Embed Size (px)
Citation preview

PRESENTED BY:
VISHNU.R.NAIR,
4TH YEAR PHARM.D,
NATIONAL COLLEGE OF PHARMACY(NCP)

GENERAL INTRODUCTION
EPIDEMIOLOGICAL STATISTICS
ETIOLOGY/ RISK FACTORS FOR AD
NORMAL PHYSIOLOGY AND PATHOPHYSIOLOGY
CLINICAL MANIFESTATIONS OF AD
DIAGNOSTIC PRINCIPLES AND MEASURES
MANAGEMENT STRATEGIES FOR AD
BIBLIOGRAPHY/ REFERENCE

1. “NEURODEGENERATIVE DISORDER, characterized by COGNITIVE & BEHAVIOURAL IMPAIRMENT, that significantly INTERFERES with SOCIAL & OCCUPATIONAL FUNCTIONING”
2. Incurable disease, with a LONG & PROGRESSIVE COURSE
3. In AD PLAQUES form in HIPPOCAMPUS (A structure deep inside the brain, that helps in MEMORY ENCODING) & in other areas of CEREBRAL CORTEX, that are used in THINKING & MAKING DECISIONS
4. Most common cause of DEMENTIA
5. Between 50-60% of all cases of dementia can be attributed to AD
6. Disease is named after DR.ALOIS ALZHEIMER, a German Doctor, who , during an AUTOPSY in 1906, discovered physical changes in the brain of a woman, who died of a strange mental illness
7. He found PLAQUES & TANGLES in her brain (Signs, that are now considered as “AD HALLMARKS” )

1. According to a 2015 report AD affects 5.3 MILLION PEOPLE in US
2. 2,00,000 people , younger than 65 years constitute the YOUNGER ONSET US population with AD
3. AD was the 6th leading cause of DEATH in 2015
4. AD and other DEMENTIAS are more likely common in AFRICAN AMERICANS , than in WHITES
5. According to the WHO’S REVIEW in 2000, on the “GLOBAL BURDEN OF DEMENTIA” :
- Approximate rates of dementia are under 1% in persons aged 60-69 years ; and 39 % in persons aged 90-95 years
- Prevalence DOUBLES with every 5 years of age (within the above ranges) ……………

1. ADVANCING AGE (Especially> 65 years)
2. FAMILY HISTORY
3. OBESITY
4. INSULIN RESISTANCE (According to a study by BAKER ET AL)
5. VASCULAR FACTORS
6. DYSLIPIDEMIA
7. HTN
8. INFLAMMATORY MARKERS
9. DOWN SYNDROME (A common birth defect , that is usually due to an extra chromosome 21 , associated with MENTAL RETARDATION, & MULTIPLE MALFORMATIONS)

10. TRAUMATIC BRAIN INJURY
11. HIGH ALUMINIUM LEVELS
12. LONG TERM USE OF NSAIDs
13. GENETIC CAUSES:
- Mutations in the following genes increases risk of ALZHEIMER’S DISEASE:
a. AMYLOID PRECURSOR PROTEIN (APP) GENE, on CHROMOSOME 21
b. PRESENILIN-1 (PS-1) GENE, on CHROMOSOME 14
c. PRESINILIN-2 (PS-2) GENE, on CHROMOSOME 1
- Presence of the following SUSCEPTIBILITY LOCI also increase AD risk:
a. APOLIPOPROTEIN E EPSILON 4 (APOE E4) GENOTYPE
b. CLUSTERIN (CLU) GENE
c. PHOSPHATIDYLINOSITOL- BINDING CLATHRIN ASEMBLY PROTEIN (PICALM) GENE

d. COMPLEMENT RECEPTOR-1 (CR-1) GENE
e. ATP-BINDING CASSETTE SUBFAMILY A MEMBER 7 GENE (ABCA 7)
f. MEMBRANE- SPANNING GENE CLUSTER (MS4A6A/ MS4A4E)
g. EPHRIN- RECEPTOR 1 (EPHA1)
h. CD33
i. CD2AP
14. DEPRESSION (ACCORDING TO FRAMINGHAM STUDY DATA)
15. INFECTIOUS CAUSES:
i. Treponemas
ii. Borrelia burgdorferi
iii. HSV1 …………………

The changes that take place in the brain, begins at the MICROSCOPIC LEVEL, long before the FIRST SIGNS OF MEMORY LOSS occurs
Here, we will see the NORMAL PHYSIOLOGY of the brain’s neuronal activities, and the pathological cascades associated with AD PATHOPHYSIOLOGY……………………

1. NORMAL PHYSIOLOGY:- The brain has 100 BILLION NERVE CELLS (NEURONS)
- Each NEURON Connects to many others of the same forms COMMUNICATION NETWORKS
- In addition to neurons brain also includes CELLS specialized to SUPPORT & NOURISH other cells
- Group of NEURONS possess special functions
- Some are involved in THINKING, LEARNING & MEMORY
- Others help us SEE, HEAR, SMELL , & TELL OUR MUSCLES WHEN TO MOVE
- Neurons also receive supplies, generate energy, construct equipment and get rid of waste
- Cells also PROCESS & STORE INFORMATION AND COMMUNICATE with OTHER CELLS
- Keeping everything running requires CO-ORDINATION as well as LARGE AMOUNTS OF NUTRIENTS & OXYGEN……………………..

2. PATHOPHYSIOLOGY:- Scientists believe that AD PREVENTS parts of a CELL’S FACTORY from
running well
- Just like a real factory BACKUPS & BREAKDOWNS in one system causes problems in other areas naturally
- As the damage spreads cells LOSE THEIR ABILITY to do their JOBS Eventually DIE
- ROLE OF PLAQUES & TANGLES:
A. Brains of individuals with AD have an ABUNDANCE of PLAQUES & TANGLES
B. PLAQUES : “Deposits of a PROTEIN FRAGMENT called BETA-AMYLOID, that builds up in the SPACES between NEURONS”
C. TANGLES : “TWISTED FIBRES of another PROTEIN called TAU, that builds up INSIDE CELLS”

- Although AUTOPSY studies show that most people develop some plaque & tangles as they AGE
Those with AD tend to develop them FAR MORE, & in a PREDICTABLE PATTERN
They develop in the areas important for MEMORY before SPREADING to other REGIONS
PLAQUES & TANGLES DISABLE/ BLOCK COMMUNICATION AMONG NEURONS
Gradually SPREAD to other areas of BRAIN

Causes MEMORY FAILURE, PERSONALITY CHANGES, PROBLEMS in CARRYING OUT DAILY ACTIVITIES & other SYMPTOMS of ALZHEIMER’S DISEASE………………….

AD can be divided into 5 STAGES:
1. PRE-CLINICAL AD:i. Patient may appear NORMAL on PHYSICAL EXAMINATION & MENTAL
STATUS TESTING
ii. Specific regions of brain (ENTORHINAL CORTEX, HIPPOCAMPUS) are likely to be affected DECADES BEFORE ANY SIGNS/ SYMPTOMS APPEAR
2. MILD AD:Signs include:
i. Memory loss
ii. Confusion about location of familiar places
iii. Taking longer time to accomplish NORMAL, DAILY TASKS
iv. Trouble in HANDLING MONEY & PAYING BILLS

v. COMPROMISED JUDGEMENT, often leading to BAD DECISIONS
vi. Loss of SPONTANEITY & SENSE OF INITIATIVE
vii. MOOD & PERSONALITY CHANGES
viii. Increased ANXIETY
3. MODERATE AD:Signs include:
i. Increased MEMORY LOSS
ii. Increased CONFUSION
iii. SHORTENED ATTENTION SPAN
iv. Problems recognizing friends & family members
v. Difficulty with LANGUAGE
vi. Problems with READING, WRITING, WORKING WITH NUMBERS
vii. Difficulty ORGANIZING THOUGHTS and in LOGICAL THINKING
viii. Inability to LEARN NEW THINGS/ to COPE with NEW/ UNEXPECTED SITUATIONS

ix. Restlessness
x. Agitation
xi. Anxiety
xii. Tearfulness
xiii. WANDERING, especially in the LATE AFTERNOON/ NIGHT
xiv. REPITITIVE STATEMENT/ MOVEMENT
xv. Occasional MUSCLE TWITCHES
xvi. Hallucinations
xvii. Delusions
xviii. Suspiciousness/ paranoia
xix. Irritability
xx. LOSS OF IMPULSE CONTROL (eg: undressing at inappropriate times/places, etc.)
xxi. PERCEPTUAL-MOTOR PROBLEMS (eg: trouble getting out of a chair/ setting the table)

4. SEVERE AD:- Patients with SEVERE AD Can’t recognize family/ loved ones
- Can’t communicate effectively
- Completely dependent on others for care
- All sense of self seems to vanish
- Other symptoms include:
i. WEIGHT LOSS
ii. SEIZURES
iii. SKIN INFECTIONS
iv. DYSPHAGIA
v. GROANING, MOANING/ GRUNTING
vi. INCREASED SLEEPING
vii. LACK OF BLADDER & BOWEL CONTROL

5. END-STAGE AD:- During END-STAGE AD Patients are in bed all of the time
- Death usually occurs due to other illnesses, notably ASPIRATION PNEUMONIA………………………………..

DIAGNOSTIC PRINCIPLES INCLUDE:
1. BLOOD STUDIES:- Laboratory tests can be performed to rule out other conditions that may cause
COGNITIVE IMPAIRMENT
- According to AMERICAN ACADEMY OF NEUROLOGY(AAN) recommendations Measurement of COBALAMIN (VITAMIN B12) and THYROID FUNCTION SCREENING TEST is useful
- ABNORMALITIES in CBC& VITAMIN B12 levels require further work-up to rule out HEMATOLOGIC DISEASE
- ABNORMALITIES IN LFTs require further work-up to rule out HEPATIC DISEASE
- ABNORMALITIES in THYROID STIMULATING HORMONE levels require further work-up to rule out THYROID DISEASE

- ABNORMALITIES in RAPID PLASMA REAGENT(RPR) levels require further work-up to rule out SYPHILIS
- ABNORMALITIES in HIV SEROLOGY/ PCR require further work-up to rule out HIV/AIDS
- ABNORMALITIES in PARANEOPLASTIC ANTIBODIES require further work-up to rule out AUTOIMMUNE ENCEPHALITIS
- ABNORMALITIES in CSF PROTEINS (TAU, P-TAU, 14-3-3) require further work-up to rule out CREUTZFELDT-JAKOB DISEASE
2. BRAIN MRI/CT-SCAN:- According to AAN guidelines STRUCTURAL NEUROIMAGING with either
CT/MRI SCAN is useful in the EVALUATION of patients with DEMENTIA
- This helps in detection of LESIONS that may result in COGNITIVE IMPAIRMENT (STROKE, SMALL VESSEL DISEASE, TUMORS)
- Also helps to detect CEREBRAL & HIPPOCAMPAL ATROPHY

3. SPECT(SINGLE PHOTON EMISSION COMPUTERIZED TOMOGRAPHY)/ PET(POSITRON EMISSION TOMOGRAPHY) SCAN:- According to AMYLOID IMAGING TASKFORCE(AIT) & the SOCIETY OF
NUCLEAR MEDICINE & MOLECULAR IMAGING (SNMMI) AMYLOID-BETA (PET ) IMAGING is appropriate in patients with PERSISTENT/ PROGRESSIVE , UNEXPLAINED, MILD COGNITIVE IMPAIRMENT.
4. LUMBAR PUNCTURE:- Perform LUMBAR PUNCTURE to rule out conditions, like :
a. NPH(NORMAL PRESSURE HYDROCEPHALUS)
b. CNS INFECTIONS (NEUROSYPHILIS, NEUROBORRELIOSIS, CRYPTOCOCCOSIS)
- CSF levels of TAU & PHOSPHORYLATED TAU is INCREASED in AD
- AMYLOID More concentrated in BRAIN than CSF Thus it is found less in CSF..

5. GENOTYPING:- GENOTYPING for APOE ALLELES is a RESEARCH TOOL that is helpful in
DETERMINING AD risk in populations
- According to INVESTIGATORS from COPENHAGEN GENERAL POPULATION STUDY & COPENHAGEN CITY HEART STUDY :
a. APOE GENOTYPES with HIGHEST risk for AD : EPSILON 43,44
b. APOE GENOTYPES with LOWEST risk for AD: EPSILON 12,22,32,42,33………………………..
6. ELECTROENCEPHALOGRAPHY:- Applicable when CREUTZFELDT-JAKOB DISEASE/ other PRION-RELATED
DISEASE is a likely diagnosis
- PERIODIC HIGH AMPLITUDE SHARP WAVES Detected in most cases of CREUTZFELDT-JAKOB DISEASE
- MULTIPLE,UNWITNESSED SEIZURES Present as DEMENTIA Here, EEG is useful to evaluate such a possibility…………………..

INCLUDES:
1. GOALS OF THERAPY
2. PHARMACOTHERAPY
3. NON-PHARMACOTHERAPY……………..

1. To maintain PATIENT’S BRAIN FUNCTION as far as possible
2. To treat PATIENT’S PSYCHIATRIC & BEHAVIOUR SEQUELAE
3. To decelerate the LIKELIHOOD of PROGRESSION INTO COMPLICATIONS
4. To focus on EMOTIONAL & SUPPORTIVE CARE for the concerned patient
5. To reduce MORBIDITY & MORTALITY as far as possible
6. To improve QOL………………………

A. PHARMACOTHERAPY OF COGNITIVE SYMPTOMS:- Manage B.P, CHOLESTEROL & BLOOD SUGAR reduces risk of developing
AD , and also prevents WORSENING of DEMENTIA in patients with AD
- SYMPTOMATIC ATTEMPTS are only possible to maintain COGNITION
- Drugs used include:
I. CHOLINESTERASE INHIBITORS :- DONEPEZIL
- RIVASTIGMINE
- GALANTAMINE
- TACRINE (FIRST cholinesterase inhibitor approved for the treatment of AD, but is now replaced by safer drugs, with lesser ADRs)
II. NMDA RECEPTOR ANTAGONISTS : MEMANTINE……

B. PHARMACOTHERAPY OF NON-COGNITIVE SYMPTOMS:
- There are some guidelines for the PHARMACOTHERAPY of NON-COGNITIVE SYMPTOMS:
1. Use REDUCED DOSES
2. MONITOR patient closely
3. TITRATE DOSAGE SLOWLY
4. DOCUMENT carefully
5. Periodically, go for REDUCING MEDICATIONS in MINIMALLY SYMPTOMATIC PATIENTS
6. Avoid PSYCHOTROPIC MEDICATIONS having ANTICHOLINERGIC EFFECTS, since they WORSEN COGNITION
- Drugs used include :
1. CHOLINESTERASE INHIBITORS
2. MEMANTINE

3. ANTIPSYCHOTICS
4. ANTIDEPRESSANTS
5. MISCELLANEOUS THERAPIES(CBZ, OXAZEPAM)……………

3. DRUG DETAILS:
A. DONEPEZIL (ARICEPT):- MOA : Drug selectively INHIBITS ACETYLCHOLINESTERASE(Enzyme,
responsible for DESTRUCTION of Ach ) Improves Ach availability
- Drug has LONG HALF-LIFE (70 hours) provides LONG DURATION of DRUG AVAILABILITY for BINDING at RECEPTOR SITES
- Used in :
i. MILD-MODERATE AD
ii. MODERATE-SEVERE AD
- ADRs:
i. SEIZURES
ii. ATRIAL FIBRILLATION
iii. BLURRED VISION
iv. ARTHRITIS

- DRUG INTERACTIONS:
i. DRUG + BETA-BLOCKERS increases risk of BRADYCARDIA
ii. DRUG + CCBs increases risk of DRUG ADVERSE EFFECTS
- DOSE:
i. FOR MILD-MODERATE AD : 5-10 mg OD
ii. FOR MODERATE-SEVERE AD : 10 / 23 mg OD
B. RIVASTIGMINE (EXELON):
- MOA : Drug REVERSIBLY INHIBITS HYDROLYSIS OF Ach by CHOLINESTERASE Increases Ach concentration
- Drug POTENT, SELECTIVE inhibitor of brain ACETYLCHOLINESTERASE & BUTYRYLCHOLINESTERASE
- Used for treatment of AD of MILD-MODERATE DEMENTIA TYPE

- ADRs:
i. HTN
ii. TREMOR
iii. SJS
- DRUG INTERACTION:
i. DRUG + CCB enhanced BRADYCARDIC effect
- DOSE:
i. Initial dosage : 1.5 mg PO, BID
ii. Max. dose : 12 mg/ day PO
iii. Transdermal patch dose : 13.3 mg/ day

C. GALANTAMINE (RAZADYNE) :- MOA :
i. Drug enhances CENTRAL CHOLINERGIC FUNCTIONS
ii. Inhibits AChE
iii. Drug MODULATES NICOTINIC Ach RECEPTOR Increases Ach levels from SURVIVING PRE-SYNAPTIC NERVE TERMINALS
- Drug derived from DAFFODIL BULBS
- ADRs:
i. BRADYCARDIA
ii. TREMOR
iii. RHINITIS
- DRUG INTERACTION:
i. DRUG + ATROPINE Causes ANTAGONISTIC EFFECTS
- DOSE : 16-24 mg/day (MAINTENANCE DOSE)………….

D. MEMANTINE (NAMENDA):- Low-to-moderate affinity, uncompetitive NMDA antagonist
- Drug binds preferentially to N-METHYL-D-ASPARTATE RECEPTOR OPERATED CATION CHANNELS Blocks the receptor
- BLOCKING OCCURS ONLY UNDER CONDITIONS OF EXCESSIVE STIMULATION, and NOT UNDER NORMAL NEUROTRANSMISSION
- ADR:
i. HTN
ii. CATARACT
iii. CVA
iv. THROMBOEMBOLISM
- DRUG INTERACTIONS:
i. COTRIMOXAZOLE + DRUG Causes MYOCLONUS & CONFUSION

- DOSE:
i. Initial dose for immediate release formulation : 5 mg OD
ii. Maximum dose : 20 mg/day
iii. Initial dose for extended-release formulation : 7 mg OD
iv. Maximum dose : 28 mg/day.
- Used for MODERATE-SEVERE DEMENTIA in patients with AD.

E. CAPRYLIDENE (AXONA):
- Prescriptional medical food
- BRAIN-IMAGING STUDIES of OLDER ADULTS and those with AD, reveal a dramatically decreased uptake of glucose
- CAPRYLIDENE Metabolized into KETONE BODIES Provides an ALTERNATE GLUCOSE SUBSTRATE TO BRAIN Brain can use the KETONE BODIES for energy , when its ability to PROCESS GLUCOSE is IMPAIRED
- ADRs:
i. Diarrhea
ii. Flatulence
- INDICATED for CLINICAL DIETARY MANAGEMENT of METABOLIC PROCESSES associated with MILD-MODERATE AD
- Dose : 40 g/ day (during breakfast)

INCLUDES:
A. HOME REMEDIES FOR AD
B. DO’S FOR AD
C. DON’T’S FOR AD

A. HOME REMEDIES FOR AD:
I. NUTRITIONAL SEEDS:
- Seeds of PUMPKIN, SESAME and SUNFLOWER Filled with ESSENTIAL FATTY ACIDS Necessary for BRAIN FUNCTION
II. SESAME OIL:
- Popular AYURVEDIC remedy
- Relieves DEPRESSION associated with AD
- Use 3 drops of WARMED SESAME OIL in each NOSTRIL TWICE DAILY
- You can also rub a little warmed sesame oil on the top of the hand and bottoms of the feet.
III. WHEAT GERM/ POWDERED MILK:
- Above substances HIGHLY PROTEINACEOUS add to foods helps in AD

IV. BLUEBERRIES :
- BLUEBERRIES Contains ANTIOXIDANT Slows down AGE-RELATED MOTOR CHANGES ASSOCIATED with AD
V. BOTTLED WATER:
- TAP WATER May contain ALUMINIUM and other IMPURITIES
- BOTTLED WATER is a better option
- Installing a WATER FILTER is also a good option
VI. CARROTS :
- CARROTS Loaded with BETA-CAROTENE Natural VITAMIN A source improves NERVE HEALTH & MEMORY PROBLEMS associated with AD
VII. CITRUS FRUITS:
- CITRUS FRUITS Contain VITAMIN C Possesses ANTIOXIDANTproperty protect BRAIN NERVES

8. FISH:- Also known as “BRAIN FOOD”
- FISH High in FATTY ACIDS (DHA) Good for NORMAL BRAIN FUNCTION
- Good choices include:
i. SALMON
ii. SARDINES
iii. TUNA
iv. LAKE TROUT
9. DARK GREEN LEAFY VEGETABLES:- LEAFY VEGETABLES Have high levels of FOLIC ACID Stimulates
COGNITIVE FUNCTION
- According to research from the NETHERLANDS People who eat large amounts of DARK GREEN, YELLOW & RED VEGETABLES documented REDUCED RISKS OF DEMENTIA BY 25%

- Sources of FOLIC ACID:
i. SPINACH
ii. KALE
iii. BEETS
iv. BLACK-EYED PEAS
v. BRUSSELS SPROUTS
vi. WHOLE GRAIN FOODS
10. ORANGE JUICE:
- ORANGE JUICE Rich in VITAMIN C Helpful in AD
11. SOY PRODUCTS:
- According to studies SOY PROTEINS contain ISOFLAVONES Protects POST-MENOPAUSAL WOMEN from AD
- Dietary guidelines suggest 20-25 grams of SOY PROTEIN a day

12. ALMOND EXTRACT :- ALMONDS Contain VITAMIN E Helps in people with AD & DEMENTIA
- VITAMIN E Highly FAT SOLUBLE Plays critical role in preventing HARMFUL FAT OXIDATION
13. TURMERIC :- TURMERIC Contains CURCUMIN has ANTI-OXIDANT and ANTI-
INFLAMMATORY properties helps in AD prevention
- This might explain why INDIA has one of the LOWEST AD RATES IN THE WORLD
14. LEMON OIL:- Steep few drops of LEMON/ PEPPERMINT OIL in HOT WATER INHALE
AROMATHERAPY STIMULANT Useful in LETHARGY/ DEPRESSION ASSOCIATED WITH AD
15. SAGE:- Drink a tea made with ½ tsp. SAGE and ¼ tsp. BASIL LEAVES steeped in 1 cup of HOT WATER Cures DEPRESSION associated with AD

16. RESVERATROL:
- Available in RED GRAPES , in SUPPLEMENTS, etc
- According to recent studies RESVERATROL prevents AD by inhibiting TOXIC PROTEINS LINKED TO AD
17. GINGKO BILOBA :
- Helps in MEMORY LOSS
- Prevents INFLAMMATION
- Also acts as ANTI-OXIDANT Protects BRAIN from any DAMAGE
- Can be used both as PREVENTIVE & THERAPEUTIC
18. WALNUTS:
- According to studies DIET rich in WALNUTS Contain ALPHA-LINOLEIC ACID Reduces OXIDATIVE STRESS , by ELIMINATING FREE RADICALS Reduces AD risk and also of CHD……

B. DO’S FOR AD (PATIENT COUNSELLING) :1. Do always check FOOD TEMPERATURE
2. Hot sensations may be numbed for people with AD, but still their tongue can get burned
3. Serve foods that require little chewing, like GROUND MEAT , SOUPS, etc
4. Serve several SMALLER MEALS, rather than THREE MAIN MEALS
5. Do select favourite foods, especially if the appetite is poor
6. Keep in mind that as DISEASE PROGRESSES, FOOD PREFERENCES MAY CHANGE
7. Focus on consuming foods rich in VITAMINS, which serve as perfect NEUROPROTECTIVES
8. Treat conditions of DM, DYSLIPIDAEMIA or HTN (as the case may be)
9. Focus on exercises, deep breathing and morning walks, which provide good oxygen and fuel for brain activities
10. Warm support, family care and affection always prolongs the life and sense of well being in ALZHEIMER patients……………….

C. DON’T’S FOR AD (PATIENT COUNSELLING):1. Avoid CONSUMPTION OF RED MEAT
2. Avoid FRIED, JUNK FOODS
3. Avoid CONSUMPTION OF TAP WATER
4. Avoid consuming foods with BONES
5. Avoid eating foods with a mixture of TEXTURES, since they may be hard to SWALLOW……………………

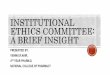
New Alzheimer’s treatment fully restores memory function
Of the mice that received the treatment, 75 percent got their memory function back.
BEC CREW 18 MAR 2015
Facebook Icon Twitter Icon
Australian researchers have come up with a non-invasive ultrasound technology that clears the brain of neurotoxic amyloid plaques - structures that are responsible for memory loss and a decline in cognitive function in Alzheimer’s patients.
If a person has Alzheimer’s disease, it’s usually the result of a build-up of two types of lesions - amyloid plaques, and neurofibrillary tangles. Amyloid plaques sit between the neurons and end up as dense clusters of beta-amyloid molecules, a sticky type of protein that clumps together and forms plaques.
Neurofibrillary tangles are found inside the neurons of the brain, and they’re caused by defective tau proteins that clump up into a thick, insoluble mass. This causes tiny filaments called microtubules to get all twisted, which disrupts the transportation of essential materials such as nutrients and organelles along them, just like when you twist up the vacuum cleaner tube.
As we don’t have any kind of vaccine or preventative measure for Alzheimer’s - a disease that affects 343,000 people in Australia, and 50 million worldwide - it’s been a race to figure out how best to treat it, starting with how to clear the build-up of defective beta-amyloid and tau proteins from a patient’s brain. Now a team from the Queensland Brain Institute (QBI) at the University of Queensland have come up with a pretty promising solution for removing the former.
Publishing in Science Translational Medicine, the team describes the technique as using a particular type of ultrasound called a focused therapeutic ultrasound, which non-invasively beams sound waves into the brain tissue. By oscillating super-fast, these sound waves are able to gently open up the blood-brain barrier, which is a layer that protects the brain against bacteria, and stimulate the brain’s microglial cells to activate. Microglila cells are basically waste-removal cells, so they’re able to clear out the toxic beta-amyloid clumps that are responsible for the worst symptoms of Alzheimer’s.
The team reports fully restoring the memory function of 75 percent of the mice they tested it on, with zero damage to the surrounding brain tissue. They found that the treated mice displayed improved performance in three memory tasks - a maze, a test to get them to recognise new objects, and one to get them to remember the places they should avoid.
"We’re extremely excited by this innovation of treating Alzheimer’s without using drug therapeutics," one of the team, Jürgen Götz, said in a press release. "The word ‘breakthrough’ is often misused, but in this case I think this really does fundamentally change our understanding of how to treat this disease, and I foresee a great future for this approach."
The team says they’re planning on starting trials with higher animal models, such as sheep, and hope to get their human trials underway in 2017.


1. “ALZHEIMER’S DISEASE” ; WELLS.G.B; PHARMACOTHERAPY HANDBOOK, BY DIPIRO.T.J; MCGRAW HILL PUBLICATIONS; Page: 727-734
2. LAKHAN.E.S; CHAWLA.J; ALZHEIMER’S DISEASE
3. www.sciencealert.com/new-Alzheimer’s-treatment -fully-restores-memory-function
4. Health.howstuffworks.com
5. REBECCA.P;“BASICS OF ALZHEIMER’S DISEASE” ; ALZHEIMER’S ASSOCIATION

THANK YOU !!