Embed Size (px)
Citation preview
Anemia In PregnancyNzyoki Mulovi

Introduction
• Anaemia in pregnancy is defined as an Hb <11g/dl in the first and last trimester and less than 10.5g/dl in the second trimester.
• Commonest medical disorder in pregnancy• 30-50% of women become anemic during pregnancy, with
iron deficiency being the most common form of anemia accounting for more than 90% of the cases.
Hemoglobin Level
1st trimester < 11g/dl
2nd trimester <10.5g/dl
3rd trimester < 11g/dl
Causes • Increased blood loss
– acute – APH, PPH– Chronic- hookworm infestation, PUD, menorrhagia
• Nutritional– Low intake- vegans, socio-ecomonic factors– Reduced absorption- malabsorption syndrome, dairy products
• Reduced formation– Aplastic anemia– Medication – zidovudine, cancer chemo
• Increased destruction (hemolytic anemia)– Hereditary – hemoglobinopathies, membranopathies, enzymopathies– Acquired – immune (AIHA), non immune (paroxysmal nocturnal
hemoglobinuria)– Mechanical damage- malaria, HIV

Physiologic changes in pregnancy
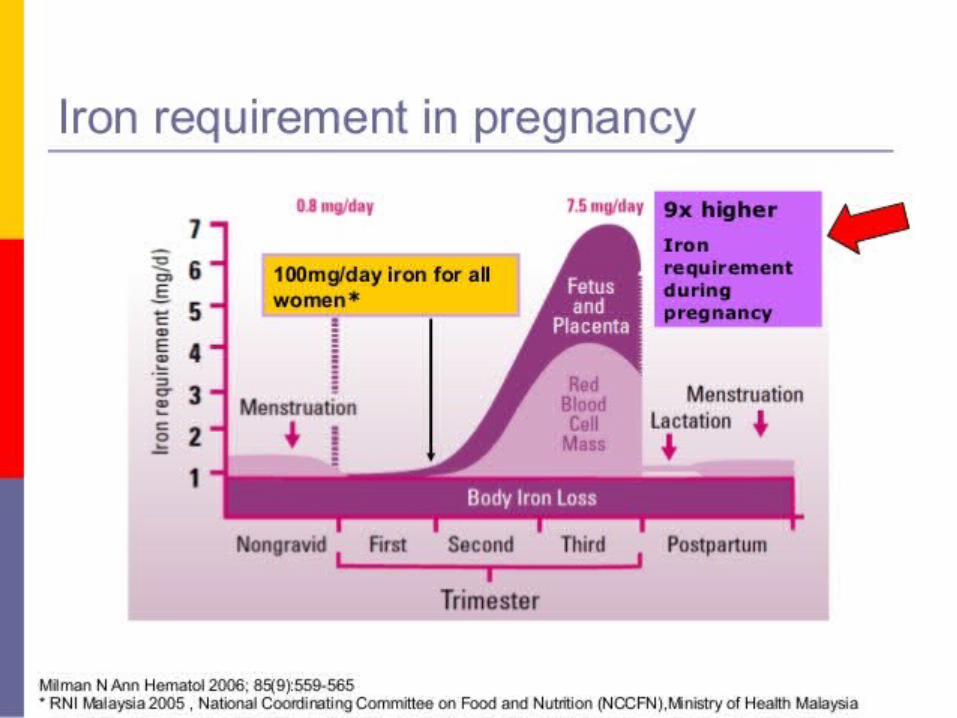
• During pregnancy there is an increase in total blood volume by 30-40%. The increase in plasma volume is usually higher than the HB level increase resulting in dilution.
• Iron requirements increase rapidly in the second (4-5mg/day)and third trimester(>6mg/day) due to fetal growth, however iron absorption in the gut is not sufficient to meet this increased demand. Thus iron balance depends on maternal iron stores during this period.

Impact of anemiaMaternal Fetal
Fatigue, Low birth weight
Increased risk of PPH Small for gestational age
Increased risk of sepsis Increased risk of peri-natal morbidity and mortality
Risk of CCF Increased incidence of diabetes and cardiac disease later in life
Increased risk of preterm labor Increased risk of preterm delivery
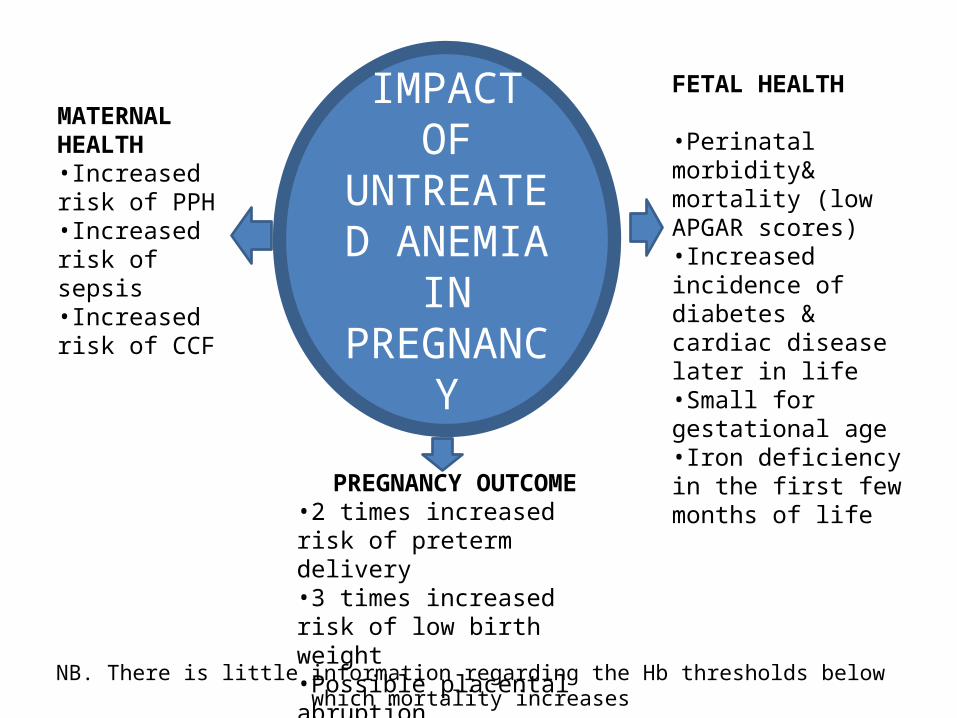
IMPACT OF UNTREATED ANEMIA IN
PREGNANCY
FETAL HEALTH
•Perinatal morbidity& mortality (low APGAR scores)•Increased incidence of diabetes & cardiac disease later in life•Small for gestational age•Iron deficiency in the first few months of life
MATERNAL HEALTH•Increased risk of PPH•Increased risk of sepsis•Increased risk of CCF
PREGNANCY OUTCOME•2 times increased risk of preterm delivery•3 times increased risk of low birth weight•Possible placental abruption
NB. There is little information regarding the Hb thresholds below which mortality increases
Epidemiology
• Iron deficiency is the most common form of malnutrition in the world, affecting more than 2 billion people globally i.e. 1/3 of the world’s population. (source WHO)
• Anemia in pregnancy is highly prevalent in less-developed countries (40-75%) compared to 18-20% in developed countries. (source RCOG)
• Responsible for 40% of maternal mortality in the 3rd world
35-56% 37-75 %37-52%

Risk factorsPregnancy Postpartum
Multiple pregnancy Iron deficiency during pregnancy
Low socio-economic status Delivery by CS
Multiparity Placenta previa
Short period between pregnancies Assisted vaginal delivery
Dietary factors PPH
Pre-pregnancy BMI
Other risk factors:•Malaria•HIV/ AIDS

DIAGNOSTIC WORKUP
Detailed History– Dietary Hx– Obs/Gyn Hx– Drug Hx– Social Hx– Duration of symptoms if any
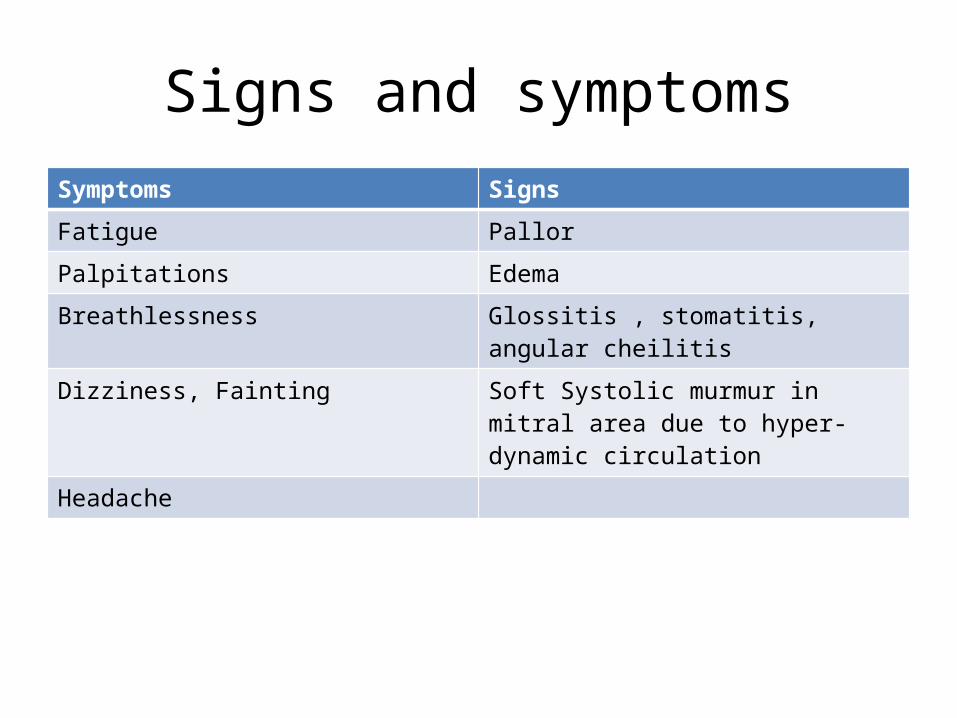
Signs and symptomsSymptoms Signs
Fatigue Pallor
Palpitations Edema
Breathlessness Glossitis , stomatitis, angular cheilitis
Dizziness, Fainting Soft Systolic murmur in mitral area due to hyper-dynamic circulation
Headache
Investigations
• Full blood count– Hemoglobin levels– PCV – Red cell Indices- MCV, MCHC, MCH
(routinely done as part of antenatal profile. NICE recommends Hemogram at booking and at 28wks gestation)
• Peripheral blood film- allows characteristics of the RBC to be observed. Hypochromic microcytic cells may be seen. Abnormal RBC morphology will also be seen.
Other investigations• Serum Ferritin
– Serum ferritin is a stable glycoprotein which accurately reflects iron stores in the absence of inflammatory change. It is the first laboratory test to become abnormal as iron stores decrease and it is not affected by recent iron ingestion.
– It is generally considered the best test to assess iron-deficiency in pregnancy, although it is an acute phase reactant and levels will rise when there is active infection or inflammation.
– Serum ferritin should be checked prior to starting iron in patients with known haemoglobinopathy.
• Serum Iron and Total Iron Binding Capacity (TIBC)- lack sensitivity and specificity due to diurnal variations and recent ingestion of iron.
Investigations cont.
• Stool for Ova & Cysts • Stool for occult blood• Bone marrow – considered the gold standard
for assessment of iron stores. Is however invasive and impractical unless cause of anemia can’t be identified by simpler means.
Trial of Iron Therapy
• Is both diagnostic and therapeutic.• It should be considered as the first line
diagnostic test for normocytic or microcytic anaemia. An increase in Hb must be demonstrated at 2 weeks, otherwise further tests are needed.
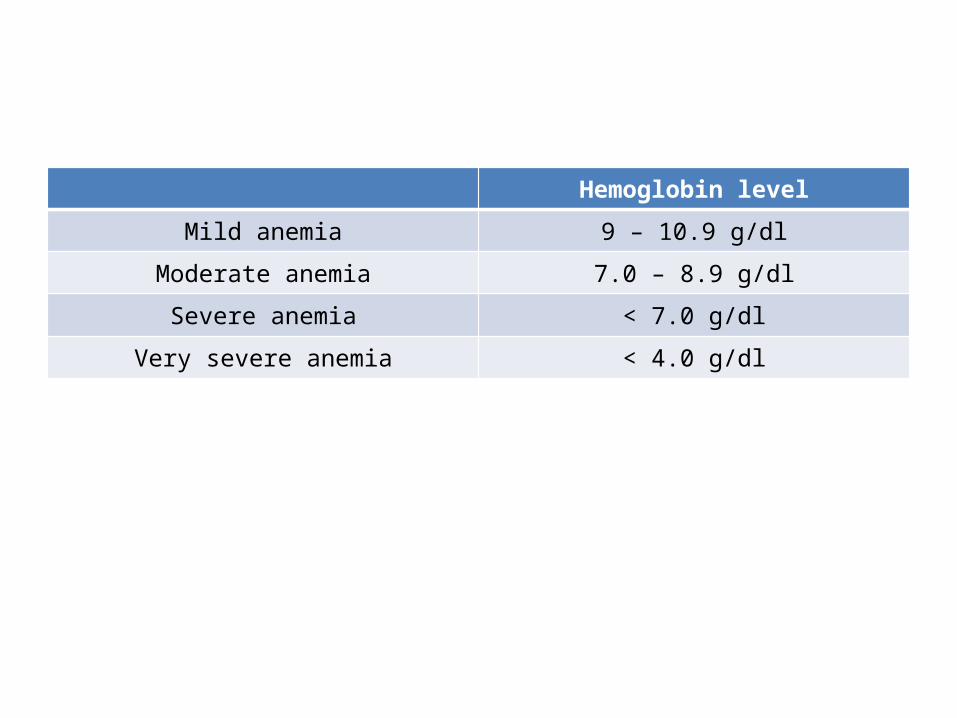
Hemoglobin level
Mild anemia 9 – 10.9 g/dl
Moderate anemia 7.0 – 8.9 g/dl
Severe anemia < 7.0 g/dl
Very severe anemia < 4.0 g/dl
Management of Iron Deficiency Anemia

DIETARY MANAGEMENT
• The amount of iron absorption depends upon the amount of iron in the diet, its bioavailability and physiological requirements.
• Haem iron is only found in meat, chicken and fish, and is easily absorbed.
• Non-haem iron is also found in plant foods, such as vegetables, cereals , beans and lentils, but is not absorbed as well by the body. Absorption may be enhanced by vitamin C. Germination and fermentation of cereals and legumes improve the bioavailability of non-haem iron by reducing the content of phytate.
• All women should be counseled regarding diet in pregnancy including details of iron rich food sources and factors that may inhibit or promote iron absorption and why maintaining adequate iron stores in pregnancy is important.
Oral Iron Supplementation
• Once women become iron deficient in pregnancy it is not possible to ensure repletion through diet alone and oral supplementation is needed.
• Ferrous iron salts are the preparation of choice. The oral dose for iron deficiency anemia should be 100-200mg of elemental iron daily.
• Available ferrous salts include ferrous fumarate, ferrous sulphate and ferrous gluconate
How to take Iron Supplements
• Women should be counseled as to how to take oral iron supplements correctly.
• This should be on an empty stomach, 1 hour before meals, with a source of vitamin C (ascorbic acid) such as orange juice to maximize absorption. Other medications or antacids should not be taken at the same time.
Indications for Iron supplementation
• Women with a Hb <11.0 g/dl in the 1st trimester or < 10.5g/dl thereafter should be offered trial of iron therapy unless they are known to have a hemoglobinopathy.
• In the presence of known haemoglobinopathy, serum ferritin should be checked and women offered therapeutic iron replacement if the ferritin is <30 µg/l.
• Secondary care should be considered if:– Anemia is severe (<7g/dl)– Significant symptoms– Advanced gestation (>34 weeks)
Response to oral Iron therapy
• The hemoglobin concentration should rise by 2 g/dl after 3–4 weeks. Failure to do so is usually due to poor compliance, misdiagnosis, continued blood loss, or malabsorption.
• Iron supplementation should be continued for three months after correction of anemia to replenish iron stores.
• For nausea and epigastric discomfort, preparations with lower iron content should be tried. Slow release and enteric coated forms should be avoided.

Parenteral Iron Therapy
Parenteral Iron Therapy• Parenteral iron should be considered from the
2nd trimester onwards and postpartum period in women with iron deficiency anemia who fail to respond to or are intolerant of oral iron.
• Associated with faster increases in Hb and better replenishment of iron stores in comparison with oral therapy.
• Fewer post partum transfusions have been reported in those treated with IV iron.
Parenteral Iron preparations
• Iron III carboxymaltose• iron sucrose e.g venofer• Iron dextran
Dose calculation
• Several formulas exist. The commonest is Nakao’s formula.
Iron needed(mg)=
(target HB-current HB)X
Body weightX
2.4

Precautions to take with Parenteral Iron Therapy
• Administer in a facility with capacity to handle any severe anaphylactic or allergic reaction.
• Start oral iron only after 5 days after the last injection of parenteral iron.
• Only use in proven cases of iron deficiency anemia.
• Shouldn’t be administered more than 3 times per week.
Contraindications to parenteral Iron Therapy
• History of anaphylaxis or reactions to parenteral iron therapy
• First trimester of pregnancy• Active acute or chronic infection• Chronic liver disease
BLOOD TRANSFUSION
Indications for Transfusion during pregnancy
• HB <7g/dl• HB <8g/dl & gestation >36 wks• Moderate or severe anemia in patient with
heart disease or severe resp. disease• Placenta previa with HB < 10g/dl• those who develop severe reactions to both
oral and parenteral iron.

Management of Anemic patient in labor
• If Hb is <8g/dl tranfuse• If Hb is <10 g/dl have blood available for
transfusion• Active management of 3rd stage of labor
(AMTSL)
Prevention
• Universal iron supplementation in pregnancy from the second trimester.
• Nutritional counseling on rich sources of iron.• Intermittent prophylactic therapy and
insecticide treated nets given in Malaria endemic zones. (SP given after 16 wks and 4 wks thereafter)
• Deworming with mebendazole 500mg stat in the 2nd trimester.


![Anaemia in Pregnancy - Welcome to JPAC...Anaemia during pregnancy is a global problem WHO region Prevalence of anaemia (%) in pregnant women [95% CI] Number of pregnant women affected](https://img.pdfslide.us/doc/110x75/5f048bb57e708231d40e80e4/anaemia-in-pregnancy-welcome-to-jpac-anaemia-during-pregnancy-is-a-global.jpg)







![Anaemia in Pregnancy: Prevalence, Risk Factors, and ......Anaemia during pregnancy is a public health problem especially in developing countries and is associated with adverseoutcomesinpregnancy[].WorldHealthOrgani-zation](https://img.pdfslide.us/doc/110x75/60df1f679f6a99520b461cd1/anaemia-in-pregnancy-prevalence-risk-factors-and-anaemia-during-pregnancy.jpg)