Embed Size (px)
Citation preview

NHSNHS Improvement
Transforming Inpatient Care Programme
An integrated approach:The transferability of the WinningPrinciples - Sharing the learning
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE


An integrated approach: The transferability of the Winning Principles - Sharing the learning | 3
ContentsForeword 4
Introduction 5
Transferring the Winning Principles through integrated working 6
Testing the transferability of the Winning Principles 8
Winning Principle 1 and 4 - Single point of access for cancer patients 9
Winning Principle 1 - How existing good practice in long term 14conditions can benefit lung cancer patients
Winning Principle 1 - A primary and secondary care clinical 18management pathway for all patients with acute urine retention
Winning Principle 4 - Self management programme 21for cancer patients and carers
Lessons from other integrated working communities 24
A practical service improvement framework to support 25integrated working
Challenges faced and overcome 26
Key learning - Patient and carer experience 27
Achieving integration - 12 recommendations 28
Conclusion 29
Appendices 30
Websites and useful reading 32
Acknowledgements 33
Further information 34

4 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Foreword
Every person affected by cancer should receive world class services at each stage of their cancerjourney. (The Cancer Reform Strategy, 2007).
A patients’ journey involves many stages, and they encounter a large range of staff from differentorganisations providing services to them. The provision of integrated services that provide care inthe right place, at the right time and through the right person or team is paramount.
An integrated approach – The transferability of the Winning Principles shares the learning andchallenges drawn from the experiences of the integrated working communities involved in thiswork. The integrated working communities involved a vast range of staff from Acute Care, PrimaryCare, Social Care and the third sector communities. All of whom aim to improve services for theirpatients, carers, service users and their families.
This improvement work is part of the Cancer Transforming Inpatient Care Programme and highlightsthat although ‘integrated community working’ can be challenging the opportunities and benefitsare great for patients and their families.
Dr Janet WilliamsonNational DirectorNHS Improvement

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 5
Introduction
NHS Improvement tested the transferabilityof the four quality driven WinningPrinciples (NHS Improvement 2008). Theaim was to explore if the spread of theprinciples could be accelerated throughtaking an ‘integrated’ working approach tosupport the drive to enhance health andsocial care integrated working.
The learning from this testing supports thenew governments ‘commitment to thecontinuous improvement of the quality ofservices to patients’ (The Coalition; Ourprogramme for the Government 2010)and continues to support the delivery of theCancer Reform Strategy, TransformingInpatient Care Programme (2007).

6 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Five integrated test communitiestook on the challenge to spread.
Winning PrinciplesWinning Principle 1Unscheduled (emergency) patients should be assessed prior to the decisionto admit. Emergency admission should be the exception not the norm.
Winning Principle 2All patients should be on defined inpatient pathways based on theirtumour type and reasons for admission.
Winning Principle 3Clinical decisions should be made on a daily basis to promote proactivecase management.
Winning Principle 4Patient and carers need to know about their condition and symptoms toencourage self-management and to know who to contact when needed.
www.improvement.nhs.uk/cancer/inpatients
Transferring the Winning Principles throughintegrated working
The learning from the integrated testsites demonstrated that the principlesare appropriate, relevant andtransferable across the health andsocial care setting.
There has been a decade ofpublications and policies that indicatethe benefits of health and social careintegrated working. However thecase studies in this publicationindicate this is not easy to achieve andinvolved significant challenges,learning , vast amounts of time andthey have had varying degrees ofsuccess and shown that integratedworking can be achieved, provided:
• Relationships are built• Agreements are reached andcommunicated, with services andsystems that are aligned
• Partnership working and decisionmaking is clearly understood, whatthis means and the values thatunderpin this
• Responsibility for the improvementof services is shared.

0 10 20 30 40
Staf
fd
isci
plin
es
50
GP Practice Managers
Training Co-ordinator
NHS Direct
PCT Commissioners
Clinical Governance Staff
Information and Data Analysis
Voluntary Organisation Staff
Benefits and Employment
Hospice Staff
Walk-in Centre Staff
Ambulance Call Handlers
End of Life Facilitators
Clinical Illustraion
Pharmacists
Service Improvement Staff
All Managers Across All Organisations
Therapists
Specialist Nurses/Hospitals/Community
Doctors/Consultants/GPs
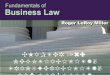
Number of staff involved
Figure 1: Discipline of staff involved in integrated working
An integrated approach: The transferability of the Winning Principles - Sharing the learning | 7
The case studies, share the learning fromfive ‘integrated’ working communities,involving acute care, primary care, socialcare, and tertiary services. Over 360people, including patients, carer's andstaff were involved (Figure 1).
‘There are many powerful examples of ways to improvequality in the NHS while encouraging better productivity.Together, we need to identify these examples ofexcellence, understand why this kind of approach issuccessful and actively diffuse this good practice acrossthe whole health service’
Jim EastonNHS National Director for Improvement and Efficiency

8 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Testing the transferability of theWinning Principles
The integrated working communitiestested the transferability of the qualityWinning Principles, 1 and 4.
The following case studies share theintegrated working communitieslearning and experiences.

Integrated testing model: Single pointof access for cancer patients
BackgroundTrusts local baseline data (2008) on allcancer related admissions showedthat approximately 70% of cancerinpatient admissions were nonelective. Average length of stay forthese patients was 6.5 days (April –Dec 2009) and the majority of theseadmissions came via A&E (Figure 2).
The most common reasons foremergency admissions were:• Shortness of breath• Pain• Collapse• Diarrhoea, constipation,dehydration, nausea and vomiting
As a testing community we agreed totest the assumption that many of thepatients admitted as emergenciescould have been treated in alternativecare settings and admission intohospital could have been averted.Bringing care closer to home andvaluing patients time.
120
100
80
60
40
20
0Accident
& EmergencyEmergencyOutpatient
EmergencyGP
OtherImmediate
Nu
mb
ero
fp
atie
nts
Referral type
Figure 2: Emergency referrals by type
Figure 3: Integrated working community
Sherwood Forest Hospitals NHS Foundation Trust
GP Practices
East Midlands Cancer Network
CNCS
Social Services
MacMillan
Patients and carers
Notts County Teaching PCT
NHS Direct
EMAS
Nottinghamshire Health Informatics Service
Source: SFHFT Health Informatics Department
An integrated approach: The transferability of the Winning Principles - Sharing the learning | 9
Sherwood Forest Hospitals NHS Foundation Trust
Kirkby Walk in Centre
Nottingham University Hospital NHS Trust
Beaumond House Hospice
Crossroads
Lloyds Pharmacy
Local independent pharmacy
Crossroads
Department of Work and Pensions
Job Centre Plus
Nottinghamshire Community Health
John Eastwood Hospice
Integrated testing community -what was it?The testing community included22 organisations across thecommunity (Figure 3).
WinningPrinciple 1
WinningPrinciple 4

Key stakeholders from theorganisations were identified early onin the work to assist in buildingmomentum and planning for anintegrated cancer service.
Fact finding and visioning events wereheld during the first four months of2009 to establish areas ofcommonality, identify problems thatneeded to be investigated andhighlight where testing may beneeded.
Across the community the main‘issues’ indentified were:• Poor communication and integratedworking between health and socialcare
• Inappropriate and rigid systems ofdiagnostics and treatment withincare pathways
• Lack of patient empowerment withcare needs.
• Unclear management of emergencyadmissions
• Lack of a clear clinical pathway• Lack of development promotingpatient self management support.
What was tested?To address the issues identified it wasagreed to test a single point of access(SPA) communication model. Thissupported the testing of thetransferability of Winning Principles 1and 4 and built upon the concept ofRecurring Admission Patient Alerts(RAPA) that had been successfullyimplemented in the Trust.
The single point of access wassupported by patients and their carersas during the visioning events theystated that they:
‘Did not know whoto contact and howto access servicesafter the end of theworking day.’Patient carers statement
Included in the scope of testing wasthe out of hours provision (OOH) andthe measures of impact were:• Valuing patient time reducingunnecessary waits and delays
• % reduction of inappropriateadmissions to hospital
• % of appropriate care deliverednearer to home.
After considering several options themost appropriate provider for testingthe model of a single point of accesswere Central Nottinghamshire ClinicalServices (CNCS). They were able tooffer dedicated nurses to answer calls,and already had information sharingagreements with the trust and anunderstanding of primary andsecondary care. Therefore this was ause of resources already in placerather than new financial investment.
10 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
SPA arranges foradmission to
surgical & medicalassessment units.
NOT A&E
SPArefers tooncology
ward
SPArefersclinicalnurse
specialist
SPArefers towalk incentre
SPArefers to
socialservices
SPArefers to
crossroads forindependent
social care
No immediatecare requiredAdvice givenor signposted
SPArefers toGP for
assessmentand/or visit
Patient makes call toSingle Point of Access (SPA)
Automated call outcomesent via email to appropriate CNS
Figure 4: The Single Point of Access (SPA)

Central Nottinghamshire Clinical Services
Cancer Nurse Specialists
Both CNCS & CNS (separate occasions)
71%
5%
24%
An integrated approach: The transferability of the Winning Principles - Sharing the learning | 11
Testing ran for 12 weeks (October2009 – January 2010) and involved 82cancer patients from four tumoursites: Gynaecology, Breast, LowerGastro Intestinal (LGI) and Urology.
Calls were received by SPA callhandlers at CNCS, were dealt withand then an automated message sentdirectly to both an email account andthe smart-phones held by the clinicalnurse specialists (CNS), which linkedto the existing successful RAPAmethodology of automated alerts thisaided clear communication channelsto the relevant clinicians.
Of the 82 patients, 66 calls weremade:• 41% of the calls were made in theout of hour’s period (5pm – 9am), atimeframe which currently provideslittle support outside of emergencycare and can be confusing forpatients and carers to navigate
• 34% of calls resulted in a possibleor definite emergency avertedadmission
• 9% of all calls resulted in a primarycare intervention and averted a nonelective admission
• 4% of patients had an expeditedemergency admission, bypassingA&E and resulting in a shorter bedstay
• A further 5% of calls resulted in apossible averted admission, all casesbeing resolved in primary care.
The following tables and graphsprovide a detailed breakdown of theactivity involved.
In hours Out ofhours
Calls (total)
16
3
13
7
39
16
5
4
2
27
32
8
17
9
66
Breast
Lower GI
Urology
Gynaecology
Total
Figure 5: Amount of patients that called SPA (including multiple times)
Figure 6: Calls to SPA who answered in and out of hours
25
20
15
10
5
0Info
to keyworker
Am
ou
nt
999Emergency
DoctorsAdvice
Tested atPrimary
Care Centre
HomeVisit
NurseAdvice
DistrictNurse
Non CNCSCalls
(CNS &Tech Faults)
Outcome
22
1 1
56
1
7
1113
Figure 7: Distribution of calls by outcome
Tumour site

12 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Averting emergency admissionsand A&E attendances definitionsWhere we have confirmed that hadthe patient not contacted the SPA andthat 999 would have been called, wehave classified this as ‘averted’.Where we have not been able todirectly confirm whether anemergency admission was averted butthat it was indeed possible we haveclassified this as ‘possible’.
Benefits and impactPotential cost savings/capacityreleasingBased on local data from SherwoodForest Hospitals NHS Foundation Trusthealth informatics department(February 2010) from January 2010across the four tumour sites involvedin testing, there are approximately4,255 active cancer patients.
Averting eight A&E attendancesduring testing resulted in a saving of£640 (standard A&E tariff = £80).Adding the four possible averted A&Eattendances brings the total to £960.Based on eight definite A&E avertedattendances out of 82 test patients(9.75%) over a 12 month period thepotential cash flow release at astandard tariff for active cancerpatients in the test tumour sitesequates to approximately £33,200 ayear.
Averted non-electiveadmission
Possible avertednon-elective admission
Tumour site
5
0
2
1
8
4
0
0
0
4
Breast
Lower GI
Urology
Gynaecology
Total
Figure 8: Averted and possible averted non elective admissions
Cash flow release£ (A&E only basedstandard tariff of£80)
Potentialinpatient bed daycash flow release
Figure 9: Potential cost savings/capacity releasing
Potential bed days releasedacross four tumour groups(using average LOS of 6.5days & average tariff of £340)
Test (3 monthsand 82 patients)
£80 x 8 = £640 6.5 days x 8 patients =52 released bed days
52 bed days x£340 = £17,680
Valuing patients timeFor those patients that were admittedduring the test, the average LOS was1.5 days. This was five days less thanthe original average length of stay.This can potentially be attributed tousing the special patient notes andimproved communication set up forthe integrated testing work.
The benefits identified fromtesting the SPAQuality• Delivers care in the mostappropriate setting
• Reduces pathway delays – threepatients admitted straight to wardmissing out A&E and EAU
• SPA standardises in hours and out ofhours care
• Special patient notes aid clinicaldecision making as does oncologicalemergencies training for callhandlers
• Patient safety, less exposure to riskof hospital acquired infection
• Improved communication modelmeaning call handlers cancommunicate directly with allintegrated areas.
Productivity• Reduction in length of stay from 6.5to 1.5 days for those patientsneeding a hospital admission
• Potentially released 52 bed days• Potential cash flow release of£17,680
Valuing patients’ time andexperience• Values patients’ time and addressespatient and stakeholdersexpectations
• Delivers care at home wherenecessary and where appropriate

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 13
• Enables patients to accessinformation and guidance allowingfor increased ability to self manage
• Reassurance of speaking to a personrather than being met by ananswering machine enhanced theirconfidence and assisted in reducinganxiety
• Reduction in numbers of delayedtransfers of care demonstrated bypatients going directly to the wardwhere appropriate.

14 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
How existing good practice in long termconditions can benefit lung cancer patients
BackgroundWorking in partnership NHS Coventry,University Hospitals Coventry andWarwickshire (UHCW) and CoventryCity Council, had developed anintegrated model of care – CareOutside of Hospital for Long TermConditions, (LTC).
The aim of the integrated testing wasto build on this existing infrastructureand test the transferability of the LTCmodel to improve services for lungcancer patients.
What was the issue for lungcancer patients?Coventry had the highest number ofemergency admissions for lung cancerpatients across the West MidlandsStrategic Health Authority (SHA), andof the patients admitted 50% diedwithin seven days, suggesting thatthey were in the end of life phase oftheir illness.
NHS Coventry
Testing approach: Gettingbaseline information for betterdecisionsA systematic service improvementapproach was used for testing, thisincluded a baseline analysis, and aretrospective notes review on theinitial lung cancer patient cohort.Many of these patients were deceasedand notes were held off the hospitalsite. Although a well establishedapproach, the process of undertakingthis initial review proved difficult andaffected the momentum andengagement across the integratedworking community.
Emergencyadmissions(Lung)
140
Figure 10: Hospital Episodes statistics Data
Ended in deathon day ofadmission
12%
Ended indeath byday one
24%
Ended indeath byday five
45%
Ended indeath byday seven
50%
Replicatedprocess as per
PCT map
Room identifiedwhere notes
review needs totake place
Safe guardian ofnotes niminated -Director of Nursing& Medical Director
Head of Inforequested toorder patient
notes (9 Feb 2009)
Notes againrequested
(16 Feb 2009)
Head of Info:delegated notes
retrieval
Head of Info:liaise with PCT
to order
Notes to beavailable byend of week
Acute TrustExecutive
interventionrequired
Figure 11: The Acute process
WinningPrinciple 1
Collating baseline informationfor better decisionsThe learning from this process and thereality of the experience is shared infigures 11 and 12 and shows theAcute and PCT process.

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 15
HES dataobtained
(Nov 2008)
Caldicottapproval
needed at PCT
Patient identifiersrequested
from PCT datadepartment
Request sentto audit
department
Clarity requiredif this is ‘audit’
or ‘research’
Request sentback to service
redesign qualitydirector for clarity
PCT datadepartment
issue job no. 247
Caldicott Guardiansign off request
given(Jan 2009)
Paperwork notreceived in
relevantdepartment
Need torequest Caldicott
Guardian signoff again
All paperworkresent
PIDs identifiedfrom PCT Head of
Info (Feb 2009)
Caldicott Guardianapproval given
(Feb 2009)
No budgetavailable
within PCT
Agreement fromservice redesign quality
director to pay fornotes request
Sent to acutetrust to order
notes
Finance Process
Figure 12: The PCT process
Identifying the real problems,issues and areas for testingAlthough the notes review was apains taking experience they dididentify that a high proportion ofpatients were admitted from oneparticular post code area, CV2.
Patients from this area presented asemergencies with a number ofsymptoms, with the highest numberbeing shortness of breath and pain asthe main reasons for admission.
Figure 13: Main presenting symptoms
Presentingsymptom
Shortness of breath
Pain
Number ofpatients
42
23
Gaining Re-engagement across thecommunityA pathway event was held April 2009,to share the results of the baselineand to jointly determine across thecommunity new ways of working.
The event included staff membersfrom the acute and communityorganisations, West MidlandsAmbulance NHS Trust and staff fromCoventry City Council.
The pathway day was successful forcommunication and engagement andit was agreed that communicationand information would be the focusof testing. Two ideas were takenforward:• Single point of contact for lungcancer patients
• Community directory.

16 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Single point of contact for lungcancer patientsThis involved GP practices andcommunity service providers for thepostal code area of CV2.A key improvement was to gainaccess to the ‘special notes facility’available on Webaccess. Webaccess isa system that was already available foruse in all GP practices across Coventry.This was utilised to share informationregarding lung cancer patientsincluded in the test cohort. It was aresource already available andrequired no further investment.
Testing was due to commence inOctober 2009. However, technicaldifficulties delayed the start of thetesting until January 2010. This delayaffected the momentum andengagement in the work. The testingperiod was for six weeks and included14 GP practices in the CV2 postcodearea of Coventry, which at the timehad 13 patients between themregistered with a diagnosis of lungcancer.
During the testing period the specialnotes facility was accessed for 31% ofpatients, none of these patients wereadmitted to hospital suggesting thatthe enhanced communication andknowledge of the patient, i.e. accessto the ‘special notes facility’ may haveaverted the admission.
The testing of the Webaccess systemfor lung cancer patients demonstratedthat it can be utilised successfully, anddoes avert emergency admissions.

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 17
Community directory for staffA community directory was developedin partnership between primary andsecondary health care, social care andCoventry City Council to enhancecommunication. Notification of thiswas emailed to all staff and GPsinvolved in the test site.
It is available to all with access to theNHS Coventry website. The directoryprovides a comprehensive list ofservices, there is a brief explanation ofeach of these services with contactdetails and what patients and carerscan expect form the service.
Lessons learned and reflectionsThis improvement work was based onthe understanding that there was anexisting successful integrated model ofcare for long term conditions, andthat the relationships alreadydeveloped through this work wouldprovide a platform for testingintegrated working with cancerpatients. However this did not providethe basis for testing with cancerpatients as had been anticipated. Thequestion is why? The following areobservations and experiences fromsome of those involved that may helpothers when embarking on similarintegrated working.
• ’It has proven difficult to identify asense of a shared test initiative inspite of the involvement of differentorganisations and multi-disciplinarygroups of staff’
• ’There were many issues to beaddressed, but the ability togenerate ideas and innovations fortesting were not forthcomingeveryone seemed to think it wassomeone else’s problem’
• ’An improvement project like thisrelies on good baseline information,but the delays in getting thisinformation was not identified as arisk, but it had a significant impacton engagement’
• ’Leadership has proven difficult asoriginally this area of work wasinitiated by only one of theorganisations involved, with adedicated lead for the work,however when the individual movedjob roles there was no-oneidentified to take ‘ownership’ of theworkstream, it therefore lost itsmomentum’
• ’During the lifetime of the project,other events (swine flu, HPVdevelopment) took over the time,resources and the key playersavailable’
• ’There was no strategic pressures onany of the organisations to fulfill thisproject’s potential’.
This work fits with many nationalagenda’s, QIPP, Care Closer to Home,Encouraging Improvements in MedicalCare and Decision Making. Integratedworking supports the message thatpatient care does involve the wholecommunity. A key lesson learned fromthis work is that an important successfactor is the organisations involvedhave the ability to relate to oneanother and have the capability andwillingness to partner and share.This small scale testing indicated thepotential, however to take thisforward and scale up the work,engagement of all the organisationsinvolved must be at the forefront.

18 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
A primary and secondary care clinical managementpathway for ALL patients with acute urinary retention
Starting positionA baseline data analysis on 122urology patients presenting to LincolnCounty Hospital revealed:• The average length of stay was fivedays with a maximum of 57 daysand minimum of 0 days.
• The largest referral source was 45% from GPs followed by:• 15% GP out of hours• 23% patient, self referral• 8% unknown• 4% via the nurse practitioner,• 2% other A&Es,• 2% via outpatient clinic• 1% via nursing home
• 113 (93%) of the 122 patients wereadmitted as emergencies andcatheterised as an in-patient
• These patients presented at threeentry points• A&E 42%• Emergency assessment unit 39%• Straight to wards 19%
The Lincolnshire Experience
• 119 (98%) patients had urineretention, some with additionalsymptoms such as abdominal painor haematuria, and three patientswere admitted with a blockedcatheter.
A real time data collection confirmedthat a disparity in pathways existed forpatients with acute urinary retention.Using an integrated approach the aimwas to test Winning Principle 1 andnew ways of working for patientswith acute urinary retention thatwould benefit ALL patients with nocarving out for cancer patients.
An integrated task with anintegrated team.An integrated task and finish groupwas established, the membershipconsisted of GPs, consultant urologist,clinical nurse specialist from United
Lincolnshire Hospital NHS Trust, wardrepresentation, community nursingleads, incontinence lead from the PCTand director of provider services forthe PCT.
After review of the baseline data itappeared that a large number ofpatients were being inappropriatelyguided to acute hospital emergencydepartments. The group agreed toplan a clinical management pathwaywhich, if successful through testing,would be a benefit to a large group ofpatients who would/may go on tohave prostate cancer or not.
It was agreed, as numbers wereexpected to be small, to initially testall males in first time urine retentionpresenting from North West andSouth Lincoln Practice BasedCommissioning Clusters. Althoughthe group acknowledged co-morbidity
Patientpresentsto OOHor GP
Patient sentto A&E for
catheterisation
Discharged fordistrict nursecontact visitwithin 48hrs
District nurse tomake contactvisit & liaise
with GP
GP to review ifnecessary
GP to prescribeTamsulosin
(Alpha Blockers)as per proforma
from A&E
District nurseperforms TWOC(Trial Without
Catheter)14 days after
patientcommencesTamsulosin
Copy ofpathway tobe given to
patient
IntermediateCare
IntermediateCare GP to seewithin 24hrs
Admitted tofollow
alternativepathway
SuccessfulTWOC GPreferralto GPSI
Seen by GPSIin BPH clinic
to inc ProstateSymptom Score
Flow RateBladder Scan
Maximum SymptomsReferral to
urology team insecondary care
Referral faxed toone number
Minimum SymptomsDischarge to GP
If abnormalDRE
If TWOC unsuccessfulcatheter reinserted
Failed reinsertionPatient referred
directly to EAU at LCH
Community nurse completesproforma & faxes GP for
referral to urology team insecondary care
PSA result toGP to initiate2WW referral
Figure 14: Proposed primary care pathway for male patients with acute urine retention
WinningPrinciple 1

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 19
A&E with MIWent in
retention
Dischargedwith
catheter
TWOC bycommunity
nurse
SuccessfulDischarged
to GP
PATIENT 1
Presentedto EAU
Dischargedwith
catheter
Admitted withsymptomsrelated toupper GI
cancer
TWOC’don theward
Successfuldischrge but
has sincedied
PATIENT 2
Presentedto OOH
Catheteredby OOH GP
TWOC bycommunity
nurse
Failed TWOCReferred back to urology
team. Seen in 11 days
PATIENT 3
Figure 15: Stage one - acute urine retention pathway
reasons for admissions it felt thatthere was a need to test a pathway inorder to:
• Reduce inappropriate admissions tohospital
• Provide an opportunity formanaging acute urine retention inprimary care
• Promote different ways of workingand identifying opportunities formaking services available in analternative setting.
• Reduce unnecessary lengths of stayin acute hospitals and value patientstime.
A pathway was initially developed toenable the total management of acuteurine retention in primary care butafter long and in depth consultationthere were patient safety concernsand clinical governance issuessurrounding the training ofcommunity nurses about first timecatheterisations in the community thatwere unable to be resolved.
The group compromised from movingthe pathway entirely into primary careto having the first catheterisation inUnited Lincoln Hospital NHS TrustA&E department. Unfortunately, A&Estaff felt they were unable toaccommodate the testing of the newpathway at the time. The groupsecured the Emergency AssessmentUnit (EAU) as the single point ofaccess for patients to have theircatheters inserted.
Stage one - Acute urine retentionpathwayInitially testing commenced for a threemonth period. At the end of thisperiod only three patients had beenthrough the pathway, these numberswere less than the period which wasanalysed for the baseline. It wasintimated at the start by clinicalstakeholders that numbers would besmall but they were lower thanoriginally predicted. The evaluation ofstage one identified:
The two patients who had their trialwithout catheter in the communitywere seen by day 12 as per protocoland patient did not have to return toacute trust for this procedure.
The communication between allparties in primary care worked veryefficiently. The patient who had afailed trial without catheter wasreferred to urology team in acute trustvia the GP and this cut the wait forappointment from 42 days to 11 days.
The task group felt reassured thatalthough numbers were small theprinciples of the pathway could workand that the original hypothesis hadnot changed. The clinicalmanagement pathway had reducedunnecessary admissions to hospitaland reduced the number of visits forthe patient. It was agreed to moveforward to the next phase and thatnegotiations should continue with keypeople in order to commence the nextstage of testing. However, progress inthis area has been slow. Themembership of the group hasincreased inviting colleagues from theout of hours team to join. Meetingshave been held with primary carecolleagues to negotiatecommencement of the next stageunfortunately, to date there has stillbeen no sustainable and robustagreement made to establish theclinical management pathway foracute urine retention across thehealth community.

20 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Good idea - tested - can deliverpatients receiving right care in theright place at the right time - sowhat went wrong what have welearned
Clinical champion: During the initialtesting one of the clinical championsfrom the PCT left and it was difficultto find another to join with theGeneral Practitioner with SpecialistInterests (GPSI) to help drive the work.The GPSI was a great support andhelped refocus the group to worktogether to progress to next stage oftesting
Eliminating and managingthe risk factorsThere was a reluctance to reachagreement surrounding first timecatheterisation in primary care and theneed to secure a safe environment asper local clinical governancecatheterisation policy. The clinicalgovernance issues became the focuspoint rather than re -examining thepatient care pathway and these issueswere not resolved, but testing moved.Further work in this area is required ifcare is to be delivered in thecommunity.
It takes timeNot to underestimate the length oftime it takes to ensure all keyrepresentatives from primary andsecondary care are round a table,engaged, have a clear communicationplan and signed up from thebeginning. Dedicated time was alsoallocated with individuals attemptingto overcome ongoing reluctance toconsider changing working practices.
Buy-in - ownership - responsibilityGaining buy-in, ownership andresponsibility from all key stakeholdersis not easy and dealing with thediversity of agendas and differences isdifficult without strong clinical andmanagerial leadership.
GP compliance to the pathwayHigh quality care does save moneyand GP are in a good position to takethis pathway forward and benefitmore than cancer patients.
PerceivedBenefits
of Acute UrineRetentionPathway
For PatientsNo attendance at A&E
No admissionNot as many handoffs
as original pathwayDirect referral
back to urologyteam
For StaffReduction in
patients returningto acute trust for
trial without catheterA defined pathway
Collaborativeworking
For PCTDevelopment ofa clear pathway
across theWhole Health
Community
For Acute TrustReduction in LOS
Reduction ininappropriate
admissions
Figure 16: The perceived benefits of the acute urine retention pathway
Despite all the challenges anddifficulties, the principles of thepathway appear to be right and thereare benefits that can be realised andsupport the transferability of theWinning Principles.

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 21
• Fatigue• Benefits• Social services• Supporting the needs of carers• Nutrition• Cancer information• Complementary therapies• Look good feel better• Support groups.
Self Management Programme (SMP)for cancer patients and carers
BackgroundPatients and carer's had raisedfrustrations regarding unnecessaryadmissions to hospital for symptommanagement. Baseline analysisshowed that four presentingsymptoms dominated, these wereshortness of breath, pain,falls/collapse and diarrhoea, whichrepresented 65% of recordedsymptoms, 76% of these symptomswere related or possible related to thepatients cancer (Table 1 East MidlandsCancer Network).
Taking an integrated approachto developing a patient SelfManagement Programme (SMP)A patient self managementprogramme (SMP) aimed to empowercancer patients and their carers inmanaging their own symptoms wasdeveloped for testing.
15 different organisations wereinvolved in the development, bringingdifferent perspectives and expertise.The Self Management Programmewould provide advice, support andinformation on symptommanagement, coping strategies andliving with cancer.
Collapse, slips, trips & falls
Diarrhoae, constipation
Emergency
End of life
Infection
Pain
SOB
TIA
Unable to cope
Urinary/urology
Treatment related
Bleeding
Unwell
0 5 10 15 20 25 30 35 40 45 50
Related Possible Related Unrelated
4
7
11
6
1
3 10
33 4
41518
262
1
1 4
18
9 13 26
1 1
4
3
3 1
10 5
Figure 17: Out of hours pathway for cancer patients(EMCN 2008 - data period: 07/07/2008 - 31/12/08)
Figure 18: Integrated working community
Sherwood Forest Hospitals NHS Foundation Trust
East Midlands Cancer Network
Social Care Services
Macmillan Cancer Support
John Eastwood Hospice
Notts County Teaching PCT
Nottinghamshire Health Informatics Service
Nottingham University Hospital Trust
Sherwood Forest Hospitals NHS Foundation Trust
Expert Patients
Crossroads North Notts
Look Good Feel Better
Department of Work & Pensions
Job Centre Plus
Complementary therapists
Nottinghamshire Community Health
The programme consisted of a total offive sessions each session involved aninteractive element.
Range of topics covered in the selfmanagement programme• Pain management• Anxiety and coping• Breathlessness• Exercise
WinningPrinciple 4

22 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Impact and outcomesA course evaluation (reproduced fromthe Glasgow Caledonian UniversityCaring With Confidence, Knowledgeand Skills Training For Carers) wascompleted by all course attendees onthe final day of the programme and afocus group was arranged for sixweeks following the end of the courseto evaluate learning.
A pre-course evaluation wascompleted on week one and repeatedthree months post course to assessthe impact on the attendees everydaylives. The questions were all based onsymptoms and situations over the lasttwo weeks and the evaluation wastaken from 'Macmillan NewPerspectives course evaluation'. Eachof the evaluation areas was scaledfrom 1-10 with 10 being a negativeresult and 0 being most positive.
The questions were themed across thefollowing areas: Fatigue, Pain, Stress,Daily Activities (chores, socialising etc)and Exercise. Since attending the SMP67% of all patients felt that theirlevels of fatigue had decreased, 83%of all patients felt that their levels ofpain and stress had decreased andthere ability to perform daily activitieshad increased. 100% of patients saidthat they had not changed theamount of exercise they wereundertaking since the completion ofthe course.
Extremely useful Very useful
A little use
67%
11%
22%
Figure 19: How useful was whatyou learned?
Very good Excellent
67%
33%
Figure 20: Where would you rateyour overall experience of the course?
Pre SMP Post SMP10
9
8
7
6
5
4
3
2
1
0Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
Patient
Eval
uat
ion
scal
e1-
10(1
0b
ein
gth
em
ost
pro
ble
mat
ic)
Figure 21: Fatigue
Pre SMP Post SMP
12
10
8
6
4
2
0Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
Patient
Eval
uat
ion
scal
e1-
10(1
0b
ein
gth
em
ost
pro
ble
mat
ic)
Figure 22: Pain

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 23
Averted A&E attendancesThere were 3 (43% of test patients) A&E attendances averted during the testdue to techniques learnt at the SMP.
Pre SMP Post SMP10
9
8
7
6
5
4
3
2
1
0Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
Patient
Eval
uat
ion
scal
e1-
10(1
0b
ein
gth
em
ost
pro
ble
mat
ic)
Figure 23: Stress
Pre SMP Post SMP4.5
4
3.5
3
2.5
2
1.5
1
0.5
0Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
Patient
Eval
uat
ion
scal
e1-
10(1
0b
ein
gth
em
ost
pro
ble
mat
ic)
Figure 24: Daily activities
Cash flow release £(A&E only based standardtariff of £80)
£80 x 3 = £240
3 x average LOS 6.5 days =19.5 bed days
Test (six weeks and seven patients)
Potential bed delays released during test
The benefits identified fromtesting the SMPQuality• Reduces pathway delays -Integrated working has ensuredhealth and social sectors worktogether identifying social problemsprior to crisis point as opposed tothe current pathway
• Offer a proactive new model ofcare
• Delivers care in the mostappropriate setting
• 86% of patients prior to the coursewere not receiving their full benefitentitlements.
Productivity• 43% of attendees managed ananxiety attack, where they hadpreviously attended A&E fortreatment
• Potentially released 19.5 bed days(three patients x 6.5 day averageLOS)
• Potential financial cash flow releaseof £6,870 (£80 A&E standard tariff+ £340 bed day tariff x 3 patients)
• Techniques taught resulted inprevented anxiety relatedadmissions.
Patient experience• Values patients’ time and addressespatient stakeholder expectations
• Delivers care at home wherenecessary and where appropriate
• Empowers patient to accessinformation and services acrosshealth and social care.

24 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Two of the integrated communitieswere unable to produce case studiesrelating to their work as they felt thework had not come to fruition.Discussions with these organisationsand other (non- test sites) who hadexperiences of integrated workinghighlighted the following complexitiesand key areas of learning:• Integrated working acrossorganisations requires a high inputof time and a dedicated resource toaccelerate the pace of delivery.
• Local trusts and organisations areunder considerable pressure andneed to balance the day to daywork with trying out new ideas. Thewillingness is there but the reality isthat often this is difficult.
• Strong leadership is vital forintegrated working.
• The cancer agenda is huge andalthough seen as a priority by someorganisations it is not seen as apriority across all organisationsinvolved. The alignment of prioritiescan be difficult and all theintegrated organisations want togain something from testing.
• Not all organisations want to sharethe burden of improvement.
• Bringing different organisationstogether to work on a common goalmakes common sense, but thedifferent organisations havedifferent values and cultures andthis can get in the way of progressand needs time to understand.
• Forming relationships and trust isthe key to successful integratedworking.
• Integrated working can expose theshort-comings of organisations andpeople and there are those who willnot wish to take this risk.
Lessons from other integrated workingcommunities
• Integrated working is the future andit can work and benefit the wholehealth community, but it will takeyears, it's a longer term strategy.The testing has shown us howdifficult this can be but given usvaluable lessons to build upon.
• There can be difficulties inestablishing a shared purpose andaligning priorities acrossorganisations. This requires amanaged programme of change.
• Keep the focus onpatient/client/carers benefits.
This demonstrates the difficulties ofestablishing a shared purpose andalignment of priorities acrossorganisations and illustrates thatintegrated improvement requires amanaged programme of change.
What theses two sites would havedone differently?• Join the work up - there are lots ofseparate pieces of serviceimprovement and redesign goingon, but they are in silos, separateprojects.
• Focus on service improvement thatbenefits all patients - wholesystems.
• Cancer should not be seenseparately, we are trying to fit it intoexisting pieces of work.
• Dedicated individuals leading thework.
• Be realistic about the time - thingstake much longer than expected.

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 25
Using a practical service improvementframework for testing, the integratedworking communities share thechallenges they faced, and makerecommendations for otherorganisations attempting to achieveintegrated working.
A practical service improvement frameworkto support integrated working
AnalysisBaseline from
differentperspectives
VisioningWhat are you
trying toachieve?
Testing cyclesTest out
ideas
Identifywhat is the
real problem
Is it theright solution to
address thereal problem?
EvaluationEvaluate the
benefits. Whatis the difference?
Case for changePlan the
implementationof the tested idea
Agree theredesign and
implementation of theimprovements
Implementation
Spread andadoptionstrategy
Evaluateand check
sustainability
Data gatheringNotes analysis
Patient discovery interviews
Stakeholder event allorganisations/services
involved
Develop workinggroups to take
forward testing ideas
Processing mapHome to home
Identify repetition and rework
Areas for testingreviewed for clarity
and agreed
Prepare business casebased on outcomesimpact of testing
What has been theimpact of the testing.
Quantify
Outcomesreported to
executive groups
Patient & staffquestionnaires
Gather patients views
What the integrated sites did
Figure 19: Service Improvement Framework supporting integrated working

26 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Main challengesidentified by all sites
Engagement/timeEngaging strategic andclinical leadership
Engagement of all keystakeholders
Lead in time
Delivering the samemessage for differentaudiences/organisations
Overcoming reluctance tochange
Reluctance to considerchange in working practices
LeadershipAchieving appropriateleadership across ALLorganisations involved
Communication &coordinationOrganisations need tounderstand each other andhow they differ
Complexity of establishingmeetings with multipleorganisations
Ensuring all involved areaware of progress
Information/dataMeasuring the impact ofchange
Integration of systems
Governance differs acrossorganisations
Distractions
Overcoming the challenge(what they did)
Establish an executive steering group with appropriateleadership from all organisations involved
Organise visioning events for all involved across thepatient pathway - home to home.
Ensure good planning build in realistic time frames
Align the testing work with differing organisationalpriorities that meet local/national indicators
Nominate a champion/s in each organisation - createa culture of ownership
Develop smaller working groups to take forward theareas of testing
Take a three pronged approach to leadership,executive, clinical and operational leaders all need tobe involvedExecutive steering groups are helpful for providingdirection
Develop communication pathways between allorganisations involved
Develop clear, concise, graphical communication andprocess algorithms
A news letter is a quick and effective way tocommunicate to a wider audience
Develop outcome measures at the start of the testing
Agree methods for data collections
Involve people from your IT departments early in thework
Involve the appropriate people, think wider than thechanges to the service delivery
Review the scope of the work on a regular basis tokeep the work on target
Outcomes
Commitment and enthusiasm fromstakeholders involved in this work.
Tapping into to the power ofpatients, extremely valuable
Developing a culture that allowedfor working in true partnership
Sharing ideas and practices andimproving knowledge of eachothers organisations
Building new and lastingrelationships for future working
Improved communication with GPsaverted inappropriate admissions
Patients and carers learn from peersas well as professionals
Sharing patient information acrossorganisations involved has beenrelatively easy, with the support ofthe right people
Be realistic - some things may needto take a priority for a short periodof time e.g. Swine Flu campaign
The following identifies the challenges the integrated working communities faced and how they overcame them.
Challenges faced and overcome

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 27
The integrated working communitiesidentified common themes around thepatient/carer experience involving
Communication;• Lack of and inconsistent Information• Unclear pathways of care that weredifficult to navigate
• Lack of clarity surrounding whereand who to go to for support
• Patients/carers continue to beconfused about who to contact andwhere to go out of hours.
Valuing patients time;• Admissions into hospital were notalways necessary but became thedefault as patients did not knowwhere to go
• Easily managed symptoms werepresenting as emergencies andcould be managed at home
• Unnecessary long lengths of stay forpatients admitted as an emergency.
Patient choice and preferredplace of care;• High numbers of emergencyadmissions ending in death withinthe first 24 - 48 hours of admission,as integrated working was notevident and patient choice andpreferred place of care not activatedor communicated.
Key learning: Patient and carer experience

28 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
‘It takes willingness, determination and a desire from allthe organisations, teams and disciplines of staff involvedto overcome the challenges if they are to win through todeliver services in a truly integrated way to patients.’
1. Communication: Develop arobust communication mechanismbetween all organisations toensure engagement of all keystakeholders from the beginning.
2. Leadership: Do not commenceunless executive, clinical andoperational leadership has beenidentified across ALLparticipating organisations.
3. Patient, user and carerinvolvement: Listen - Start theconversations with the users atthe beginning they really knowwhat happens, it happens tothem!
4. Involvement: Cancer networksare a useful resource, they havethe ability to work acrossorganisational boundaries andbring organisations together.
5. Integration champions: identifyand establish a champion withineach organisation.
6. Engagement and ownership:Equal playing fields, acknowledgeall the issues and ways of differentworking, identify the commondenominator with and across allorganisations involved.
7. Win win: Identify the wins foreach organisation aligned to theorganisations strategic objectives.
8. Direction: Establish a steeringgroup - ensure members have thenecessary skills to action andinfluence decisions.
9. Assumptions: Don't make themand where you have, test themout- a solution identified assuccessful in one area may notwork in another - adapt.
Achieving integration - 12 recommendations
10. Evaluate and measure: Agreethe measurable outcomes acrossthe different organisations. So allachieve and can showimprovement in the quality,efficiency and the patientsexperience; remember to captureand demonstrate the impact andagree what success looks like.
11. Time: Do not under-estimate thetime needed to establish and buildrelationships. This is crucial andwithout investment in time andpeople, integration is unlikely tobe successful.
12. Stability and sustainability:Keep testing the strength of theintegrations. A team is only asgood as its weakest link.
The integrated working communities demonstrated that integration can be achieved, but that integration in reality isstretching many organisations. The sites make the following recommendations

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 29
Testing the transferability of theWinning PrinciplesTransferring the Winning Principlesinto an integrated working approachto deliver services for cancer patientsand their carers can be achieved.However what the organisations andthe range of patients, carers and staffinvolved in this work havedemonstrated is that this is not easyto do. It involves significantchallenges, and it needs a real senseof determination if organisations areto win through to work in this way.The test sites have shared with ustheir experience of integrated workingand this embraces valuable learningthat will assist other organisationswith the integrated delivery of cancerservices.
This work supports the current healthlandscape. Delivering improvements inaccess and quality for cancer patientsand their carers will remain a focus ofcontinuous improvement (Revision tothe Operating Framework for the NHSin England 2010/11). The programmewill continue to support spread anddisseminate the practical learningacross the NHS to benefit all patients.
Conclusion

30 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Appendices
The NHS Plan2000Vision for care based on integrationbetween health and social care.Establishment of care trusts to bringtogether the commissioning ofservices
Health and Social Care Act2001New role for local government in thescrutiny of local health services
Choosing Health2004Concept of partnership arrangementswith statutory bodies, voluntaryorganisations and others
Local Area Agreement Pilots2004/5To improve service delivery, efficiency,partnership working.
Independence, well being and choice2005Better integration between social careand PCTs. Focus on outcomes forservices users
Our Health, Our Care, Our Say2006Joint commissioning, linking healthand social care. Practice basedcommissioning to realign healthy andsocial care to deliver services closer tohome and more effectively
National Health Service Act2006Consolidation of previous legislation,removal of inconsistencies, s.31Health Act 1999 replaced with s.75NHS Act 2006
Putting People First2007Concordat between government, NHSand Adult social care. Charged localauthorities with system widetransformation by 2011
Commissioning Framework for Health& Well-being2007Introduction of Joint Strategic Needsassessment for NHS andlocal authorities.
High Quality Care for All2008Development of a series of integratedcare pilots, operating alongsidehospital, community and social care.Delivering care closer to home.
Health and Social Care Bill2008Significant measures to integratehealth and social care, creation of theCare Quality Commission, bringingtogether regulation of health andsocial care into one regulatory body.
World Class Commissioning2008Seeks to improve the way health andcare are commissioned, strategic longterm vision for delivering health care
Green Paper 'Shaping the Future ofCare Together2009Local authorities to harness thecapacity of the whole system of highquality care environments through thedevelopment of commissioningstrategies.
Transforming Community Services2009Details how thecommissioner/provider split will workwithin PCTs to provide communityservices
Integrated Care Pilots2009Developed to test a range of modelsof integrated care
Operating Framework2009Deliver cash releasing strategies, whilesustaining and improving quality
From Good to Great2009Taking responsibility for care along thewhole pathway. Acceleratedimprovements in cancer and patientexperience
The State of health care and adultsocial care in England2010First report that sets out how wellhealth and social care services inEngland performed in 2009, and theimprovements leading up to 2009
Appendix 1
Publications underpinning Integrated working over the last decade

• Patients & Carers
• Consultants
• Oncologists
• Doctors (Including Out of Hours staff)
• General Practitioners (GPs)
• GPs with Specialist Interest (GPSI)
• Clinical nurse specialists (CNS)
• Incontinence nurses
• District nurses
• Community matrons
• Telephone triage nurses
• Nurses (Including Out of Hours staff)
• Healthcare Assistants
• Occupational therapists
• Physiotherapists
• Complimentary therapists
• Dieticians
• Executive Management
• Managers, from NHS, Social Care, PCT, Ambulance Service, Macmillan, Community Providers
• GP Practice managers
• Service Improvement leads
• Service Improvement Facilitators
• Service Improvement Officer
• Local Improvement Leads
• Pharmacists
• Clinical Illustration/photographer
• End of Life Facilitators
• Ambulance Call Handlers
• Hospice staff
• Walk in Centre staff
• Voluntary organisations/Charities including Crossroads, Macmillan, Look Good Feel Better
• Department of works and pensions (Benefits)
• Job centre plus (Employment)
• Informatics staff
• Data Analysts
• Caldicott Guardian/Clinical Governance Staff
• NHS Direct
• PCT Commissioners
• Training Coordinator
An integrated approach: The transferability of the Winning Principles - Sharing the learning | 31
Appendix 2
The range of people involved across all of the Integrated Working Communities

32 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Websites and useful reading
Websites
Putting People First - TransformingAdult Social Carewww.puttingpeoplefirst.org.uk/
DH Care Networks - Integrated CareNetworkwww.dhcarenetworks.org.uk/icn/index.cfm
NHS Improvementwww.improvement.nhs.uk
NHS Improvement - TransformingInpatientswww.improvement.nhs.uk/cancer/inpatients/new_inpatients.html
Useful reading
A practical guide to Integratedworking - Care Services Improvementpartnership, Integrated Care Network2008
The Evidence base for integrated care(2009) - DOH Dr Angus Ramsey andProf Naomi Fulop NIHR Kings PatientSafety and Service Quality ResearchCentre - Kings College London
Putting People First (2007) A sharedvision and commitment to thetransformation of Adult Social Care.
Department of Health - DirectPayments For Health Care: Aconsultation on proposals forregulations and guidance (2009).
Department of Health -Understanding personal healthbudgets (2009).
Department of Health - Revision tothe Operating Framework for the NHSin England 2010/11. (2010).
Department of Health - Shaping thefuture of care together (2009) GreenPaper.
The Coalition:Our programme forGovernment (May 2010) CabinetOffice, London.
Fulop, N., Mowlem, A. & Edwards, N.(2005) Building integrated care:Lessons from the UK and elsewhere.London, The NHS Confederation.
NHS Improvement - TransformingInpatient Care Programme for CancerPatients, The Winning Principles, NHSImprovement. (April 2008).
NHS Improvement - TransformingInpatient Care ProgrammeFrom Testing to Spread - Sharing theknowledge and learning fromorganisations spreading the WinningPrinciples. (July 2010).
NHS Improvement - TransformingInpatient Care ProgrammeConsolidation Report (2009): Fromtesting to spread. (July 2010).
NHS Improvement - TransformingCare for Cancer Patients - Spreadingthe Winning Principles and GoodPractice. (July 2009).
NHS Improvement – TransformingInpatient Case Studies. (July 2009).
NHS Improvement - TransformingInpatient Care Programme for CancerPatients - Meeting the Challengetogether…. delivering care in themost appropriate setting. (October2008).

An integrated approach: The transferability of the Winning Principles - Sharing the learning | 33
NHS Improvement would like to thank all those involved from the integratedcommunities test sites for their support and input into this challenging area ofwork. Their contribution, cooperation and determination has identified thepotential for improving cancer services using an integrated approach, it has alsoidentified that this is not easy to achieve and involves significant challenges.
Acknowledgements

34 | An integrated approach: The transferability of the Winning Principles - Sharing the learning
Further information
Transforming Inpatient Team:
Angie RobinsonNational Improvement [email protected]
Marie TarpleeNational Improvement [email protected]
Catherine [email protected]


3rd Floor | St John’s House | East Street | Leicester | LE1 6NB
Telephone: 0116 222 5184 | Fax: 0116 222 5101
www.improvement.nhs.uk
NHS Improvement
With over ten years practical service improvement experience in cancer,diagnostics and heart, NHS Improvement aims to achieve sustainableeffective pathways and systems, share improvement resources andlearning, increase impact and ensure value for money to improve theefficiency and quality of NHS services.
Working with clinical networks and NHS organisations across England,NHS Improvement helps to transform, deliver and build sustainableimprovements across the entire pathway of care in cancer, diagnostics,heart, lung and stroke services.
Delivering tomorrow’simprovement agendafor the NHS
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
©NHSIm
provem
ent20
10|AllRigh
tsRe
served
|July20
10
NHSNHS Improvement