Embed Size (px)
Citation preview


Case Discussion
ByDr. Muhammad SaifullahPG Trainee, Surgical Unit V.Under Supervision of Assoc. Prof. Dr. Javaid Iqbal

CASE HISTORYMr. X.Y.Z, 42 years old male, resident of
Toba Tek Singh, presented to us with complaint of
» Abdominal Pain 5 days» Vomiting 3 days» Abdominal Distention 3 days» Absolute Constipation 2 days

History Detail…..» The patient was in usual state of
health 5 days back when he developed severe abdominal Pain which was sudden, colicky in nature, non-radiating, non shifting, non-aggravating but relieved by vomiting.

History Detail…..» The patient also had three day history
of non-projectile vomiting, initially bilious but later it became feculent. It was associated with abdominal distension, absolute constipation for 2 days & weight loss. There was also history of fresh bleeding per rectum for 5 months. There was no history of mucous discharge, tenesmus and altered bowel habits.

Systemic inquiry…..» General….. H/O loss of appetite &
significant weight loss during past 4 months.» Cardio-vascular System….. No H/O
shortness of breath, palpitations, chest pain or claudication.
» Respiratory System….. No H/O cough or hemoptysis.
» Urinary System….. No H/O flank pain, hematuria, nocturia or dysuria.

Systemic inquiry…..» Nervous System….. No H/O
weakness, numbness, headache, blackouts, fits or visual loss.
» Locomotor System….. No H/O joint pain, stiffness or restriction of movements.
» Skin….. No H/O rash, itch or colored spots.

Past history…..» Patient is known diabetic for 15 years but
not taking any treatment.» No other significant past medical or surgical
history.
» No family history of bleeding per rectum in first degree relatives, hypertension, diabetes, tuberculosis or ischemic heart disease.
» Both parents alive and healthy.
family history…..

Personal and social history…..» Patient is non-smoker with average socio-
economic status.» No drug or alcohol addiction.

Clinical examination…..An emaciated middle aged man, oriented
in time, space and person, lying on the couch having following vitals
B.P 90/60 Temp 98.6 oF Pulse 112/min R/R 15/min

General physical examination….. »Nails… Pallor +ve, No clubbing,
koilonychias, splinter hemorrhages or cyanosis.
»Fingers… No Osler’s, Heberden’s or Bouchard’s nodes, Joint swelling or deformity.
»Palm… No sweating, palmar erythema or dupuytren’s contracture.

General physical examination….. »Face… No puffiness, proptosis,
jaundice, xanthelasmas or central cyanosis. Poor oro-dental hygeine.
»NECK… No thyroid swelling, engorged neck veins or palpable cervical lymph nodes.

General physical examination…..
» No palpable axillary or inguinal lymph nodes.
» FOOT… No edema, cyanosis or loss of hair.

Abdominal examination…..» Abdomen distended with normal shaped
umbilicus, central in position. Peristalsis not visible. No visible scars, striae or veins. Hernial orifices are intact.
» Abdomen was tense with generalized tenderness. No palpable mass or visceromegaly.
» Abdomen was resonant on percussion with no area of dullness.
» Bowel sounds 8-10 per minute with no audible bruits or succussion splash.

Digital rectal examination…..» Inspection showed no skin tags or perianal
abnormality.» On palpation anal tone was normal with no
palpable hemorrhoids or mass. Finger was stained with blood mixed with stool.

INVESTIGATIONS…..» Hb 9.2 g/dl» ESR 40 mm in 1st hour» TLC 10,400 / mm3
Neutrophils 70% Lymphocytes 26% Eosinophils 2% Monocytes 2%
» Platelets 2,90,000 / mm3

INVESTIGATIONS…..» RBS 330» Urea 41» Creatinine
1.1» Bilirubin
1.0 Conjugated 0.7 Unconjugated
0.3» Alk. Phosphatase 119» sGPT 58
» Serum Sodium 140
» Serum Potassium 4.4» Serum Chloride
100» Serum Bicarbonate 25» HBsAg -
ve» Anti-HCV +ve» PT 14 sec» APTT 34 sec

Radiological examination…..X-Ray Abdomen Erect Film showed
multiple air fluid levels with air shadows visible in large gut.

Resusitation & pre-op preparation…..
»IV fluids.»IV Antibiotics.»Analgesics.»Insulin therapy.»N/G intubation & Foley cathetrization.»Monitoring vitals.

Exploratory laparotomy…..Findings…..
1. A 8 cm growth at the Recto-sigmoid junction about 10 cm from the anal verge.
2. Fully distended small and large bowel.3. No Liver mets.4. No peritoneal seeding.5. No enlarged intra-abdominal lymph
nodes.

Exploratory laparotomy…..Procedure…..
Transverse Colostomy and small & large bowel decompression was done. Biopsy of the recto-sigmoid growth was also taken. As the patient was not vitally stable, so resection of the tumor was not done.
Plan…..To stablize the patient for elective procedure after histopathology report.

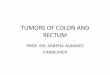
Sigmoidoscopy…..
Histopathology of the recto-sigmoid growth…..
Growth in the rectum totally obstructing the lumen about 12 cm from anal margin. Further colonoscopy not possible. Mucosal biopsy taken and preserved for histopathology.
Signet Ring Cell Adenocarcinoma

PLAN…..Low Anterior Resection of the Recto-
sigmoid growth + TME and subsequent rectal re-construction using double stapling technique.

Low anterior resection, tme &
rectal re-construction using
double stapling technique…..


1. Midline Abdominal Incision

2. Separation and Mobilization of the tumor from the surroundings.

3. Mobilization of sigmoid colon and descending colon upto splenic flexure.

4. Identification of Inferior Mesenteric Artery.

5. Ligation of Inferior Mesenteric Artery.

6. Ligation of posterior rectal pedicle and placing of curved cutter stapler across the rectum and subsequent firing.

7. Application of intestinal clamps and cutting the colon proximal to the tumor

8. Fixation of anvil in the proximal colon end.

9. Insertion of curved circular stapler through the anal verge

10. Fixation of the anvil to the cartridge.

11. Firing of stapler gun and anastomsis of rectum and colon.

12. Doughnuts of gut after resection and stapler anastomosis.


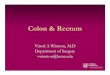
RESECTED TUMOR

Post-operative condition…..
» Recovery….. Uneventfull.» Mobilization of the patient on 3rd day.» Patient discharged on the 7th day.» Follow up.

literature reviewOverall, colorectal cancer is the
second most common malignancy in western countries, with approximately 18 000 patients dying per annum in the UK.

Origin & presentation» Colorectal cancer arises from adenomas
in a stepwise progression in which increasing dysplasia in the adenoma is due to an accumulation of genetic abnormalities.
» Usually, these carcinomas present as an ulcer, but polypoid and infiltrating types are also common.

Dukes’ staging…..» A: limited to the rectal wall: prognosis excellent.» B: extended to the extrarectal tissues, but no
metastasis to the regional lymph nodes: prognosis reasonable.
» C: Secondary deposits in the regional lymph nodes. a) C1. Pararectal lymph nodes alone are involvedb) C2. Nodes accompanying the supplying blood
vessels are implicated up to the point of division. Prognosis is poor.
» D: Widespread metastasis… usually hepatic.


Diagnosis and assessment of rectal cancer…..All patients with suspected CA rectum should undergo:■ Digital rectal examination■ Sigmoidoscopy and biopsy■ Colonoscopy if possible ■ CT colonography or barium enema if
colonoscopy not possible.

Diagnosis and assessment of rectal cancer…..All patients with proven CA rectum require staging by:■ Imaging of the liver and chest, preferably by
CT■ Local pelvic imaging by magnetic resonance
imaging or endoluminal ultrasound.

Management of rectal cancer…..
» Radical excision of the rectum, together with the mesorectum and associated lymph nodes, should be the aim.
» Rectosigmoid tumours and those in the upper third of the rectum are removed by ‘high anterior resection’, in which the rectum and mesorectum are taken to a margin 5 cm distal to the tumour, and a colorectal anastomosis is performed.

Management of rectal cancer…..
» Tumours in the middle and lower thirds of the rectum, complete removal of the rectum and mesorectum is required, i.e. total mesorectal excision (TME). A temporary protecting stoma is usually formed after TME.

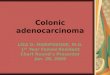
Colo-rectal anastomosisstapling technique





ADVANTAGES OF STAPLER ANASTOMOSIS…..
LIMITATION…..
» Less time consuming.» Minimum risk of leakage.» Low incidence of pelvic sepsis.» Early recovery.
» High cost.