Embed Size (px)
Citation preview

TM
Clinical Practice Guideline forthe Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents
Mark L. Wolraich, MD, FAAPCMRI/Shaun Walters Professor of PediatricsUniversity of Oklahoma Health Sciences Center
TM
Prepared for your next patient.

TM
Disclaimers Statements and opinions expressed are those of the authors and not
necessarily those of the American Academy of Pediatrics.
Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter has complete and independent control over the planning and content of the presentation, and is not receiving any compensation from Mead Johnson for this presentation. The presenter’s comments and opinions are not necessarily those of Mead Johnson. In the event that the presentation contains statements about uses of drugs that are not within the drugs' approved indications, Mead Johnson does not promote the use of any drug for indications outside the FDA-approved product label.

TM
Disclosures Consultant with: Lilly Shire Shinogi NextWave

TM
Learning Objectives Participants will be able to report on the major
changes in the revised attention-deficit/hyperactivity disorder (ADHD) guideline.
Participants will be able to obtain and use appropriate behavior rating scales.
Participants will be able to describe the importance of considering ADHD as a chronic condition.
Participants will be aware of the variations in treatment recommended for preschool age children and adolescents.

TM

TM
ADHD Guideline Recommendations1. The primary care clinician should initiate an
evaluation for ADHD for any child 4 through 18 years of age who presents with academic or behavioral problems and symptoms of inattention, hyperactivity, or impulsivity. B/strong recommendation

TM
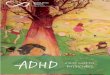
Prevalence of ADHD in Children
Centers for Disease Control and Prevention/National Health Care Surveys, 1997–2006

TM
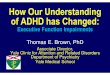
Prevalence and Medication Use
ADHD prev
ADHDon meds
ADHD noton meds
ADHD diagnosedon meds

TM
ADHD Guideline Recommendations2. To make a diagnosis of ADHD, the primary care
clinician should determine that Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria have been met (including documentation of impairment in more than 1 major setting) with information obtained primarily from parents/guardians, teachers, and other school and mental health clinicians involved in the child’s care. The primary care clinician should also rule out any alternative cause. B/strong recommendation

TM
Evaluation Identify core symptoms. Assess impairment. Identify possible underlying or alternative causes. Identify co-occurring (co-morbid) conditions.

TM
DSM-IV Core Symptoms of Inattention
*Must have 6 or more symptoms for at least 6 months to a degree that is maladaptive and inconsistent with developmental level.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth edition. Arlington, VA: American Psychiatric Association; 2000
Manifestations of the following symptoms must occur often:*
Avoids/dislikes tasks requiring sustained mental effort Can’t organize Loses important items Easily distractible Forgetful in daily activities
Inattention Careless Difficulty sustaining attention in activity Doesn’t listen No follow-through

TM
DSM-IV Core Symptoms of Hyperactivity-Impulsivity
Impulsivity Blurts out answers Can’t wait turn Intrudes/interrupts others
*Must have 6 or more symptoms for at least 6 months to a degree that is maladaptive and inconsistent with developmental level.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth edition. Arlington, VA: American Psychiatric Association; 2000
Manifestations of the following symptoms must occur often:*
Hyperactivity Squirms and fidgets Can’t stay seated Runs/climbs excessively Can’t play/work quietly “On the go”/“driven by a motor” Talks excessively

TM
Assess Function Academic performance Peer relations Sibling relations Parent relations Community activities

TM
Clinical Global Impression Scale

TM
DSM-IV ADHD Diagnostic Criteria List of core symptoms must be present for past 6
months. Some symptoms need to be present before 7 years
of age. Some impairment from symptoms must be present
in 2 or more settings (eg, school and home). Significant impairment (social, academic, or
occupational) must be present. Other mental disorders need to be excluded as the
cause of the core symptoms.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth edition. Arlington, VA: American Psychiatric Association; 2000

TM
Inattention or Hyperactive/Impulsive Problems Children who do not meet the criteria of ADHD still may
have some symptoms of inattention and/or hyperactivity/impulsivity fitting the category in the Diagnostic and Statistical Manual for Primary Care (DSM-PC) of inattention and/or hyperactivity/impulsivity. Use of the chronic illness model and behavioral interventions are appropriate, but medications are not.
American Academy of Pediatrics. In: Wolraich ML, Felice ME, Drotar D. The Classification of Child and Adolescent Mental Diagnosis in Primary Care. Elk Grove Village, IL: American Academy of Pediatrics; 1996

TM
Preschool Age Diagnostic Issues The same criteria are pertinent for preschool age
children, but it is more difficult to find qualified observers of these children.
Enroll the child in a program and/or have the parents participate in a parent training program.
Greenhill L, Kollins S, Abikoff H, et al. Efficacy and safety of immediate-release methylphenidate treatment for preschoolers with ADHD. J Am Acad Child Adolesc Psychiatry. 2006;45(11):1284–1293

TM
Adolescent Diagnostic Issues It is much more difficult to get adequate observers,
as both parents and teachers have less opportunity to observe.
The risk of substance abuse is higher and must be ruled out before a diagnosis can be made.
The occurrence of co-morbid conditions, particularly anxiety or depression, is more frequent.
Wolraich ML, Wibbelsman CJ, Brown TE, et al. Attention-deficit/hyperactivity disorder in adolescents: a review of the diagnosis, treatment and clinical implications. Pediatrics. 2005;115:1734–1746

TM
Diagnostic Process Use of ADHD specific rating scales is a clinical
option in the evaluation of ADHD. Use of broad-band rating scales is not
recommended in diagnosing ADHD although they may be useful for evaluating for coexisting conditions.

TM

TM
Websites for the Vanderbilt Scales
The University of Oklahoma College of Medicine http://www.idi.ouhsc.edu/body.cfm?id=4779
American Academy of Pediatrics - Pediatric Care Onlinehttps://www.pediatriccareonline.org/pco/ub/index/Forms-Tools/Keywords/N/NICHQ

TM
ADHD Guideline Recommendations3. Evaluation of a child for ADHD should include
assessment for coexisting conditions, including emotional, developmental, and physical. B/strong recommendation

TM
Co-morbidity:Conditions Commonly Co-occurring with ADHD Disruptive behavior disorders
– Oppositional defiant disorder– Conduct disorder
Depressive disorders Anxiety disorders Cognitive disorders
– Learning disabilities– Language disorders
Motor disorders– Developmental coordination disorder– Tic disorders (Tourette's)

TM
ADHD Guideline Recommendations4. The primary care clinician should establish a
treatment program that recognizes ADHD as a chronic condition and a child with ADHD as a child/adolescent with special health care needs who needs a medical home. B/strong recommendation

TM
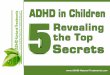
Methylphenidate therapy bout length by patient age
Miller AR, Lalonde CE, McGrail KM. Children’s persistence with methylphenidate therapy: a population-based study. Can J Psychiatry. 2004;49(11):761–768

TM
Treating ADHD as a Chronic Condition Educate parents and patients about ADHD. Develop a partnership with the family. Develop a management plan with specific
targeted goals. Include the teachers if at all possible. Requires ongoing monitoring and anticipation
of developmental changes.

TM
ADHD Guideline Recommendations5. Recommendations for treatment of children and
youth with ADHD vary depending on the patient’s age:

TM
Preschool-aged Children(4–5 Years of Age)A. Prescribe evidence-based parent- and/or
teacher-administered behavior therapy as the first line of treatment. A/strong recommendation
and
May prescribe methylphenidate if the behavior interventions do not provide significant improvement and there is moderate-to-severe continuing disturbance in the child’s function. B/recommendation

TM
Preschool Age Treatment Issues While stimulant medications are appropriate for
preschool age children based on recent research, given that a third of the children in a multi-site study improved on behavioral interventions alone, it is more appropriate to initiate a parent training program first before utilizing medication and only treat the more severe cases.
Preschool age children frequently have a slower metabolism of the medications and can start at a lower dose and titrated at a slower rate.
Greenhill L, Kollins S, Abikoff H, et al. Efficacy and safety of immediate-release methylphenidate treatment for preschoolers with ADHD. J Am Acad Child Adolesc Psychiatry. 2006;45(11):1284–1293

TM
Elementary School-aged Children(6–11 Years of Age)B. Prescribe FDA-approved medications for ADHD.
A/strong recommendation
and/or
Evidence-based parent- and/or teacher-administered behavior therapy as treatment for ADHD.
Preferably both. B/recommendation

TM
Adolescents (12–18 Years of Age)C. Prescribe FDA-approved medications for ADHD
with the assent of the adolescent. A/strong recommendation
and
May prescribe behavior therapy as treatment for ADHD. C/recommendation
Preferably both.

TM
Non-Stimulants Atomoxetine is a highly specific norepinephrine
reuptake inhibitor.
Extended release guanfacine and clonidine are alpha 2 adrenergic agents.

TM
ADHD Guideline Recommendations
6. The primary care clinician should titrate doses of medication for ADHD to achieve maximum benefit with minimum adverse effects. B/strong recommendation

TM
Summary Children from preschool age through adolescent
age can be diagnosed and treated for ADHD. Both medications (stimulants, selective
norepinephrine reuptake inhibitors and alpha adreneric agents) and behavior therapy are effective and safe treatments for ADHD.
Effective treatments require appropriate titration and ongoing monitoring to remain effective.

TM
Caring for Children With ADHDA Resource Toolkit for Clinicians, 2nd Edition
This comprehensive ADHD resource provides a full set of tools for assessment and diagnosis, treatment and medication, monitoring and follow-up, parent education and support, and coding and payment.
Included are more than 40 practice-tested tools—many in English and Spanish—on one convenient CD-ROM. The ADHD toolkit components have been evaluated and refined based on input from the American Academy of Pediatrics Quality Improvement Innovation Network (QuIIN).
For more information or to order visit the AAP bookstore at http://tinyurl.aap.org/pub169531.

TM
Additional ADHD Resources on Pediatric Care Online (www.pediatriccareonline.org) Forms & Tools
https://www.pediatriccareonline.org/pco/ub/index/Forms-Tools/Keywords/A/ADHD
Patient Handoutshttps://www.pediatriccareonline.org/pco/ub/index/Patient_Handouts_AAP/Keywords/A/ADHD
AAP Textbook of Pediatric Carehttps://www.pediatriccareonline.org/pco/ub/index/AAP-Textbook-of-Pediatric-Care/Topics/A
Point-of-Care Quick Referencehttps://www.pediatriccareonline.org/pco/ub/index/Point-of-Care-Quick-Reference/Topics/A

TM
For more information… On this topic and a host of other topics, visit:
www.pediatriccareonline.org
Pediatric Care Online is a convenient electronic resource for immediate expert help with virtually every pediatric clinical information need. Must-have resources are included in a comprehensive reference library and time-saving clinical tools.
• Haven't activated your Pediatric Care Online trial subscription yet?It's quick and easy: simply follow the steps on the back of the cardyou received from your Mead Johnson representative.
• Haven't received your free trial card?Contact your Mead Johnson representative or call 888/363-2362 today.