Embed Size (px)
Citation preview

Anna Tzontcheva, MD, PhDAnna Tzontcheva, MD, PhDChair of Clinical Laboratory and Clinical Chair of Clinical Laboratory and Clinical
immunology, immunology, Medical University – Sofia, BulgariaMedical University – Sofia, Bulgaria
Abdominal obesity, diabetes and cardiovascular risk
15th BCLF Congress, 4-7 September 2007Antalya, Turkey

• Obesity, particularly intra-abdominal (visceral) obesity, is a leading cause of cardiovascular disease (CVD), insulin resistance, type 2 diabetes, dyslipidaemia, inflammation and thrombosis.
• A useful indicator for visceral fat is waist circumference, which is associated with all-cause mortality. Pro-inflammatory adipokines play a causal role in the development of pathologies associated with insulin resistance, type 2 diabetes and CVD.




Hormonal Control of Eating
Ghrelin: made in response to an empty stomach.PYY: made in response to food entering the small intestine.


Obesity
The epidemic
Hypotheses about the causes
Environment
Behavior
Biology



Changing Portion Sizes
National Geographic, August 2004
2004
20042004
2004
2004






















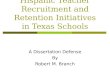
The Fat Cell Is a Veritable Endocrine Factory
Leptin
Adiponectin Resistin
Angiotensinogen
IL-6
TNF-Alfa Cortisol
Stored Triglycerides
• Fat cells are continually absorbing or releasing substances in response to the body’s energy needs
• Fat cells are better adapted to preserving calories than shedding them
Source: Underwood A, Adler J, Hand K, Ulick J. What You Don’t Know About Fat. Newsweek. 2004;144:40-47.
Fat Cell


Adiponectin
• A protein is also called ADIPOQ, gelatine-binding 28, Acrp30, discovered in 1995.
• A peptide hormone made by adipocytes in response to high fat reserves:
Increases FA uptake by myocytes and the rate of FA oxidation.
Slows FA synthesis in the liver.
Slows gluconeogenesis in the liver.
Acts through AMP-dependent protein kinase (AMPK).
• Humans who are obese or who suffer from Type II diabetes show reduced levels of adiponectin.
• Drugs (thiazolidinediones) used to treat Type II diabetes elevate expression of adiponectin.

Adiponectin - structure

Adiponectin action : activation AMPK


Molecular Mechanisms of Adiponectin Action
Kadowaki et al. Endocrine Reviews 26 (3): 439 - 451, 2005

Adiponectin R1 and R2 are Expressed in Heart, Liver, Kidney, Skeletal Muscle and Other Tissues
1. Brain2. Heart3. Kidney4. Liver5. Lung6. Skeletal Muscle7. Spleen8. Testis
Yamauchi T., et al Nature 423, 762-769


Leptin Action
• Suppresses appetite via production of -melanocyte-stimulating (-MSH) hormone, which triggers the next neuron in the circuit to send the “Stop eating!” signal.
• Stimulates the sympathetic nervous system:
Increases bp.
Increases heart rate.
Increases thermogenesis via uncoupling of electron transport.
• Leptin production depends on the number and size of adipocytes.



PI3 Kinas
e

Resistin
Protein
Produced in adipocytes
Family of proteins with C-terminal rich of cysteine
The invention of resistin as a novel factor secreted by fat cells with an impact on insulin sensitivity was proposed as a new mechanism to explain the pathogenic sequence of adipocyte-obesity-insulin resistance. Resistin is a cysteine-rich 12.5 kDa polypeptide, with unclear role in the pathogenesis of obesity- mediated insulin resistance and type 2 diabetes mellitus. Recent studies in murine models suggest that resistin (also called Fizz3), secreted by adipocytes, may represent the long-sought link between obesity and insulin resistance.

Visfatin
In 2004, Fukuhara et al. identified a molecule that is expressed at much higher levels invisceral fat than in subcutaneous fat which was named visfatin [27]. This adipokine ishighly expressed in the visceral adipose tissue of both humans and rodents. Visfatin was
Visfatin
• In 2004, Fukuhara et al. identified a molecule that is expressed at much higher levels in visceral fat than in subcutaneous fat which was named visfatin .
• This adipokine is highly expressed in the visceral adipose tissue of both humans and rodents. Visfatin was found to be identical to a cytokine expressed by lymphocytes - the pre-B cell colony-enhancing factor (PBEF).
• Visfatin binds to the insulin receptor at a site distinct from insulin and exerts hypoglycemic effect by reducing glucose release from hepatocytes and stimulating glucose utilization in peripheral tissues.
• Since insulin-mimetic actions of visfatin may be part of the feedback regulation of glucose homeostasis, a hypothesis may be raised that visfatin concentrations are influenced by glucose or insulin blood levels in humans. This possibility offers new therapeutic options for diabetics.





IL6
PAI-1TNF
adiponectinleptin
Insulin sensitivity insulin resistance
Vascular inflammation endothelial dysfunction
Adipokines Mediate Insulin Resistance and Inflammation
angiotensinogen
FFA
visfatin


Metabolic Syndrom - Diagnostic Criteria
WHO,1999Hyperglycemia or
Insulin resistance plus 2
or more of:
• Obesity: W/H>0.9 (M), 0.85(F) or BMI>30
• Dyslipidaemia: TG1.7 or HDL<0.9(M),1.0(F)
NCEP,ATPIII,2001
Three or more of:• Central obesity: waist >102
(M), 88 (F)
• Hypertriglyceridaemia:
– Triglyceride 1.7
– Low HDL: <1.0 (M),1.3(F)
• Hypertension:
- Blood pressure>135/85 or
Treatment
• Fasting glucose >6.1
• Hypertension:Hypertension:
- Blood pressure >140/90mmHg- Blood pressure >140/90mmHg
• Microalbuminuria:Microalbuminuria:
Albumin excretion >20µg/minAlbumin excretion >20µg/min

Proposed IDF Criteria 2005 (a)
Central ObesityWaist circumference (ethnic specific)
Plus two (2) of the following:• Raised triglyceride (>1.7 mmol/l)• Reduced HDL (<1.03 mmol/l,M) (<1.29 mmol/l,F)• Raised blood pressure (>130systolic or >85 diastolic)• Fasting glucose >5.6 mmol/l
• Diagnosed T2DM• Treated hypertension• Treated dyslipidaemia






Insulin ResistanceInsulin Resistance
Endothelial Endothelial DysfunctionDysfunction
TG, HDLTG, HDL--CC
sd LDLsd LDL--CC
Hypertension Hypertension
Uric Acid Uric Acid
PAIPAI--1 1
InflammationInflammation
ThrombosisThrombosis
OxidationOxidation
AtherosclerosisAtherosclerosis AtherosclerosisAtherosclerosis
Unstable plaque Unstable plaque
Inflammation, Fibrosis CapInflammation, Fibrosis Cap
Thrombosis and RuptureThrombosis and Rupture
EventEvent
HyperinsulinemiaHyperinsulinemia Metabolic SyndromeMetabolic Syndrome Impaired GlucoseToleraneImpaired GlucoseTolerane Type 2 DiabetesType 2 Diabetes
Hsueh WA, Law R. AJC, 2003
Process of Atherosclerosis in Insulin Resistance


Adapted from Steinberg H et al. Diabetes. 2000;49:1231.
InsulinInsulin NO productionVascular dilationNO production
Vascular dilationShear stressShear stress
Increased visceral fatIncreased visceral fat
Increased lipolysisIncreased lipolysis
Increased FFA levelsIncreased FFA levels
--
EndotheliumEndothelium
Increased TNFIncreased TNF
--
Decreased adiponectinDecreased adiponectin
--
FFA and Adipokines inEndothelial Dysfunction






0
5
10
15
20
25
Elevated CRP Levels in Obesity: NHANES 1988-1994
Visser M et al. JAMA 1999;282:2131-2135.
Normal
Perc
en
t w
ith C
RP
0.2
2
mg/d
L
Overweight Obese

0,00
0,50
1,00
1,50
2,00
2,50
3,00
0,0
1,0
2,0
3,0
4,0
5,0
6,0
7,0
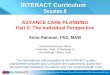
Effects of Weight Loss in Obese Women on IL-6, TNF-, and CRP
Bastard J-P et al. J Clin Endocrinol Metab 2000;85:3338-3342.
pg/m
L mg
/L
IL-6 TNF- CRP
Before diet
After very low calorie diet (mean BMI reduction 2.1 kg/m2; mean reduction in body fat mass 4 kg)
p=0.05
p=0.6
p=0.14

The Science of Obesity Is Complex and in Its Infancy
1994 – Leptin was discovered at Rockefeller University
“We like to think that eating is a voluntary act. But the amount you eat is controlled in part by how much fat you have.”
– Dr. Michael Schwartz, University of Washington
Researchers and scientists took a fresh look at obesity – was it more than a reflection of greed and weak will?
Sources: Rockefeller Researchers Clone Gene for Obesity. December 1, 1994. Available at: http://www.healthpolitics.com/home.asp?show=all. Underwood A, Adler J, Hand K, Ulick J. What You Don’t Know About Fat. Newsweek. 2004;144:40-47.

CONCLUSIONS
Visceral fat, in particular, is responsible for risk factors for diabetes and cardiovascular disease.
Visceral fat will be an important target for the reduction in the morbidity and mortality associated with multiple risk factors and the metabolic syndrome.


“In the human body, as in the world, if you control fuel resources, you influence a lot of other things as well.”
– Dr. Gökhan Hotamisligil, Harvard School of Public Health

Thank you !
Thank you !