Embed Size (px)
Citation preview
DEFINITIONThe National Kidney Foundation and the Kidney Disease Outcomes
Quality Initiative define chronic renal disease as the
structural or functional renal tissue damage lasting for over
three months, manifested by structural or functional abnormalities,
or by a drop in the glomerular filtration rate less than 60ml/kg/1.73m2.
Any drop below this level represents a loss of more than 50% of the renal function in an adult and is associated with an increased risk of disease progression
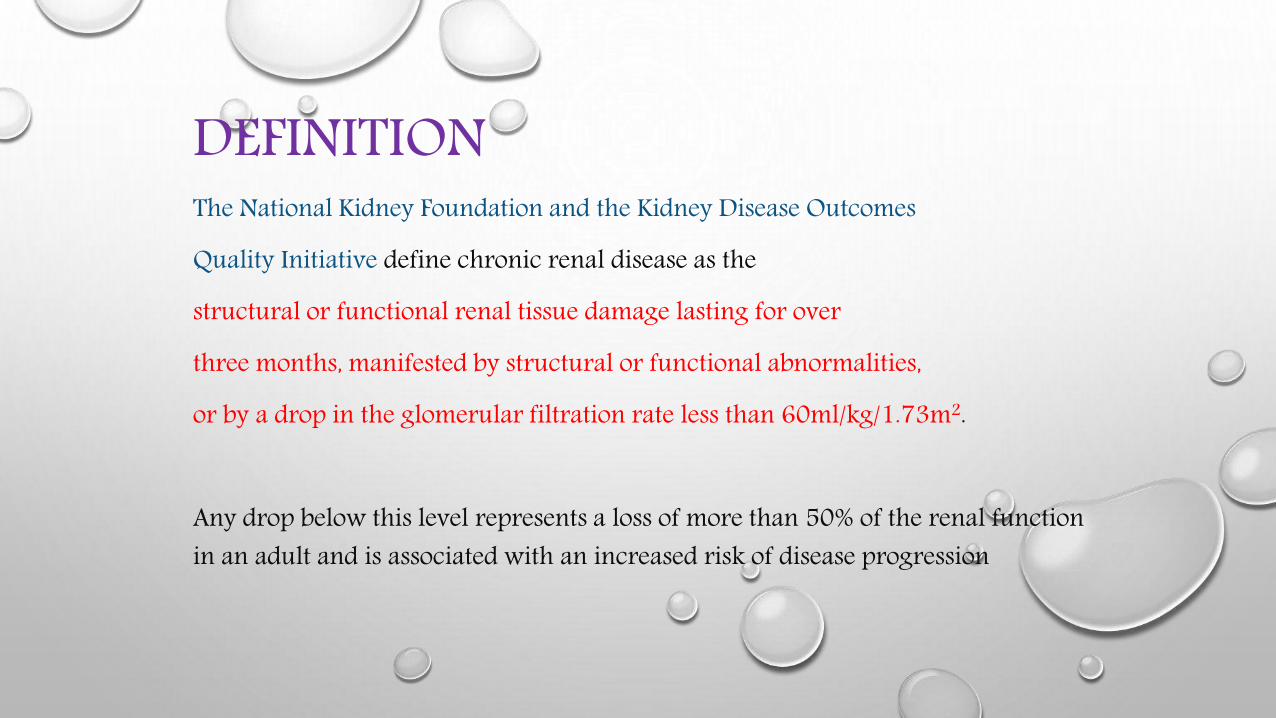
CLASSIFICATION OF CHRONIC KIDNEYDISEASE (CKD)
STAGE GFR, ml/min per 1.73 M2
0 >90*1 ≥90**2 60–893 30–594 15–295 <15
*WITH RISK FACTORS FOR CKD .**WITH DEMONSTRATED KIDNEY DAMAGE (e.g., PERSISTENT PROTEINURIA, ABNORMAL URINE SEDIMENT, ABNORMAL BLOOD AND URINE CHEMISTRY, ABNORMAL IMAGING STUDIES).
SOURCE: MODIFIED FROM NATIONAL KIDNEY FOUNDATION. K/DOQI CLINICAL PRACTICE,GUIDELINES FOR CHRONIC KIDNEY DISEASE: EVALUATION, CLASSIFICATION AND STRATIFICATION. AM J KIDNEY DIS 39:SUPPL 1, 2002.
LEADING CATEGORIES OF ETIOLOGIESOF CKD*
DIABETIC GLOMERULAR DISEASE (30%)GLOMERULONEPHRITIS
HYPERTENSIVE NEPHROPATHYPRIMARY GLOMERULOPATHY WITH HYPERTENSION
VASCULAR AND ISCHEMIC RENAL DISEASEAUTOSOMAL DOMINANT POLYCYSTIC KIDNEY DISEASE
OTHER CYSTIC AND TUBULOINTERSTITIAL NEPHROPATHY
*relative contribution of each category varies with geographic region.
Complications of CKD
Cardiovascular system
• Salt and water retention, hypertension, and LVH• Cardiomyopathy, congestive cardiac failure, • Accelerated Atherosclerosis and stiffening of large arteries• Altered lipoprotein metabolism• Uraemic pericarditis• Cardiovascular autonomic neuropathy with reduced baroreceptor sensitivity,
sympathetic hyperactivity, and parasympathetic dysfunction• Anaemia
Complications of CKD contd..Metabolic acidosis• Bone resorption• Muscle wasting, growth retardationMusculoskeletal system• Renal osteodystrophy• Rhabdomyolysis after major surgeryEndocrine system• Secondary and tertiary hyperparathyroidism, vitamin D deficiency• Diabetes mellitusGastrointestinal system• Delayed gastric emptying• Anorexia, vomiting, malnutrition• Reduced calcium absorption
Complications of CKD contd…Immune system• Immunosuppression due to uraemia or drugsFluid and electrolyte homeostasis• Hyperkalaemia• Volume overload• DehydrationNeurological abnormalities• CNS changes : mild personality changes to asterixis, myoclonus, encephalopathy and convulsions.• Peripheral neuropathy, glove and stocking sensory loss progressing to motor changes Haemostasis and coagulation• Uraemic thrombocytopathy• Prothrombotic tendency/hypercoagulation and reduced fibrinolysis• Vascular access thrombosis
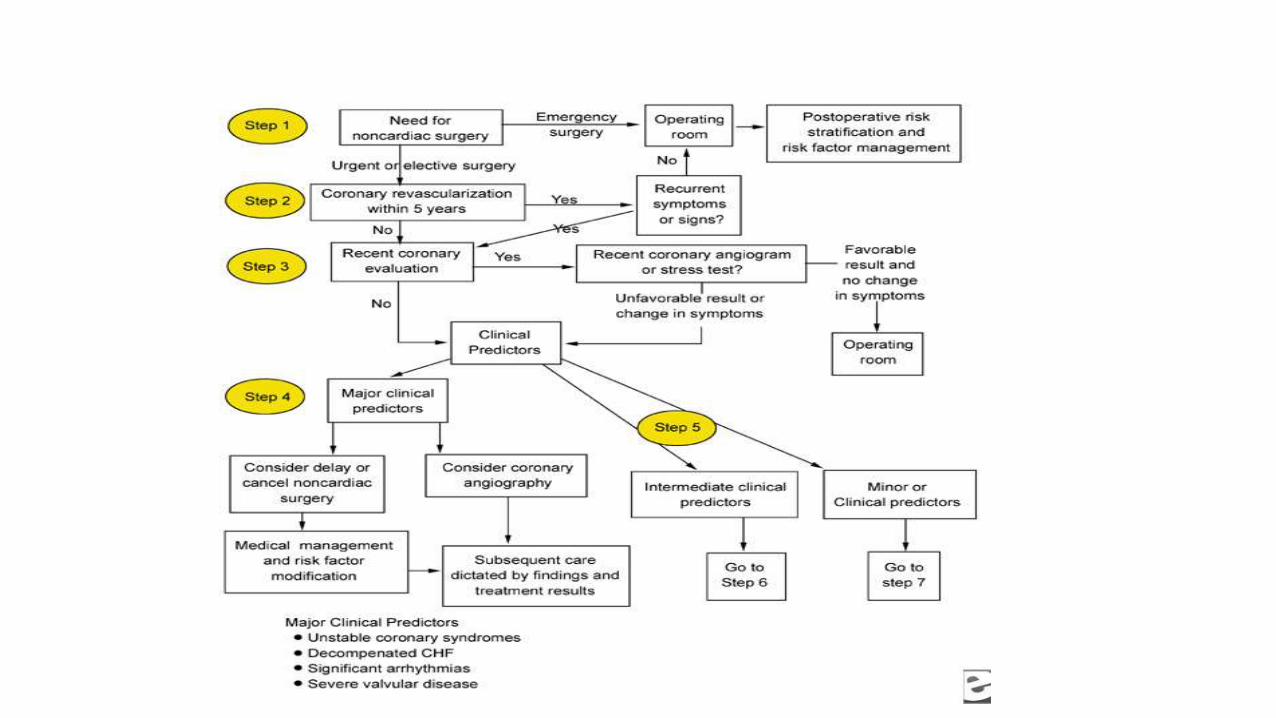
PREOPERATIVE EVALUATION• Whichever the type of surgery (emergency or programmed),the clinical history must be
carefully recorded.
• The clinical and paraclinical evaluation is limited to simple clinical data (i.e., vital signs, general aspect, signs of hypervolemia) and simple paraclinical data such as blood test, electrolytes (sodium, potassium, calcium and phosphorus), uroanalysis, coagulation status, serum creatinine and electrocardiogram.
• The clinical record shall address active cardiac conditions (active or recent acute myocardial infarction, decompensated heart failure, severe valve disease and complicated arrhythmias).
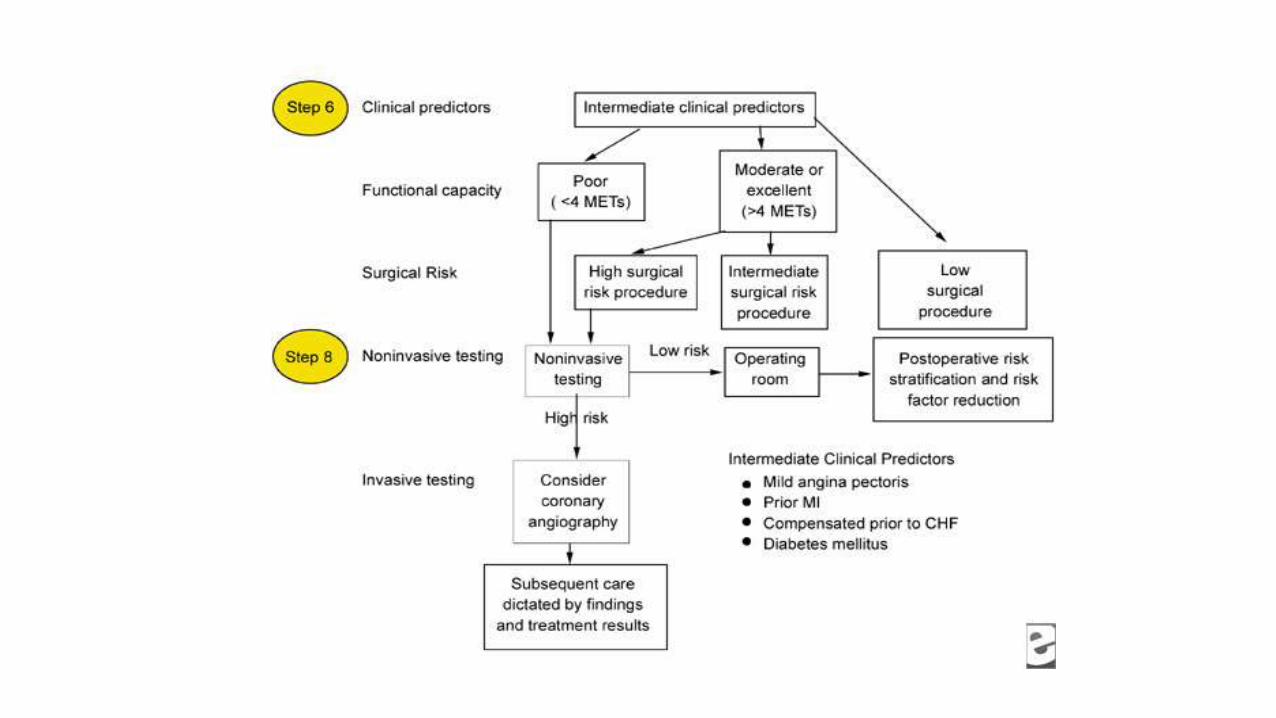
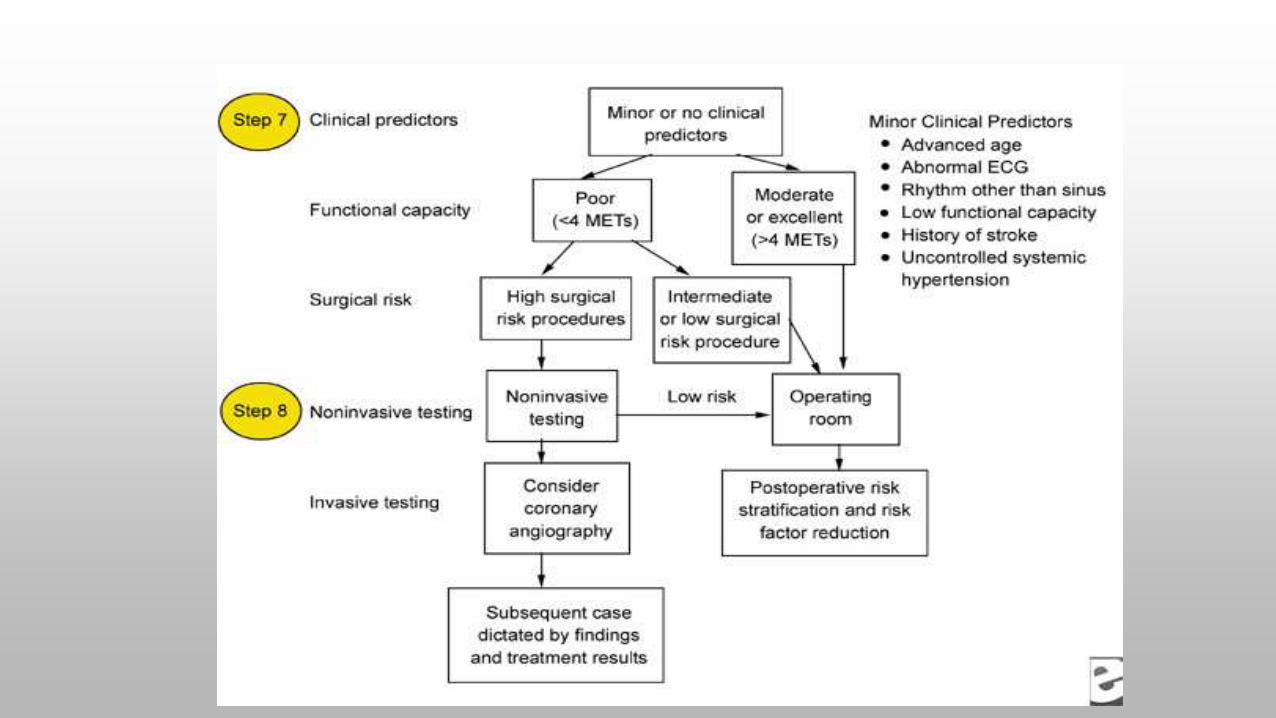
• The functional capacity should be established, expressed in metabolic equivalents (METs), according to the classification of the American Heart Society (AHA)
• Patients with a functional capacity <4 METs usually require additional studies to assess the cardiovascular risk such as the dipyridamole scan or Dobutamine stress echocardiography.
ANAESTHETIC PROBLEMS & CONCERNS• Low oxygen carrying capacity
• Fluid homeostasis -Hypotension, hypovolemia, CHF, HTN, pulmonary edema, hypoalbuminemia
• Electrolyte disturbances - Hyperkalemia, hypocalcemia
• Acid-base disturbances - Metabolic acidosis
• Arrhythmias, conduction blocks
• Immunosuppression
• Delayed gastric emptying
• Delayed drug excretion
• Bleeding tendencies
• Care of shunt , difficult venous access
• Hepatitis carrier
Pharmacology
• In patients with CKD, the effect of altered clearance, the production and accumulation of active metabolites, and the risk of aggravating pre-existing kidney disease on drug administration must be considered.
• Dose adjustment is not usually necessary until the GFR is <50 ml/min/1.73 m2
LOCAL ANAESTHETICS
L.A. have two plasma protein binding sites: a high affinity, low capacity site on AAG (α1-acid glycoprotein) and a low affinity, high capacity site on albumin.
The albumin binding site becomes increasingly important as the plasma concentration of the local anaesthetic increases.
Metabolic acidosis increases the percentage of unbound drug and this effect is more pronounced with bupivacaine.
The effect of these changes on the toxicity of local anaesthetics is unclear.
Inhalation Agents
• “All inhalation agents bio-transformed to non-volatile products of metabolism which are eliminated by kidney , but reversal of CNS effect depends upon pulmonary excretion”.
• All inhalation agents causes transient reversible ↓ of GFR, RBF, U/O, renal auto regulation.
Miller RD. Anesthesia. 7th ed., Anesthesia and the renal and genitourinary systems, page 2113.
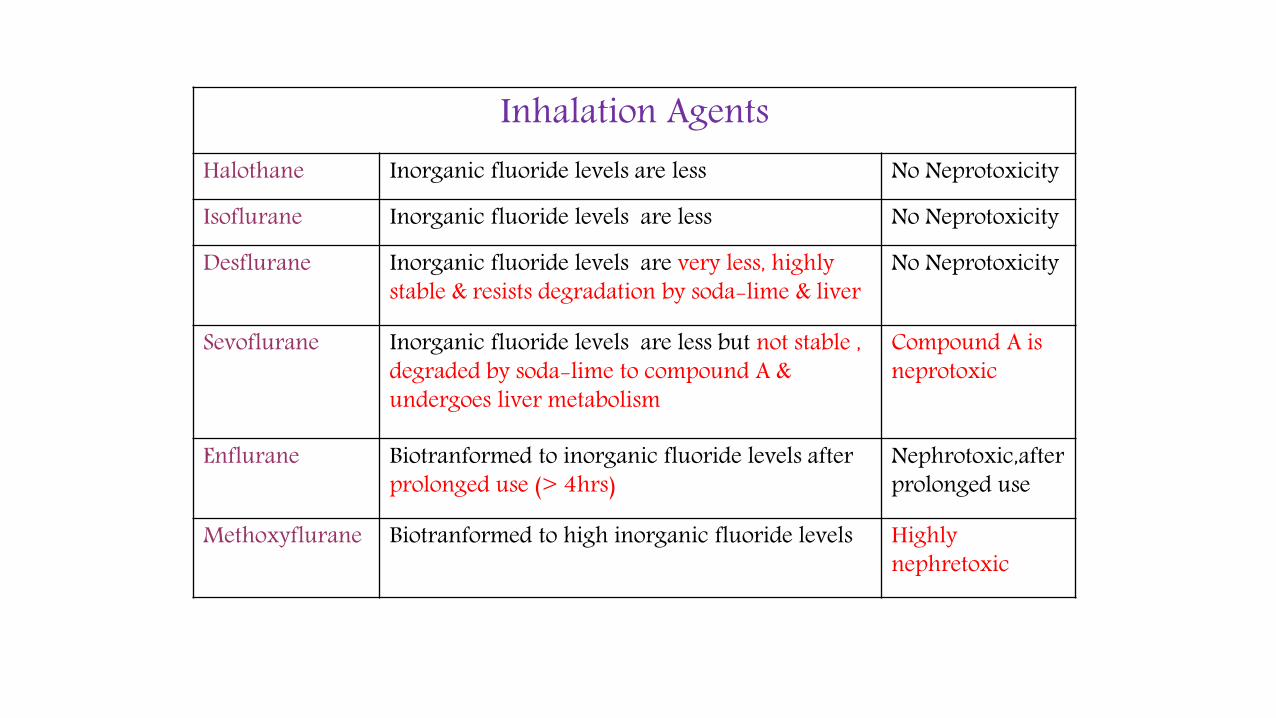
Inhalation Agents Halothane Inorganic fluoride levels are less No Neprotoxicity
Isoflurane Inorganic fluoride levels are less No Neprotoxicity
Desflurane Inorganic fluoride levels are very less, highly stable & resists degradation by soda-lime & liver
No Neprotoxicity
Sevoflurane Inorganic fluoride levels are less but not stable , degraded by soda-lime to compound A & undergoes liver metabolism
Compound A is neprotoxic
Enflurane Biotranformed to inorganic fluoride levels after prolonged use (> 4hrs)
Nephrotoxic,afterprolonged use
Methoxyflurane Biotranformed to high inorganic fluoride levels Highly nephretoxic
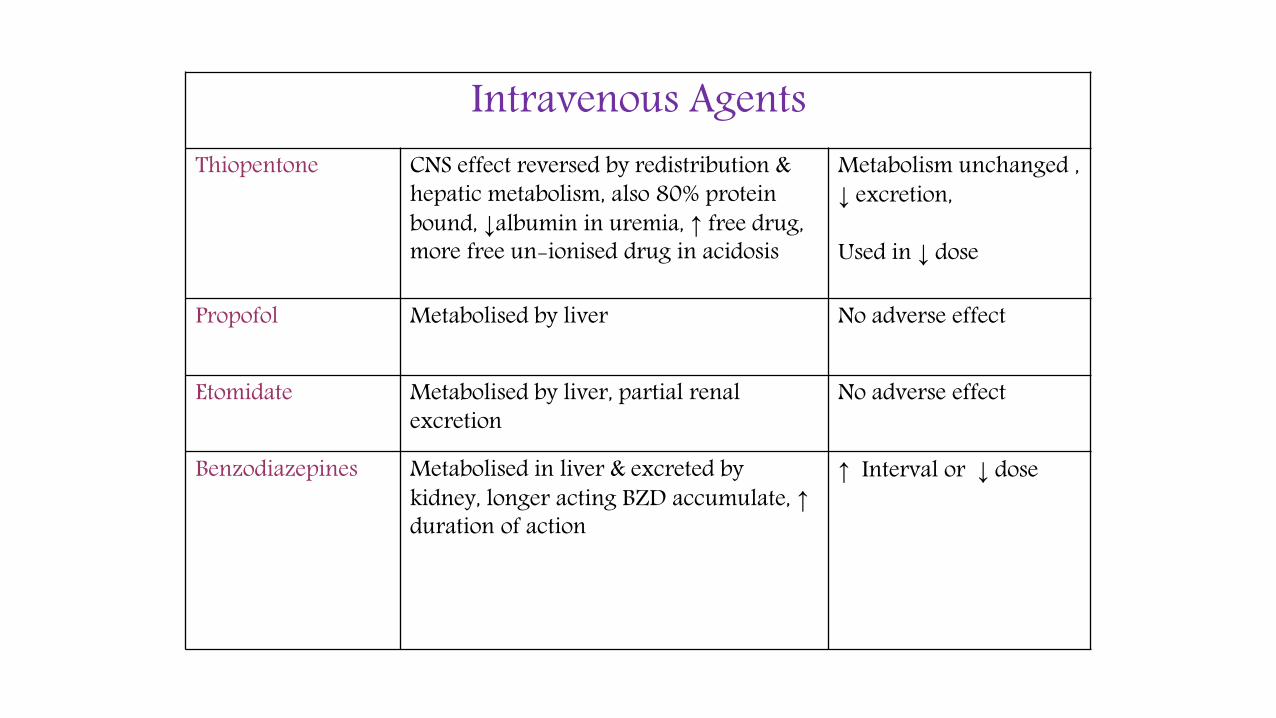
Intravenous AgentsThiopentone CNS effect reversed by redistribution &
hepatic metabolism, also 80% protein bound, ↓albumin in uremia, ↑ free drug, more free un-ionised drug in acidosis
Metabolism unchanged ,↓ excretion,
Used in ↓ dose
Propofol Metabolised by liver No adverse effect
Etomidate Metabolised by liver, partial renal excretion
No adverse effect
Benzodiazepines Metabolised in liver & excreted by kidney, longer acting BZD accumulate, ↑duration of action
↑ Interval or ↓ dose
Neuromuscular blocking and reversal agentsWhen selecting a neuromuscular blocking agent(NMBA) for use in patients with CKD, we must consider :
• The impact of renal impairment on the elimination of the drug,
• The potential for drug accumulation with incremental doses, and
• The production of active metabolites.
Other factors include :
• The effect of acidaemia and
• Drug interactions on the intensity and duration of block.
In general, the initial dose required to produce neuromuscular block is larger in patients with CKD than in normal subjects. But, with the exception of atracurium and cisatracurium, the dose required to maintain block is reduced.
To prevent postoperative residual curarization (PORC), the anaesthetist should avoid using long-acting NMBA, or agents which are excreted in part in the urine, and make routine use of neuromuscular monitoring
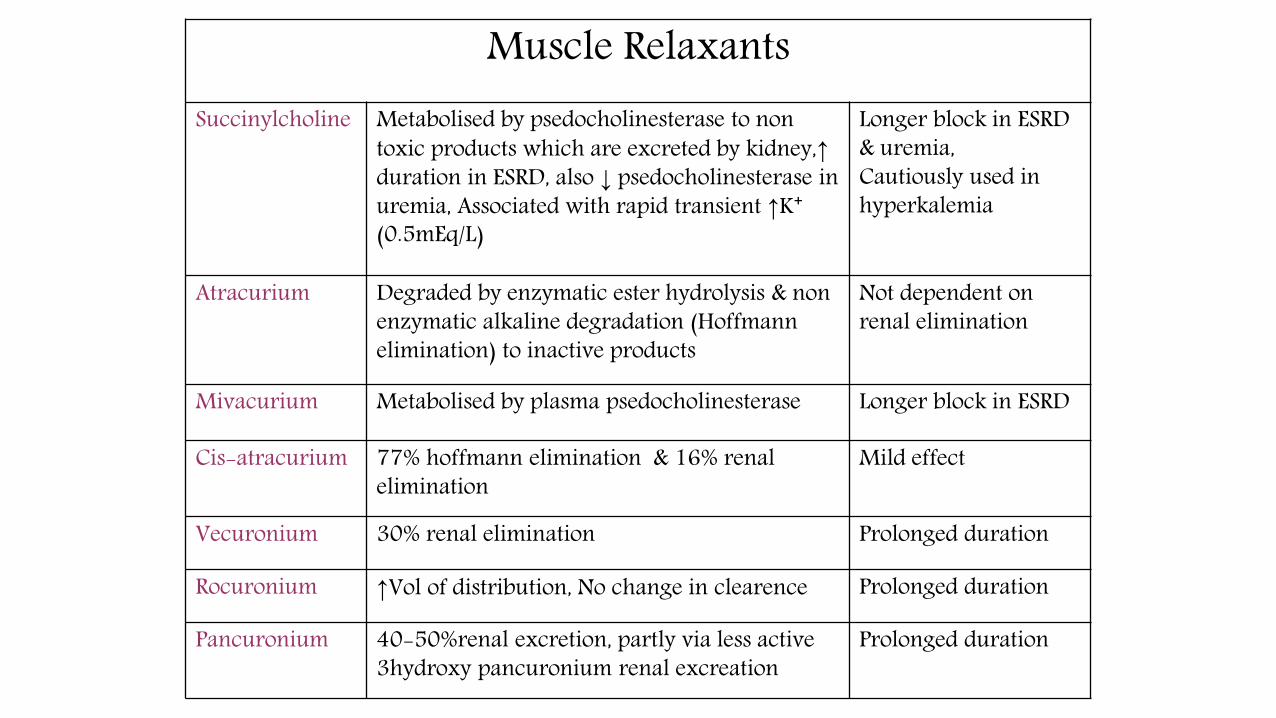
Muscle RelaxantsSuccinylcholine Metabolised by psedocholinesterase to non
toxic products which are excreted by kidney,↑duration in ESRD, also ↓ psedocholinesterase in uremia, Associated with rapid transient ↑K⁺(0.5mEq/L)
Longer block in ESRD & uremia,Cautiously used in hyperkalemia
Atracurium Degraded by enzymatic ester hydrolysis & non enzymatic alkaline degradation (Hoffmann elimination) to inactive products
Not dependent on renal elimination
Mivacurium Metabolised by plasma psedocholinesterase Longer block in ESRD
Cis-atracurium 77% hoffmann elimination & 16% renal elimination
Mild effect
Vecuronium 30% renal elimination Prolonged duration
Rocuronium ↑Vol of distribution, No change in clearence Prolonged duration
Pancuronium 40-50%renal excretion, partly via less active 3hydroxy pancuronium renal excreation
Prolonged duration
Neostigmine clearance is reduced and its half-life is prolonged in CKD. This may result in a parasympathomimetic response, including bradycardia and AV block, especially when used in combination with atropine rather than the longer-acting glycopyrronium.
Sugammadex is helpful in preventing PORC . It has got fewer side effects.
Analgesic agents
In administering analgesic agents, the anaesthetist needs to consider: • The impact of renal impairment on the distribution and elimination of
the parent compound and hence the need for adjusting the dose or dose interval;
• The formation of active metabolites; And the risk of compromising residual renal function.
Analgesic nephropathy is mainly associated with prolonged use of compound analgesics containing two antipyretic agents with caffeine or codeine.
• Acetaminophen oral acetaminophen 40 mg/kg/day for 3 days in normal subjects and patients with CKD produced no demonstrable change in glomerular or tubular function in either group. Prolonged use of acetaminophen is associated with analgesic nephropathy, but occasional or moderate use is safe and does not require dose adjustment even in perioperative period.
• Non-steroidal anti-inflammatory agents :They exacerbate hypertension and precipitate oedema, hyponatraemia, and hyperkalaemia. There is an increased risk of GI bleeding, cardiovascular complications in this at risk population. They precipitate an acute decrease in GFR and may also cause acute interstitial nephritis .
• The renal effects of the COX-2 inhibitors (rofecoxib) are similar to those of the non-selective NSAIDs and hence outweigh any potential benefit in perioperative period.
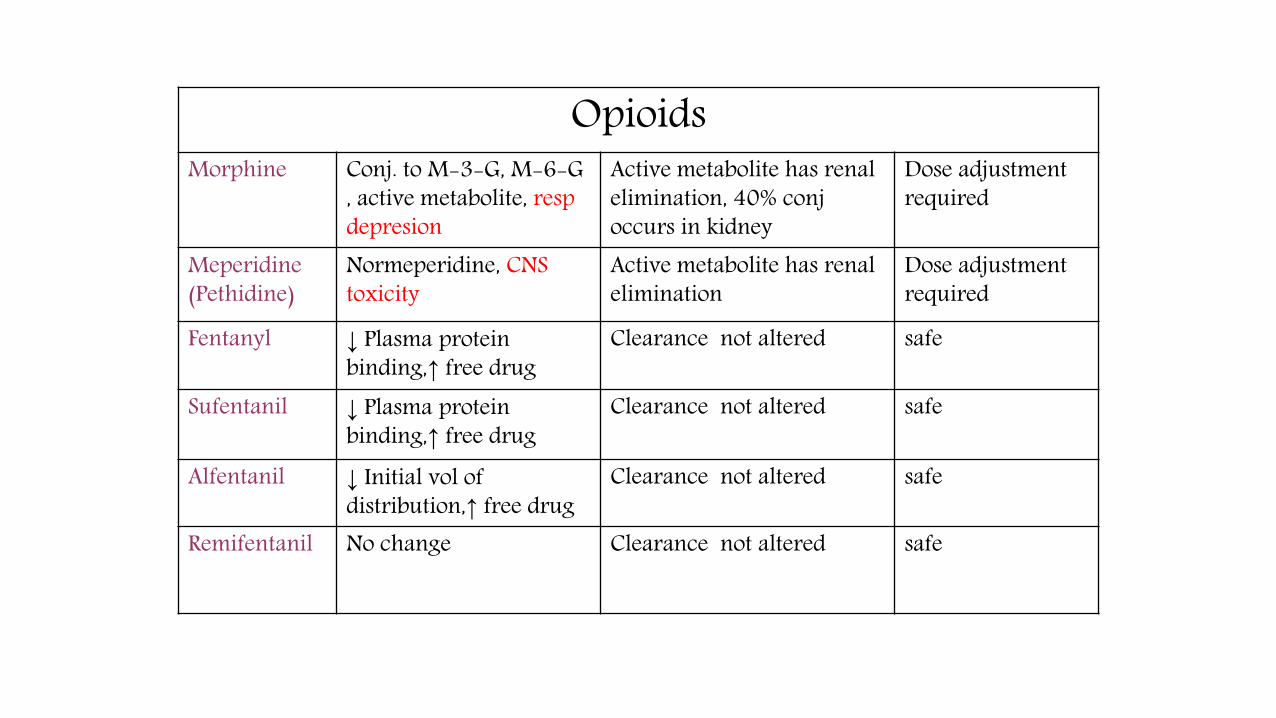
OpioidsOpioids have no direct toxic effects on the kidney. They do, however, have an antidiuretic effect, and they may cause urinary retention. Very rarely, their use has resulted in rhabdomyolysis.
Morphine is metabolized in the liver to Morphine-3-glucuronide, the major one, accounting for 70% of the dose. M3G antagonizes the analgesic effect of morphine, and is associated with irritability and a lower seizure threshold.Approx. 5% of a dose of morphine is metabolized to morphine-6-glucuronide (M6G), which has potent analgesic properties and may result in delayed onset of sedation and respiratory depression. The elimination of M6G is dependent on renal function, and in patients with renal failure, its half-life is prolonged from 2 to 27 h. The metabolite load from an equi-analgesic dose of morphine given by the oral route is greater than that from the parenteral route, due to extensive first-pass metabolism.In renal patients, the dose of morphine should be reduced and the patient carefully monitored for
signs of delayed onset respiratory
Fentanyl undergoes extensive hepatic metabolism with no active metabolites. Approximately 7% is excreted unchanged in the urine. Clearance is reduced in CKD.
Remifentanil is not dependent on renal function for elimination. It undergoes ester hydrolysis and its main metabolite is minimally active . In patients on HD, remifentanil had a reduced clearance and prolonged elimination halflife. A lower infusion rate is required, but recovery is not significantly prolonged.
Tramadol: 30 % of tramadol is excreted unchanged in the urine. O-Demethyl tramadol is an active metabolite which is excreted by the kidneys. Uraemia is associated with a lowered seizure threshold, and tramadol may be epileptogenic in these circumstances.
Meperidine is metabolized to normeperidine which is dependent on renal function for elimination. The use of meperidine in patients with CKD has been associated with seizures, myoclonus, and altered mental state.
Codeine and dihydrocodeine are also best avoided as their elimination half-life is significantly prolonged, and conventional doses have resulted in central nervous system depression.
OpioidsMorphine Conj. to M-3-G, M-6-G
, active metabolite, respdepresion
Active metabolite has renal elimination, 40% conj occurs in kidney
Dose adjustment required
Meperidine(Pethidine)
Normeperidine, CNS toxicity
Active metabolite has renal elimination
Dose adjustment required
Fentanyl ↓ Plasma protein binding,↑ free drug
Clearance not altered safe
Sufentanil ↓ Plasma protein binding,↑ free drug
Clearance not altered safe
Alfentanil ↓ Initial vol of distribution,↑ free drug
Clearance not altered safe
Remifentanil No change Clearance not altered safe
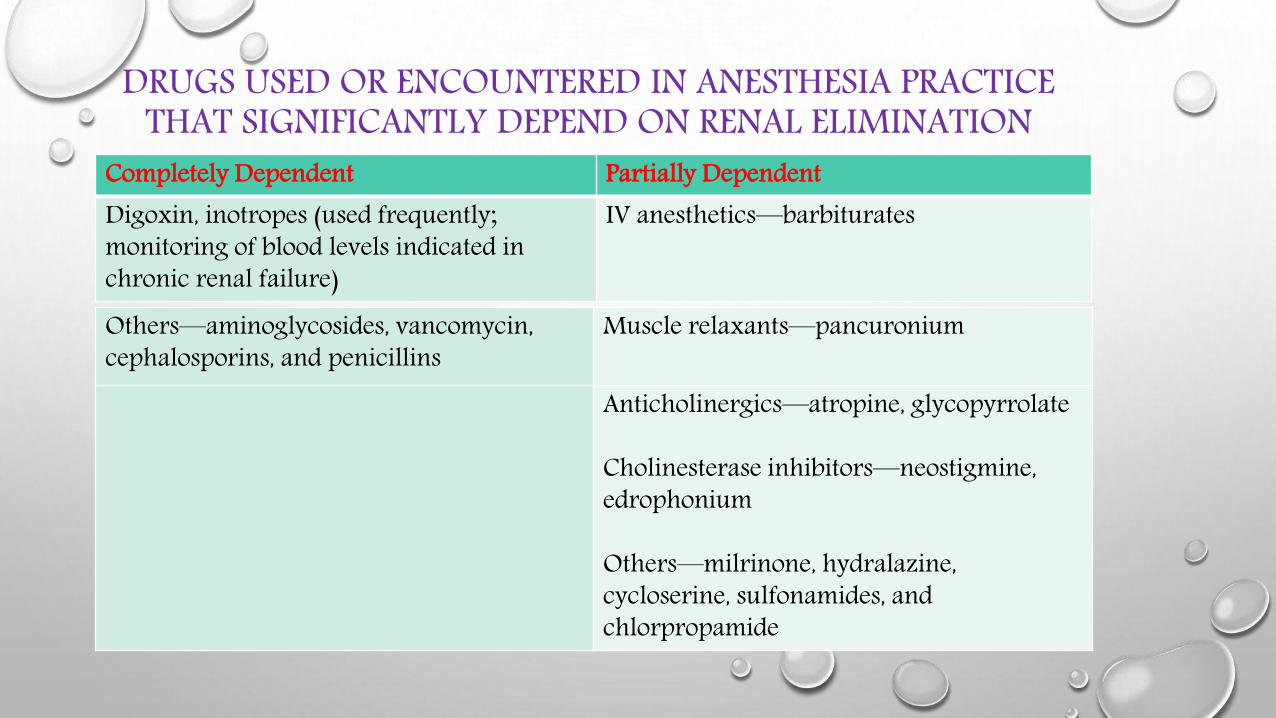
DRUGS USED OR ENCOUNTERED IN ANESTHESIA PRACTICE THAT SIGNIFICANTLY DEPEND ON RENAL ELIMINATION
Completely Dependent Partially DependentDigoxin, inotropes (used frequently; monitoring of blood levels indicated inchronic renal failure)
IV anesthetics—barbiturates
Others—aminoglycosides, vancomycin,cephalosporins, and penicillins
Muscle relaxants—pancuronium
Anticholinergics—atropine, glycopyrrolate
Cholinesterase inhibitors—neostigmine,edrophonium
Others—milrinone, hydralazine,cycloserine, sulfonamides, andchlorpropamide
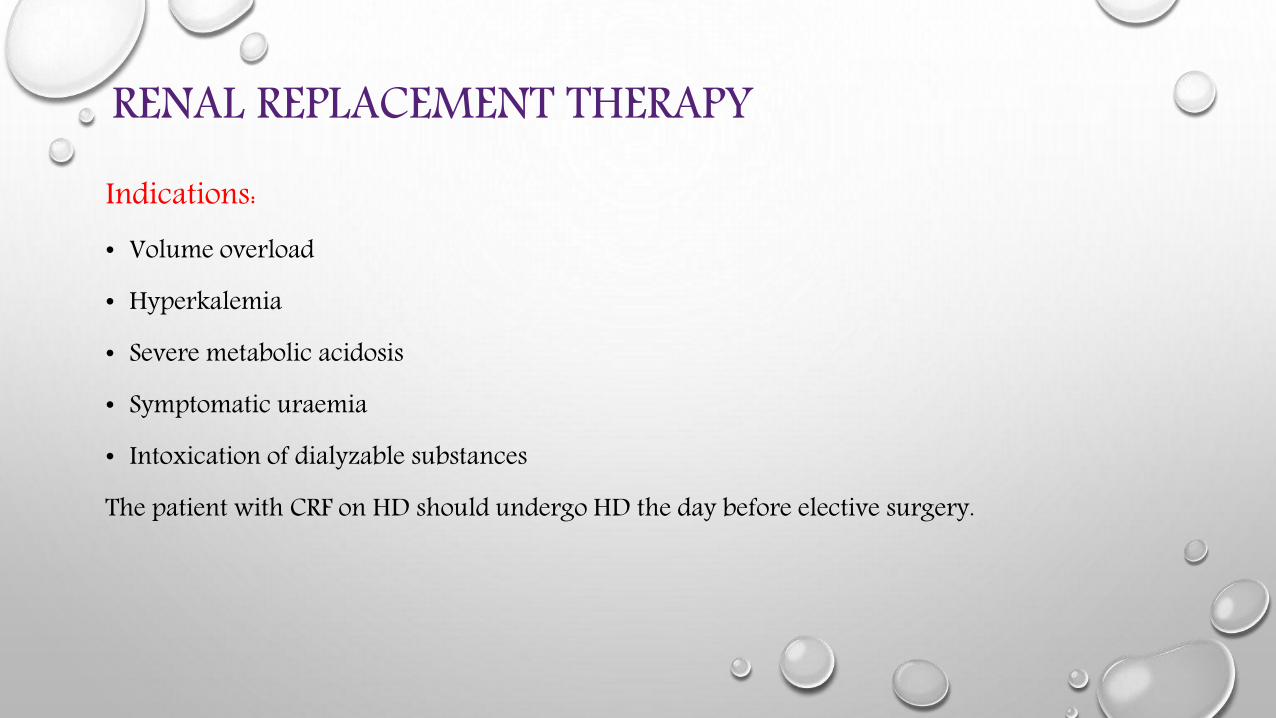
RENAL REPLACEMENT THERAPYIndications:• Volume overload
• Hyperkalemia
• Severe metabolic acidosis
• Symptomatic uraemia
• Intoxication of dialyzable substances
The patient with CRF on HD should undergo HD the day before elective surgery.
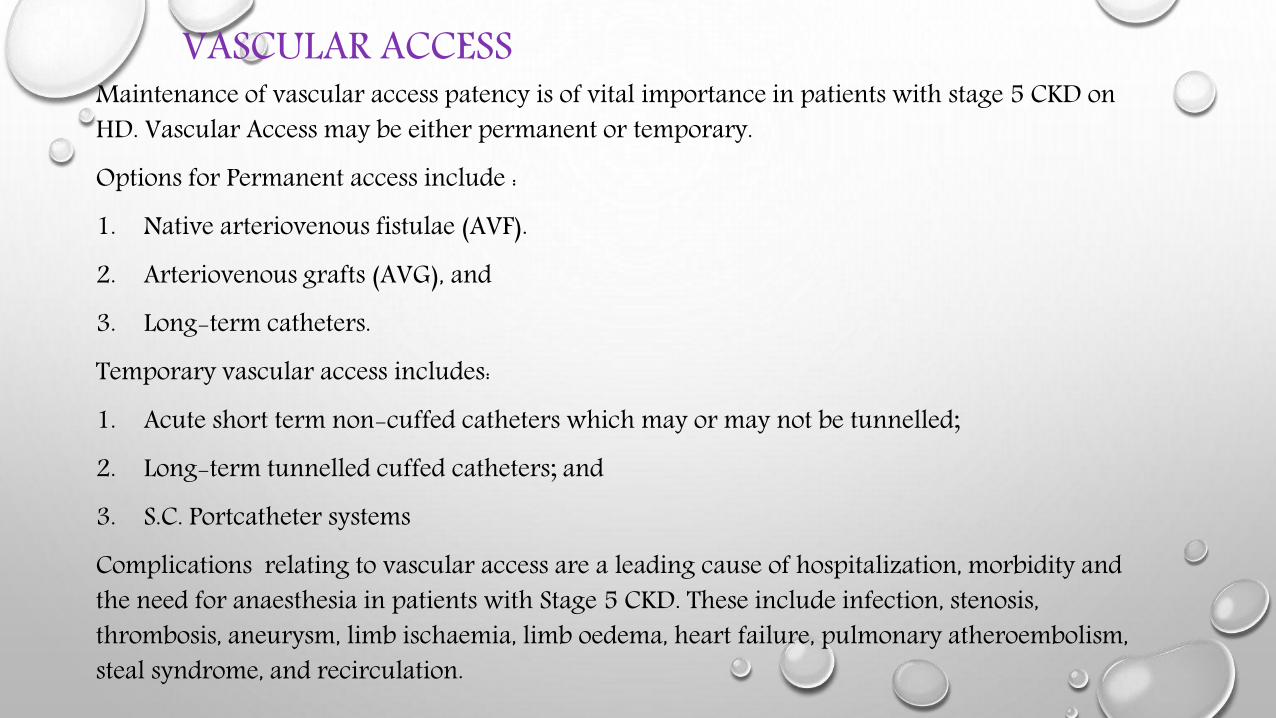
VASCULAR ACCESSMaintenance of vascular access patency is of vital importance in patients with stage 5 CKD on HD. Vascular Access may be either permanent or temporary. Options for Permanent access include :1. Native arteriovenous fistulae (AVF). 2. Arteriovenous grafts (AVG), and 3. Long-term catheters. Temporary vascular access includes: 1. Acute short term non-cuffed catheters which may or may not be tunnelled;2. Long-term tunnelled cuffed catheters; and 3. S.C. Portcatheter systemsComplications relating to vascular access are a leading cause of hospitalization, morbidity and the need for anaesthesia in patients with Stage 5 CKD. These include infection, stenosis, thrombosis, aneurysm, limb ischaemia, limb oedema, heart failure, pulmonary atheroembolism, steal syndrome, and recirculation.
PERIOPERATIVE FLUID MANAGEMENT• Non invasive operations require replacement of only sensible water losses with
5% glucose in water ( 5-10 ml/kg iv). The small amount of urine output can be replaced with 0.45% NaCl.
• Thoracic or abdominal surgeries can be associated with loss of significant intravascular fluid vo;ume to the interstitial spaces. This loss is often replaced with balanced salt solutions or 5% albumin .
• Blood transfusions must be considered when O2 carrying capacity is to be increased or if blood loss is excessive.
• Measuring CVP may be useful in guiding fluid replacement.
INTRAOPERATIVE MANAGEMENT GOALS• Appropriate intravascular volume replacement• Avoidance of nephrotoxic drugs• Urinary catheter aiming for a urine output of >0.5ml/kg/hr• Maintenance of a suitable intraop MAP• Monitoring CVP• Anticipation of anaesthetic and surgically induced hemodynamic pertubations
CHOICE OF ANAESTHESIA
• Regional anesthesia : Neuraxial anesthesia may be considered in patients with CKD. A sympathetic blockade of T4 to T10 levels may theoretically improve renal perfusion by attenuating catecholamine induced renal vasoconstriction and suppressing the surgical stress response. However, platelet dysfunction and the effects of residual heparin in patients receiving hemodialysis must also be considered. In addition, adequate intravascular fluid volume must be maintained to minimize hypotension.
• Brachial plexus blockade is useful for placing the vascular shunts necessary for long-term hemodialysis. In addition to providing analgesia, this form of regional anesthesia abolishes vasospasm and produces vasodilation that facilitates the surgical procedure.
• The presence of uremic neuropathies should be excluded before induction of regional anesthesia. Co-existing metabolic acidosis may decrease the threshold for seizures in response to local anesthetics.
Pre-Medication• Reduced doses of an opioid or BZD,
• H2 blocker - Aspiration prophylaxis,
• Metoclopramide -10 mg for accelerating gastric emptying, prevent vomiting, ↓risk of aspiration,
• Antihypertensive agents should be continued until the time of surgery.
Monitoring• All routine monitoring – ECG, NIBP, SpO₂, EtCO₂, NM monitoring
• Monitoring urinary output and intravascular volume (desirable urinary output: 0.5 ml/kg/hr)
• Intra-arterial, central venous, pulmonary artery monitoring are often indicated
• Intra-arterial blood pressure monitoring in poorly controlled hypertensive patients
ASSOCIATED CONCERNS
• Attention to patient positioning on the operating room table is important. Poor nutritional status renders the skin particularly prone to bruising and sloughing, and extra padding is required to protect vulnerable nerves around the elbows, knees, and ankles.
• Fistulas must be protected at all costs and be well padded to prevent pressure injury. Blood pressure cuffs should not be applied to the arm with the fistula. If at all possible, the arm with the fistula should not be tucked but should be positioned so that the fistula thrill can be checked periodically throughout surgery.
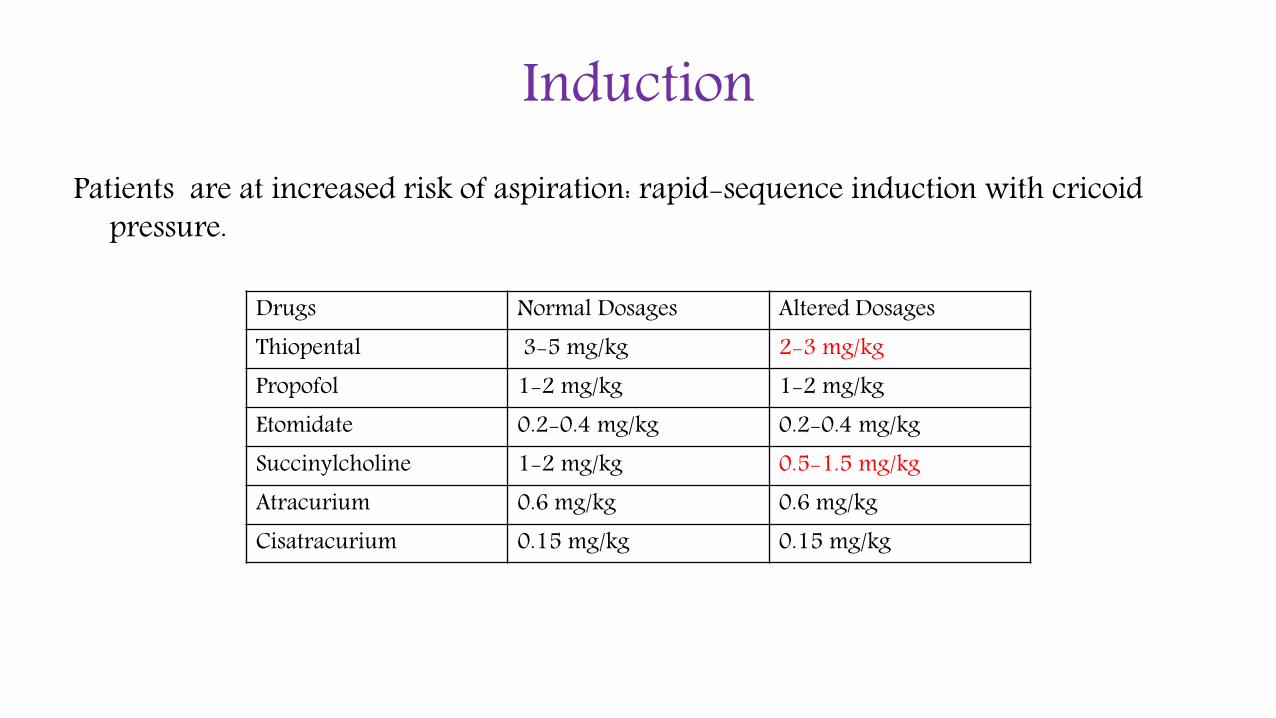
InductionPatients are at increased risk of aspiration: rapid-sequence induction with cricoid
pressure.
Drugs Normal Dosages Altered DosagesThiopental 3-5 mg/kg 2-3 mg/kgPropofol 1-2 mg/kg 1-2 mg/kgEtomidate 0.2-0.4 mg/kg 0.2-0.4 mg/kgSuccinylcholine 1-2 mg/kg 0.5-1.5 mg/kgAtracurium 0.6 mg/kg 0.6 mg/kgCisatracurium 0.15 mg/kg 0.15 mg/kg
Maintenance• Ideal maintenance - control hypertension with minimal
effects on cardiac output,
• Controlled ventilation with cuffed endo-trachial tube should be considered for patients with renal failure,
• Fluid therapy: D5W, isotonic crystalloids, colloids, pRBC,
• Anaesthesia can be maintained with inhalation agents or propofol with muscle relaxants ↓NM monitoring.
Reversal• Neuro-muscular blockage is reversed with Neostigmine or
pyridostgmine in combination with anticholenergic.
• Neostigmine and pyridostgmine has 50% & 70% renal elimination respectively.
• Glycopyrolate has 80% renal excretion so should be used cautiously.
• Atropine undergoes 25% renal elimination and rest hepatic metabolism to form metabolite noratropine which has renal excretion.
• Extubation should be done after complete reversal of NM blockage.
POSTOPERATIVE MANAGEMENT• Admission to ICU may be suitable for patients with significant comorbidities and after major
surgeries• Post op cardiac assessment must be performed and continued for 3-5 days with daily ECGs and
screening of cardiac enzymes to detect and treat perioperative MI which most frequently occurs within 72 hrs and are often silent yet quite fatal.
• HD should be ideally delayed till the risk of fluid shifts and hemorrhage has fallen ( some suggest at least 24 hrs )
• Close attention to fluid electrolyte balance. CVP to be kept between 10-12 cm of H2O• Multimodal analgesia : PCM is safe and effective . Intraoperative LA infiltration is simplest and
easiest but often inadequate and with finite duration.• Medications for HTN, IHD etc should be re established to pre operative normalcy as soon as possible. • For abdominal surgery patients placing feeding tubes facilitate drug administration even in presence
of reduced gastric emptying
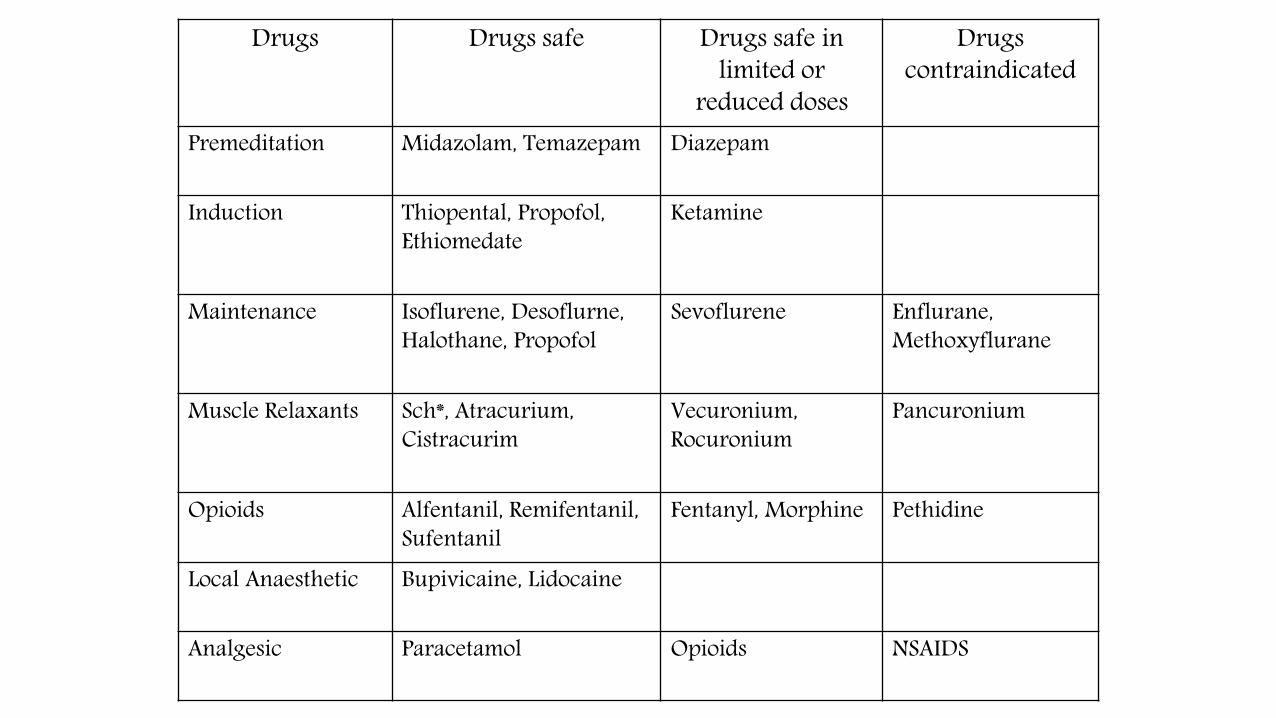
Drugs Drugs safe Drugs safe inlimited or
reduced doses
Drugs contraindicated
Premeditation Midazolam, Temazepam Diazepam
Induction Thiopental, Propofol, Ethiomedate
Ketamine
Maintenance Isoflurene, Desoflurne, Halothane, Propofol
Sevoflurene Enflurane, Methoxyflurane
Muscle Relaxants Sch*, Atracurium, Cistracurim
Vecuronium, Rocuronium
Pancuronium
Opioids Alfentanil, Remifentanil, Sufentanil
Fentanyl, Morphine Pethidine
Local Anaesthetic Bupivicaine, Lidocaine
Analgesic Paracetamol Opioids NSAIDS

.
1 MET to 4 METs >4METs Over 10 METs
Can take care of him/herself?
Climb a flight of stairs? Swim or run fast?
Get dressed on his/her own?
Walk 100 blocks? Plays a basketball game, run long distances at 10 km/h, row or participate in competition sport?
Walk at home on level ground?
Plays tennis doubles?
Climbs two steps? Does heavy household chores: moves heavyfurniture?
Do household chores: sweep the floors or washdishes?