Embed Size (px)
Citation preview

Anomalous Innervations
• Presented by Syed Irshad Murtaza
• Neurophysiology Department• Dr. Ziauddin University Hospital,• Clifton Campus, Karachi.
• 20-10-2015
Martin Gruber Anastomosis, Accessory Peroneal Anastomosis.

Anomalous Innervations
• What is anomaly?• a·nom·a·ly (-nm-l) n:Gk, anomalos, irregular• A deviation from what is regarded as normal• or norm• Or• Marked deviation from normal, especially as• a result of congenital or hereditary defects.• anomalous, adj

Why is Important to know?
• If these conditions (anomalies) are not recognized, they may easily be mistaken for technical fault & abnormalities or, in some cases, for actual pathology which would not be existing in actual.

TYPES of Anomalies• A- Upper limb anomalous innervations• Martin – Gruber Anastomosis• (Median to Ulnar anastomosis)• All Ulnar- hand innervations• Ulnar to median anastomosis• Superficial Radial nerve innervations on• dorsum of the hand• B-Lower limb anomalous innervations• Accessory Peroneal nerve• Tibial to Peroneal anastomosis

Martin- Gruber anastomosis (MGA)• It is most common anomalous innervation in• upper limb.• Present in 15 – 30 % of patients.• It is manifested by cross over of median-to ulnar• fibers.• Cross over commonly occurs in mid forearm• either from the main trunk of median nerve or from• one of its branches (most commonly anterior• interosseus nerve).• It may present unilaterally or bilaterally.• It involves only motor fibers while sensory are spared.

ANATOMY• Pathway and Innervation!• After cross over in the mid forearm, median fibers run with
the distal ulnar nerve to innervate any of the following ulnar muscles:
• 1. Innervation to hypothenar muscles(abductor digiti minimi).• 2. Innervation to FDI muscle.• 3. Innervation to the ulnar innervated thenar muscles.• 4. Combination of these.

When & how MGA is Recognized ?
• 1. During routine ulnar conduction studies.• 2. During ulnar conduction studies when recorded
from FDI.• 3. During routine median studies recording from
APB.• 4. When co- existent CTS study is performed.

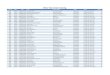
Routine Ulnar Conduction Study• If anastomotic fibers innervate abductor digiti• Minimi (ADM) > 10 % drop in CMAP amplitude is• noted between wrist and below elbow• stimulation sites. ( Higher amplitudes are seen• with distal stimulation).• Median nerve stimulation should be performedat the wrist and at the antecubital fossa (AF) while recording the hypothenar muscles (ADQ).

Anastomosis (Crossing over of Fibers

NCS recording from ADQ muscle




Marinacci communication (ulnar-to-median anastomosis in the forearm)
• Prevalence of MGA, an anomalous median-to-ulnar forearm communication, is well reported in literature while Marinacci communication, the reverse of Martin-
• Gruber with forearm ulnar-to-median communication is underrecognized . Marinacci (in 1964) first reported patient who, following trauma to the median nerve at the forearm, had preservation of median nerve innervated
• hand muscles despite denervation of forearm flexors.• Marinacci communication involving only sensory nerve fibers rise from the
median nerve distally to ulnar nerve proximally has been reported. In the patient, reported by Hopf , that the nerve action potentials evoked by
• stimulation of the middle finger (ulnar side) and the ring finger (radial side) digital nerves were propagated with the median nerve at the wrist and the ulnar nerve at the elbow.

Differential Diagnosis of MGA• The differential diagnosis of this pattern (i.e. higher
amplitude distally than proximally) includes the following.
• 1. Excessive stimulation of the ulnar nerve at the wrist resulting in co-stimulation of the median nerve.
• 2. Submaximal stimulation of the ulnar nerve at the below-elbow site.
• 3. Conduction block of the ulnar nerve between the wrist and below-elbow sites, or
• 4. An MGA with crossing fibers innervation the hypothenar muscles.

Cont’d• If no MGA is present, a small positive deflection
usually is recorded with both the wrist and antecubital fossa stimulation sites, reflecting a volume conducted potential from median muscles.
• If an MGA is present, a small positive volume conducted potential will be present with median nerve stimulation at wrist, however, median stimulation at the antecubital fossa will evoke a small CMAM over the abductor digiti minimi.

Cont’d• The amplitude of the CMAP evoked by
stimulating the median nerve at the ante-cubital fossa (Recording the hypothenar muscles) will approximately equal the difference between the CMAP amplitudes evoked with ulnar nerve stimulation at the wrist and below-elbow sites (recording the hypothenar muscles).
• If its not identified, it may give a false impression of technical fault or conduction block.

NCS Recording from ADQ

Recording from ADQ muscle

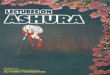
Cross Over of Median to Ulnar Fibers Supplying FDI
• If anastomotic fibers innervate FDI, >10% of amplitude drop occurs between stimulation at the wrist and below-elbow site. Higher amplitude being found by distal stimulation.
• It may give a false impression of technical mistake or conduction block.
• Q. When NCS is needed to perform from FDI?

How to Confirm MGA?
• After ruling out the technical faults, median nerve is stimulated at wrist and at ante-cubital fossa while recording from FDI.
• Higher amplitude CMAP is recorded with proximal stimulation than with wrist stimulation in case of MGA.
• The difference between wrist and antecubital fossa stimulations approximates the drop in amplitude between proximal and distal stimulation sites when stimulating ulnar nerves.

Riche-Cannieu anastomosis
• Riche-Cannieu anastomosis (ulnar-to-median anastomosis in the hand)
• In the hand, Riche (1897) and Cannieu (1897) described a neural connection between the deep branch of the ulnar nerve and the recurrent branch of the median nerve at the
• thenar eminence

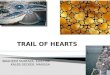
Cross over of median and ulnar fibers

NCS recording from FDI muscle.

• Cross over of median-to-ulnar fibers innervating any of the ulnar innervated thenar muscles.
• Abductor pollicis and deep head of flexor pollicis brevis are ulnar nerve innervated thenar muscles.
• When these muscles are innervated by MGA, median motor studies show a characteristic pattern of higher CMAP amplitudes with proximal median stimulation than distal stimulation.

NCS Recording from APB muscle.

How to confirm MGA• After ruling out the technical faults, ulnar nerve
is stimulated at the wrist and below elbow sites while recording from thenar muscles.
• Normally it results in a CMAP (due to ulnar innervated muscles in thenar eminence) of almost same amplitude, with proximal as well as distal stimulation.
• If an MGA is present, CMAP amplitude is lower with proximal stimulation.

MGA

How to Confirm MGA• After ruling out the technical faults, ulnar nerve
is stimulated at the wrist and below elbow sites while recording from thenar muscles.
• Normally it results in a CMAP (due to ulnar innervated muscles in thenar eminence) of almost same amplitude, with proximal as well as distal stimulation.
• If an MGA is present, CMAP amplitude is lower with proximal stimulation.

MGA with co existent CTS
• As both of these conditions are common, so they might be seen existing together.
• Co existence of both the conditions should be suspected when proximal median nerve stimulation gives a more positive deflection at the thenar eminence along with fast conduction velocity.
• In some cases of severe CTS, proximal latency may be shorter than the distal latency.

MGA with co existent CTS

Needle EMG in case of MGA
• In this situation, unexpected results may be seen creating confusion in interpretation. For example
• In cases of median nerve dysfunction at the antecubital site, EMG may show abnormal findings in ulnar innervated muscles.
• In cases of ulnar neuropathy, some of the ulnar innervated muscles may be spared on EMG examination.

All Ulnar Hand Innervation
• Among the anomalies are cases of the all-ulnar hand innervation. In rare individuals, all or most of the intrinsic hand musculature is innervated by the ulnar nerve. In these individuals, an ulnar nerve lesion at the elbow may cause much more dysfunction in the hand than one typically expects to see.
•

Anomalous innervation b/w superficial Radial and Dorsal Ulnar Cutaneous sensory nerves
• In the upper extremity, an anomalous innervation b/w the superficial radial and the dorsal ulnar cutaneous sensory nerves has been described. Normally, sensation to the dorsum of the hand is mediated by both nerves; the little and ring fingers and medial hand by the dorsal ulnar cutaneous nerves, and the remainder by the superficial radial nerve. In rare individuals, the superficial radial nerve innervated the entire territory.

NCS Recording from Sup. Radial v/s DUC
• During nerve conduction studies, this situation may present as an apparently absent response recording the dorsal ulnar cutaneous sensory nerves.
• The anomaly can be demonstrated by stimulating the superficial radial nerves in the lateral forearm, with recording electrodes placed over the dorsal ulnar cutaneous nerve territory.

Radial to DUC crossing

Accessory deep peroneal nerve• The deep peroneal nerve, a major branch of the common peroneal
nerve, usually innervates the EDB. In 21-28% of subjects, this muscle also receives innervation from the accessory deep peroneal nerve, an anomalous branch of the superficial peroneal nerve.
• This anomaly should be suspected when proximal stimulation of the common peroneal nerve at the knee elicits higher amplitude CMAP, than stimulation of the deep peroneal nerve at the ankle. Stimulation of the accessory deep peroneal nerve behind the lateral malleolus activates the anomalously innervated lateral portion of the EDB.
• Rarely, this anomalous branch may exclusively supply the EDB. In the presence of this anomaly, the lesions of the deep peroneal nerve spare the lateral portion or the whole of the EDB, thus leading to the possibility of an incorrect conclusion.



Accessory Peroneal
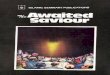
Peroneal motor NCS
Recording Site : EDBSTIMULUS SITE LAT1 DUR AMP AREA ms ms mV mVmsA1: Ankle 5.2 10.6 1.260 3.392A2: Below Fib. head 11.8 10.7 2.641 8.191A3: Above Fib. head 15.1 11.7 2.428 8.610A4: Behind lat. mall 4.9 11.1 1.578 5.331
SEGMENT DIST DIFF CV ms ms m / sAnkle-Below Fib. head 325 6.6 49Below Fib. h-Above Fib. h 225 3.3 68

Tibial to Peroneal anastomosis
• In addition, there are rare isolated case reports of tibial to peroneal and ulnar to median anastomosis. If an unusual or unexpected nerve conduction pattern is seen, one should always consider not only technical factors but also the possibility of an anomalous innervation.



,.

References• Electromyography and Neuromuscular Disordersby David C Preston MD• Clinical Electromyography: Nerve Conduction
Studies &• Principles of Clinical Electromyography by Shin J. Oh, MD• Electrodiagnosis in Diseases of Nerve and Muscleby Jun Kimura MD
AKUH Karachi and Dr.Ziauddin University Hospital, Clifton Campus Karachi, Neurophysiology Department Specific
Techniques, Protocols and Methods of Performing NCS/EMG with Normative Data.