Embed Size (px)
Citation preview

Dr. Manish Raj MD,DA,FISP,FPM Minimally Invasive Spine & Pain consultant
Fellow of Interventional spine & pain(Pci-Mumbai) Fellow of Pain manganement (FPM-Aesculap Germany)
Member- North american spine society(NASS) -Society of minimally invasive spine surgery(SMISS)

• About 85% of Indians experience back trouble by age 50.
• Back problems are the most frequent cause of activity limitations in working-age adults
• In the long run, surgery, chiropractic care, etc., are considered no more effective than no treatment in reducing low back pain…so, prevention is key!
Back facts in general…

Overview Introduction
Anatomy
Causes of LBP
Prevention
Recent Advances in Treatment

BACK & NECK PAIN One of the most common chronic conditions in India
Frequency in men & women are equal
4 out of 5 Indians will experience LBP or Neck Pain
Acute: 6 weeks
Chronic: > 6 weeks

Anatomy
Spine: 33 vertebrae
7 cervical (neck)
12 thoracic
5 lumbar
5 sacral (fused)
4 coccygeal (tailbone)
INTERVERTEBRAL DISC
Fibrocartilage
Functions:
Absorb shock
Allows increased spinal range of motion in flexion/ extension

NERVES Nerves come out of holes between vertebrae

MUSCLES & Connective Tissues Spine is supported by bones, muscles and connective
tissues
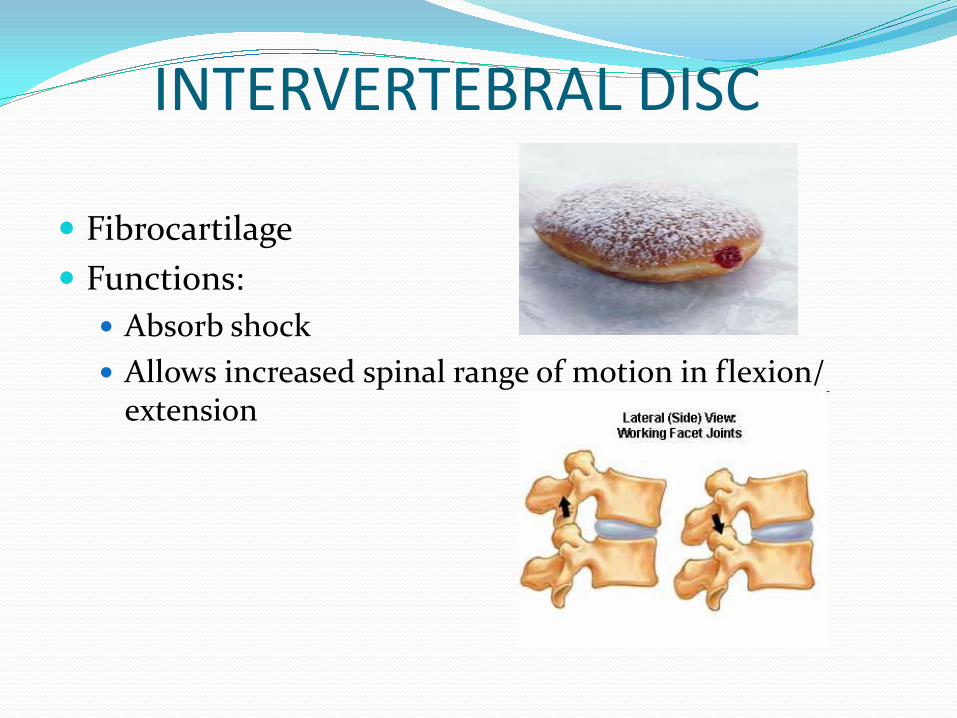
Injury to any structures previously
mentioned in the Spine
region
How do you get low back pain?

• Poor body mechanics
• Stressful living & work habits
• General physical fitness decline
• Loss of flexibility
• Loss of strength
Leading Causes of Back Problems

General joint stiffness
Acute strains and sprains
Muscle guarding or spasm
Disc bulge herniation
Degenerative disk disease
Osteoarthritis
Common Back Disorders
A other ause of a k pro le s…
accidents
It is also possible to injure your back due to accidents.

Back Strain/ Sprain
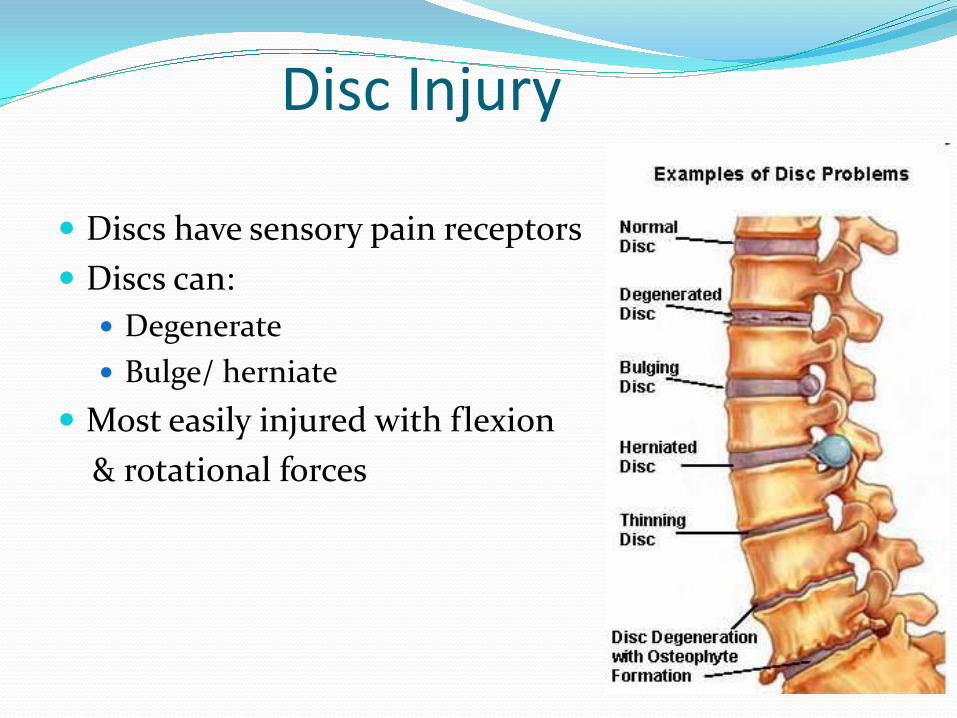
Disc Injury
Discs have sensory pain receptors
Discs can:
Degenerate
Bulge/ herniate
Most easily injured with flexion
& rotational forces
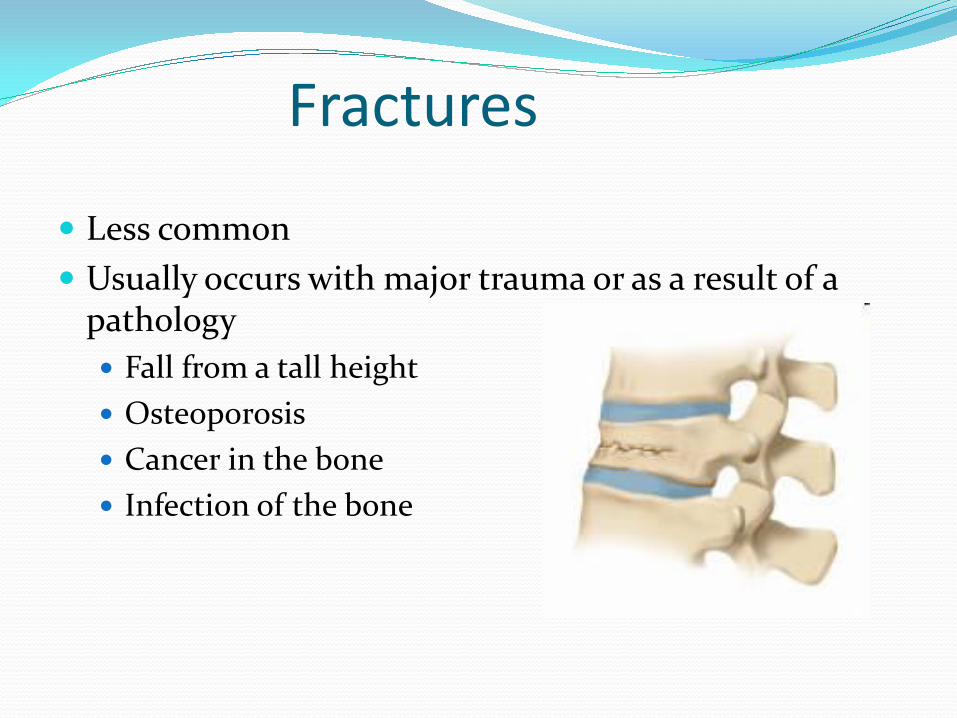
Fractures
Less common
Usually occurs with major trauma or as a result of a pathology
Fall from a tall height
Osteoporosis
Cancer in the bone
Infection of the bone

Risk Factors
Pregnancy
Poor physical conditioning
Poor movement techniques
Poor posture
Occupation
Previous back injuries
Others – spinal disorders (e.g. scoliosis, osteoporosis, spondylosis)

Causes - Summary
Any injury to supporting & surrounding structures Muscles
Ligaments
Joint
Bones
Intervertebral discs
Nerves

Maintain good physical condition Ideal weight, maintain good muscle strength,
endurance, and cardiovascular endurance
Proper diet/ nutrition
Proper lifting techniques
Proper posture
Avoid smoking Decreases blood flow
Maintain good core strength
Prevention

Prevention: Posture

Prevention: Posture Sitting posture

Prevention: Posture

Prevention: Proper Lifting

Prevention: Proper Lifting

Disc Herniation

Treatment options for Slip disc -Selective root sleeve transforaminal Epidural steroid
-percutaneous mechanical decompression:
-Decompressor STRYKER
-Nucleotomy
-Hydrodiscectomy
-NUCLEOPLASTY
-Laser Discectomy etc
-ozone discectomy
-IDET(intradiscal electrothermal coagulation)
-Disctrode(Intradiscal radiofrequency)
-Biacuplasty
-ENDOSCOPIC DISCECTOMY
-MIS fusion(percutaneous TLIF)
- Open Surgery(Microdiscectomy,laminectomy,fusion)

TFESI (EPIDURAL INJECTION)

OZONE DISCECTOMY

HYDRODISCECTOMY

DECOMPRESSOR DISCECTOMY
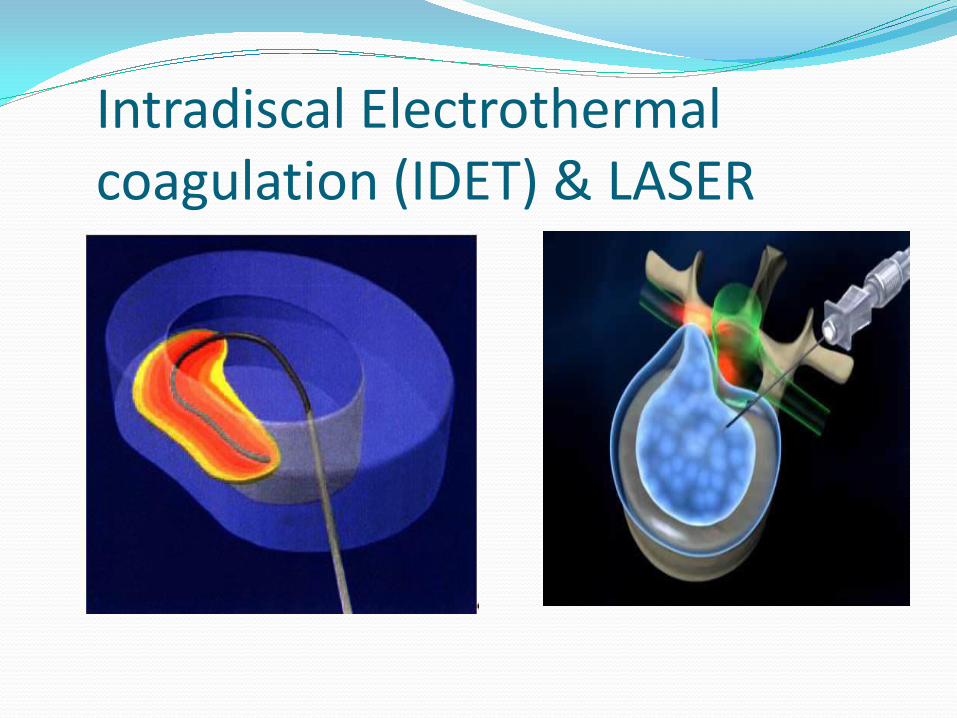
Intradiscal Electrothermal
coagulation (IDET) & LASER

NUCLEOPLASTY

Optimal Patient Selection
Radicular pattern with or without Axial Pain Leg pain > back pain
MRI evidence of contained disc protrusion
Discography positive, if indicated
Failed selective nerve root block x 1
Failed conservative therapy X 3 months
Axial Back Pain Failed conservative therapy X 3 months
MRI evidence of contained disc protrusion
Discography positive for concordant pain
Failed diagnostic injections (facet, nerve, epidural etc)
Disc height > 75%

Exclusion Criteria 50 % loss of disc height
Extruded or sequestered disc
Spinal fracture or tumour
Moderate to severe spinal stenosis
Complete annular disruption
Degenerative instability
33

Clinical Outcomes After Lumbar Discectomy for Sciatica: The Effects of Fragment Type and Annular Competence EJ Carragee et al., Stanford University , The Journal of Bone and Joint Surgery. Jan 2003
Are Nucleoplasty and Microdiscectomy patients the same?
Study of microdiscectomy outcomes based on herniation type
Classified herniations into 4 types
Results: contained herniation with no sub-annular fragment performed poorly with microdiscectomy
Conclusion: The ideal Nucleoplasty patient is not a good candidate for microdiscectomy
34

Radiology terms Oblique View
Kambins triangle

Correct Needle Placement Same approach as discography for needle placement
36

Incorrect Needle Placement 37
Needle entry too far lateral.

Incorrect Needle Placement
38
Needle entry too far lateral and shallow.

Lumbar Nucleoplasty Technique 1. Using fluoroscopy, introduce
the needle to the nucleus/annulus junction of the disk (Confirm position using fluoroscopy).
39

Lumbar Nucleoplasty Technique 2. Insert the wand through
the needle, and advance the Wand until the Reference Mark is at the needle hub.
40

Lumbar Nucleoplasty Technique
3. Using blunt dissection, advance the tip of the DLR into the nucleus, and STOP when the distal annulus is reached. This determines the Distal channel limit.
41

Lumbar Nucleoplasty Technique 4. Position Depth Gauge at
the needle hub It will reference the Distal channel limit within the nucleus (this should be confirmed using fluoroscopy).
42

Lumbar Nucleoplasty Technique - Final Result
Create additional channels at the 4, 6, 8, and o’clock positions.
Approximately 1/2 cc of tissue removed causing decompression.
43

The Procedure-Cervical Nplasty
The surgeon uses the fingers to detect the vertebral space holding the SCM
muscle laterally and the trachea medially.
44
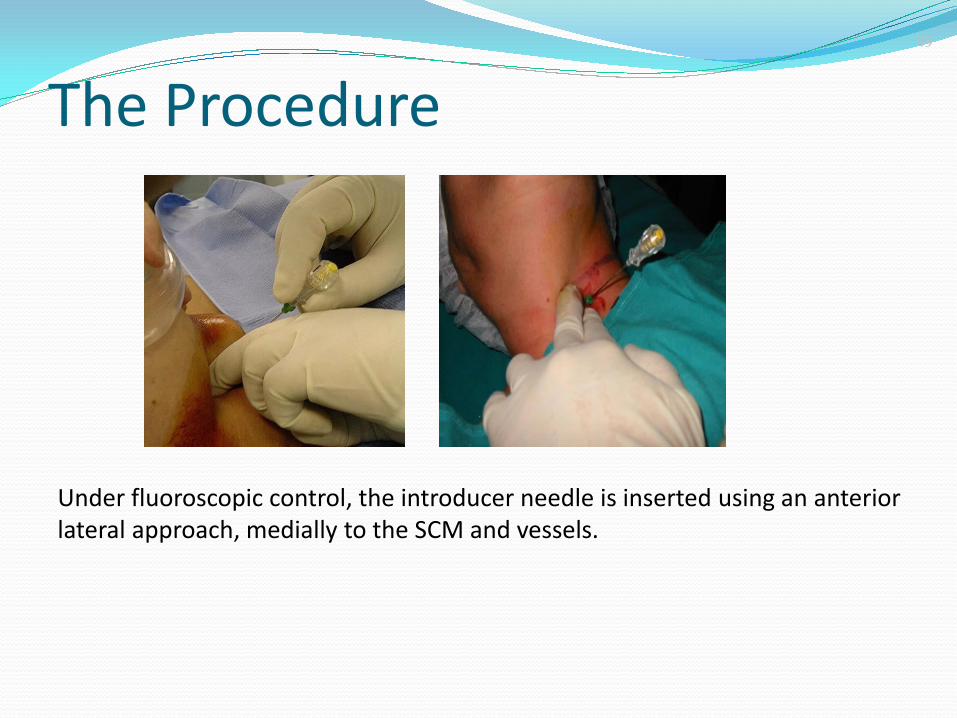
Under fluoroscopic control, the introducer needle is inserted using an anterior
lateral approach, medially to the SCM and vessels.
The Procedure
45

Needle Placement Check needle placement in A/P projection
Needle should be in line with the midline (spinous process)
A/P Lateral
46

Cervical Nucleoplasty Technique
Position needle tip in the posterior 1/3 of the nucleus Anterior-lateral approach
Fluoroscopic guidance
If desired, move the green marker down to skin level.
Unscrew and remove the stylet
Insert the Perc DC SpineWand Only as far as tip remains within end of needle
Do not allow device to protrude from needle
47

Cervical Nucleoplasty Technique
Once the device is inserted, withdraw the needle from over the tip of the device monitor deployment of device
beyond end of needle
Lock Perc DC into Needle Hub
Confirm with fluoroscopy
48

Cervical Nucleoplasty Technique In ablation mode, rotate device
through 360o for approximately 2 - 3 seconds
Withdraw device 1-2 mm and repeat to make a series of 2-3 voids.
Never maneuver or advance the needle with the device inserted
Unlock SpineWand from needle hub and withdraw into introducer needle before removing.
49
3 2 1

3 2 1
The Procedure Ablation mode is performed for three cycles in
withdrawal, rotating the wand 180 in each cycle (8 seconds ablation each)
50

The Procedure 51
The wand is unscrewed from the luer lock and removed inside the introducer
needle

ENDOSCOPIC DISCECTOMY
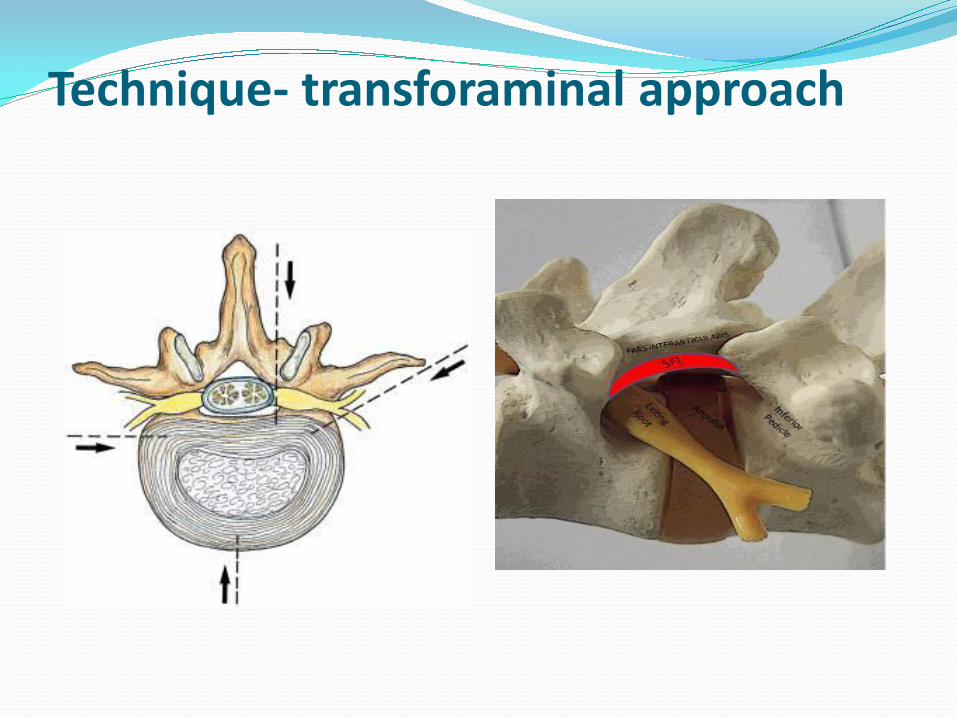
Technique- transforaminal approach

Surgical Approach



SPINE FUSION (MIS)

SPINAL CORD STIMULATOR

Vertebral compression fracture

VERTEBROPLASTY & KYPHOPLASTYPLASTY

VERTEBROPLASTY

Vertebral augmentation-KIVA

Failed Back surgery syndrome (FBSS)
Percutaneous fluoroscopic epidural adhesiolysis.
RF Facet joint denervation & DRG lesioning.
Spinal cord stimulation
Intrathecal drug delivery systems.

ADVANCEMENT ??????????????
Percutaneous Decompressor Discectomy
Hydrocision Discectomy/ Laser Discectomy
Endoscopic Discectomy
Bicuplasty/Ozone Discectomy
Disc Nucleoplasty / Automated Nucleotomy
Neuroplasty/Adhesinolysis
Vertebroplasty/Kyphoplasty
Intradiscal eletrothermal coagulation(IDET)
Spinal Cord Stimulator
Neurotomy/Radiofrequency Ablation
Provocative Discography
Lumbar & cervical Transforaminal epid.inj
Cervical & Lumbar Facet Joint injection/Block
Intrathecal Pump
Mimimal invasive lumbar discectomy(MILD)
MIS Fusion/ TLIF

QUESTIONS?

Dr Manish Raj MD,DA(Gold medal),FISP,FPM Minimally invasive spine & pain Consultant
BENSUPS Cygnus Superspeciality Hospital,Dwarka
CYGNUS Orthocare Hospital ,Safdarjung Development Area
Director-Spinomax pain & spine clinic,Safdarjung Enclave
www.spinomax.com , Email – [email protected]




















![Back Talk - Back Pain Rescue[1]](https://img.pdfslide.us/doc/110x75/577d35821a28ab3a6b90a19c/back-talk-back-pain-rescue1.jpg)