Embed Size (px)
Citation preview

AIRWAY ASSESSMENT
Presenter: Dr. Sharath K.
Moderator: Dr. Suresh Kumar

AIRWAY ASSESSMENT Three basic decisions needed before
induction of anesthesia in every patient
are whether To use awake endotracheal intubation
To use a percutaneous technique To maintain spontaneous ventilation

Airway tests to detect difficulty with direct laryngoscopy are based on anatomic features, and values have been selected as probable indicators of difficulty.
The combination of mouth opening, jaw protrusion, and head extension is the core of airway assessment

Mouth opening is measured as the inter -incisor distance, and a value of 4 cm (2 fingerbreadths) has been proposed as an indicator of probable difficult intubation.
The prognathic ability of the mandible depends on the size and shape of the mandible in relation to the maxilla and on TMJ function.

Prognathic inability of the mandible (the mandibular incisors cannot be brought in line with the maxillary incisors) is associated with difficult intubation.
Limited head (occipito-atlanto-axial) extension impairs direct laryngoscopy

The Mallampati test (visibility of pharyngeal structures) is of limited value on its own but can be combined with an assessment of dentition.
The thyromental distance is of limited value as a predictor of difficult laryngoscopy,
Examination ensures that the laryngeal cartilage is palpated and
Submandibular compliance assessed.

The larynx consists of a framework of articulating cartilage connected by fascia, muscles, and ligaments.
It is suspended from the hyoid bone by the thyro-hyoid membrane.
The principal cartilages are the thyroid, cricoid, and posterior (arytenoid, corniculate, and cuneiform) cartilage and the epiglottis.

The cricoid cartilage is a complete ring that articulates with the thyroid and arytenoid cartilage.
The arytenoid cartilage sits on the postero-lateral border of the cricoid, from where it can be dislocated during airway management.
The laryngeal inlet is bounded by the epiglottis, aryepiglottic folds, posterior cartilage, and interarytenoid notch.

The vocal cords run between the vocal processes of the arytenoid cartilage and the posterior surface of the thyroid cartilage.
The lower end of the leaf-shaped epiglottis is attached to the middle of the posterior surface of the thyroid cartilage.
The anterior surface is connected to the hyoid bone by the hyo-epiglottic ligament and to the tongue by the median glosso-epiglottic fold.

The valleculae (often called vallecula) are depressions between the median and lateral glossoepiglottic folds that connect the lateral edges of the epiglottis to the base of the tongue.
The Macintosh technique of laryngoscopy involves insertion of the tip of the laryngoscope into the vallecula, where it tensions the hyo-epiglottic ligament to achieve indirect elevation of the epiglottis.




The pharynx is a fibromuscular tube that extends from the base of the skull to the lower border of the cricoid cartilage.
It joins the nasal and oral cavities above with the larynx and esophagus below.
Both the pharynx and esophagus can be perforated by blind attempts at tracheal intubation

The examination described by El-Ganzouri and colleagues
assessment of mouth opening, prognathic ability, head extension, thyromental distance, and Mallampati test has been used with
minor modification by others.

The ability to achieve good mouth opening is important for many airway procedures.
Initial mouth opening is achieved by rotation within the temporomandibular joint (TMJ) and subsequent opening by sliding of the condyles of the mandible within the TMJ.
Also known as protrusion, translocation, or subluxation.

17
DIFFICULT TO BAG (MOANS)
Mask Seal Obesity or Obstruction Age > 55 No Teeth Stiff

18
AIRWAY ASSESSMENT Global airway assessment. (history & physical examination, airway compromising conditions)
Regional anatomical assessment (Teeth, oral cavity, mandibular space and neck)
LEMON Airway assessment method.
Radiological assessment. ( Skeletal films, fluoroscopy, USG, CT/MRI )
Wilson’s rule for predicting difficult intubation.
Quick assessment of airway “the rule of 1-2-3”


Teeth inter-incisor distance
“ It is the distance between the upper & lower incisors when the mouth is widely open”
Normal 4.6 cm or moreLess than 3.8 cm predicts difficult airway.

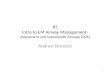
The Mallampati classification is performed by having patients open the mouth widely and protruding the tongue completely forward. A tongue depressor is not used.
In class I, the soft palate, fauces, entire uvula, and pillars are visualized;
in class II, the soft palate, fauces, and a portion of the uvula;
in class III, the soft palate and base of the uvula; and
in class IV, the hard palate only.


Relates to tongue size to pharyngeal size.
Performed with patient in a sitting position, head neutral, mouth open wide and tongue protruding to the maximum.

The evaluation should also document the status of teeth,
range of motion of the neck, neck circumference (increasing size predicts difficulty with laryngoscopy),
thyromental distance, body habitus, and pertinent deformities.

Ventilation via mask requires the ability to achieve a seal between the mask and face and to overcome upper airway obstruction.
Limited mandibular protrusion, abnormal neck anatomy, sleep apnea, snoring, and obesity are independent predictors of moderate or severe difficulty with mask ventilation.
Snoring and a thyromental distance of less than 6 cm are independent predictors of severe difficulty

Airway assessment cannot detect some serious problems, including
asymptomatic lesions in the vicinity of the larynx,
skeletal factors, and some varieties of TMJ dysfunction.

The problem with airway assessment is that the risk of difficulty is overestimated and not all cases of difficult airway management can be predicted.
Airway evaluation gives some indication of potential difficulty and should always be performed.

The anesthesiologist must then make a judgment of whether direct laryngoscopy, mask ventilation, and percutaneous rescue are likely to be successful.
The limitations of airway assessment mean that preparation of an airway strategy for the management of unanticipated difficulty is the ultimate key to safe practice.

Because of the relatively high incidence of dental injuries during anesthesia, thorough documentation of preexisting tooth abnormalities is useful.

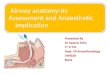
CORMACK MAC LAHANE GRADING

Grade 1: Full aperture visible Grade 2: Lower part of cords visible Grade 3: Only epiglottis visible Grade 4: Epiglottis not visible

COMPONENTS OF THE AIRWAY EXAMINATION Length of the upper incisors Condition of the teeth Relationship of the upper (maxillary)
incisors to the lower (mandibular) incisors
Ability to protrude or advance the lower (mandibular) incisors in front of the upper (maxillary) incisors
Inter-incisor or intergum (if edentulous) distance
Tongue size

Visibility of the uvula Presence of heavy facial hair Compliance of the mandibular space Thyromental distance with the head in
maximum extension Length of the neck Thickness or circumference of the neck
Range of motion of the head and neck

Creation of a surgical airway (necessary for the management of a “cannot intubate, cannot ventilate” situation) depends on percutaneous access to the cricothyroid membrane.
In some patients the cricothyroid membrane cannot be identified or lies behind the sternum, and creation of a percutaneous airway will not be possible.
In such patients who have indications that laryngoscopy or mask ventilation will be difficult, the safest strategy is to secure the airway while the patient is conscious.

35
NECK MOBILITY Atlanto –occipital joint extension normal: 35
degrees.
Any reduction in extension is expressed as grades’
Grade I >35 degree Grade II 22 – 34 degree Grade III 12 – 21 degree Grade IV <12 degree
LEMONS

MEASUREMENT OF ATLANTO -OCCIPITAL ANGLE

37
THYROMENTAL DISTANCE(MANDIBULAR SPACE) Distance from the mentum to the thyroid notch.
Ideally done with the neck fully extended. Can be done in-line
Gives an indication of the space anterior to the larynx ( the mandibular space )
Normal 6 cms or 3 Finger breadth.
Helps determine how readily the laryngeal axis will fall in line with the pharyngeal axis.
LEMONS

38
Sterno -mental distance.( >12 cms)
“In 1948 Savva estimated the distance from the suprasternal notch to the mentum and investigated
the possible correlation with mallampatti class, jaw protrusion, Interincisor gap & Thyromental Distance.”
Measured with the head fully extended on the neck with the mouth closed.
A value <12 cms is found to predicts the difficultintubation.

39
DIFFICULT LARYNGOSCOPY & INTUBATION
LEMONSLook ExternallyEvaluate 3-3-2 Mallampati ScoreObstructionNeck MobilityScene and Situation

40
LOOK EXTERNALLY
Beards or facial hair Short, fat neck Morbidly obese patients Facial or neck trauma Broken teeth (can lacerate balloons) Dentures (should be removed) Large teeth Protruding tongue A narrow or abnormally shaped face
LEMONS

41
EVALUATE 3-3-2 Mouth Opens at least 3 finger widths.
Three finger widths thyromental distance.
Two finger widths mandibulohyoid distance.
LEMONS

42
MOUTH OPENS AT LEAST 3 FINGERS WIDTH?
LEMONS

43
THYROMENTAL DISTANCE-3 FINGERS?
LEMONS

44
MANDIBULOHYOID DISTANCE- 2 FINGERS? Measured from the
mentum to the top of the hyoid bone.
The epiglottis arises from the thyroid and remains dorsal to the hyoid bone.
Therefore, the position of the hyoid bone marks the entrance to the larynx.
LEMONS

45
MANDIBULOHYOID DISTANCE
LEMONS

46
MANDIBULOHYOID DISTANCE
When the position of the hyoid bone is caudal or relatively caudal, a large portion of the tongue is situated in the hypopharynx instead of the mouth.
During laryngoscopy, this large hypo pharyngeal tongue mass further compromises the compliance needed for its displacement
LEMONS

47
MANDIBULOHYOID DISTANCE Patients who have a
longer mandibulohyoid distance, greater then 2 finger widths, tend to be more difficult to intubate.
A more caudal hyoid bone thus indicates a relatively caudal larynx.
LEMONS

48
Laryngoscopy or intubation may be more difficult in the presence of an obstructionAnatomyTraumaForeign body obstructionEdema (burns)
LEMONSOBSTRUCTION

49
SCENE AND SITUATION (SEE)
Scene safety Environment
Do you have a reasonable chance to get the tube?Space, positioning, access
EgressWill you be able to ventilate during egress?A respiratory rate of 4 is better than a rate of 0!Enough meds for a long extrication?
LEMONS

50
WILSON’S RULE FOR DIFFICULT INTUBATION.
Risk factor. Level score.
Weight. 90kg 090-110kg 1 >110kg 2
Head & neck above 90 0Movement: about 90 1
below 90 2
Jaw movement IG>5cm 0IG<5cm 1IG<5cm 2
Receding mandible normal 0moderate 1severe 2
Buck teeth normal 0 moderate 1
severe 2

51
RADIOLOGICAL AIRWAY ASSESSMENT.
Subtle bony abnormalities of mandible, maxilla & cervical spine difficulty in visualization of larynx
White & kander made several measurements on the radiographs lateral, PA & Submento-vertical view.
1. Posterior depth of the mandible 2. Effective mandibular length. 3. Gap between the occiput & spine of the
first cervical vertebra

52
Posterior depth of the mandible.The distance between the alveolus immediately
behind the 3rd molar tooth to the lower border of the mandible
Effective mandibular lengthThe distance from the tip of the lower incisors to the
tempero-mandibular joint
“ direct laryngoscopy was difficult when the effective mandibular length was less than 3.6 times the posterior depth of the mandible”

53

54
SOME PREDICTORS OF A DIFFICULT AIRWAY
C-spine immobilized trauma patient
Protruding tongue Short, thick neck Prominent upper
incisors (“buckteeth”) Receding mandible High, arched palate Beard or facial hair
Dentures Limited jaw opening Limited cervical mobility Upper airway conditions Face, neck, or oral trauma Laryngeal trauma Airway edema or
obstruction Morbidly obese

55
ADDITIONAL PREDICTORS:MEDICAL HISTORY
Joint disease Acromegaly Thyroid or major neck
surgeries Tumors, known abnormal
structures Genetic anomalies Epiglottitis
Previous problems in surgery
Diabetes Pregnancy Obesity Pain issues

DIFFICULT AIRWAY ALGORITHM Assess the likelihood and clinical impact
of basic management problems. A. Difficult ventilation. B. Difficult intubation. C. Difficulty with patient co operation or
consent. D. Difficult Tracheostomy

2. Actively Pursue opportunities to deliver supplemental oxygen throughout the process of difficult airway management.
3. Consider the relative merits and feasibility of basic management choices.
A. Awake intubation Vs. Intubation attempts after induction of GA.
B. Non invasive technique for initial approach to intubation Vs. invasive technique for initial approach to intubation.
C. Preservation of spontaneous ventilation Vs. Ablation of Spontaneous Ventilation.

4. DEVELOP PRIMARY AND ALTERNATIVE STRATEGIES.



REFERENCES: Millers Anesthesia- 7th Edition. Morgan’s Clinical Anesthesiology- 4th
Edition. Indian Journal of Anesthesiology- 2005
49(4) Airway assessment- Predictors of
difficult airway.

THANK YOU