfuvirtide

THANK YOU