Embed Size (px)
Citation preview

EFTC 2009: Eyes on the futurereview of the conference
Anne Goossensen
Researcher at Erasmus Universiteit (Health Policy and Management) & Professor Substance Abuse Treatment INHolland (Practice) University.

Opening: participation of 27 countries

Content of the congress
Overwhealming amount of information:
Meetings at welcome reception
8 Plenaries with 16 lectures
51 workshops in 5 themes
3 site visits with different treatment programmes each
3 Films
Meetings at Gala dinner
And different satellite activities, like physicians meeting

Focus of the review
Leading Questions / issue:
Eyes on the future. Who’s future? Of the TC’s? Of the professionals?
Of the patients? (Teeuwisse)
1. Effectiveness issue
2. Policy issue
3. Innovation issue
4. Therapy methods issue
5. Special populations issue
6. Spirituality issue

1. Effectiveness issue / right of existence
Cochrane Collaboration shows little effectiveness
De Leon presents evidence from other types of research
For many psycho-social elements in TC’s there is evidence (like
reïnforcement, peer mentoring en role modeling)
An RCT just not fits on a TC
Not being able to measure is something else than not effective
It is clear that the EBM research paradigm fits not to TC’s
Other evaluation studies are possible, and should be done more
Evaluation of the method (WHAT people do)
Namely HOW they do it
That points to the relationship as a critical succes factor
That should be included in an evaluation frame

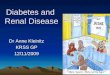
What causes effect in psychotherapy?
15%
40%
40%
15%Relationship
Used methods
Factors outside therapy

1. Effectiveness issue / right of existence
This was a main issue through the conference
If TC’s want to continue existing an ANSWER is necessary
To evidence based financing structures

2. Policy issue
As a movement: are we connected, disconnected or unknown (Turner)?
Not connected to important organizations
A critical succes factor for the future
At European level, but also national and regional
Very strong regional networks / care chains, where TC’s are imbedded
in – a strong point
Clear description of the goal population helps matching regional patient
to treatment
Furthermore there seem to be different languages between the TC
movement and other parties, here bridges can and have to be built

3.Innovation issue
How can TC’s innovate & grow?
Community as a method – the basic idea
Standards / manualized / therapeutic integrity
Fidelity to the model
Checking by audit through other TC members
For me this is again only the WHAT part of the story
Thinking of two brain hemispheres
One side: mental, logical reasonable, manuals, protocols and models
The other side: emotions, creativity, intuition, relating, ‘warmth’
Innovations should affect both sides: logic and love
Let’s try to avoid focus only on the mental/logical side

4. Therapy issue
Encounter groups
Running Therapy
Multidimensional Family Therapy
Self-help
Bonding Therapy
Aftercare and Rehabilitation
Movement Therapy
Wilderness Therapy
Reflecting Art Therapy
Motivation methods
Schema Focus Therapy
Website focussed on learning (Digital Community)

5. Special populations issue?
TC and Justice - Culture clashes
Making a whole prison a TC!
About dual diagnosis in general
About ADHD
About youngsters
Integrate knowledge on new subgroups
In existing model
Keep up with new information

6. Spirituality issue
My psychology thesis was about addiction care and spirituality
What is meant with spirituality?
12 steps and the higher power?
Giving meaning?
Definition of Eric Broeckaert?
Unique relationships, ecologicaly and systemic interconnected?
Interiorization of life events & experiencing a new life style?
Mindfulness?

Eyes on the future: being present in relationships!
The TC is an unique setting in terms of:
Forming deep and healing relationships
Ability to work through trauma and attachment difficulties
And thereby change lives, change identities of persons
Enable turning points in (family) histories of addiction
Spirituality can help to realize and optimize this power of relationships in
the TC
For instance by mindfulness, the power of attention, becoming
present for professionals and patients
Professionals can improve in relating by practising mindfulness,
becoming at ease in the here and now

Eyes on the future: being present in relationships!
Innovation can happen by:
Performing (effect) research also from a relation focused
perspective
Educating professionals in quality of relationship building and
communication
There are concepts and validated research instruments available
Combine fidelity work with relation improvement work
Perform bonding groups
Teaching mindfulness to staff and patients

Eyes on the future: being present in relationships!
Disconnectedness at policy level may be repaired by:
Communicate about relation based work as identity of TC’s
Educate parties about the deeper healing options
Describe and communicatie which patients groups fit to a TC
Make TC’s part of the care chain
Show results from relation based research besides EBM

Eyes on the future: becoming present in relationships!
In short:
Nowadays professionals will not have the changing experiences of
those who initiated the TC’s
But new generations can aim at the same attainments with new
concepts
Relationship building is such a concept, as an offer to let patients heal
themselves while relating to the community
Mindfulness (being present) is such a new and powerful concept that
enables professionals nowadays to ‘be’ a TC and not just ‘run it’ (De
Leon)

Thank you for your attention!
For Blogs:
www.verslavingskundeplein.nl