Embed Size (px)
Citation preview
ADEM Management
Dr Roopchand PS
Senior Resident Academic
Department of Neurology
Introduction:• Uncommon monophasic idiopathic
inflammatory demyelinating disease.
• Pleiotropic clinical manifestations.• Usually include encephalopathy.
• Often considered in the differential diagnosis of
a clinicallyisolated (demyelinating) syndrome
(CIS).
• The hallmark of ADEM is its monophasic
course.
• The annual incidence of ADEM is reported to
be 0.4–0.8 per 100,000
• ADEM should be considered when one or more
of the following are present:
• Multifocal, polysymptomatic initial
presentation.
• Age younger than 10 years.
• Signs and symptoms of meningoencephalitis.
• Encephalopathy.
• Bilateral ON.
• Cerebrospnal fluid (CSF) pleocytosis without
oligoclonal bands.
• Magnetic resonance imaging (MRI)-detected
lesions involving structures not typically
affected in MS such as the deep gray matter
or cortex.
• MRI-detected lesions that are large and
exhibit indistinct borders and enhancement
following gadoli nium administration.
• There are no accepted, prospective, or
pathologically verified clinical diagnostic criteria
for ADEM.
• Mikaeloff et al definition:• The occurrence in a previously healthy child of
acute symptoms associating the following at onset:
more than one neurological deficit
(‘‘polysymptomatic’’ onset); change in mental state;
and any combination of alterations seen on MRI,
providing that these included white matter lesions.
• Most restricted definition of ADEM to date• In Pediatric age group.
• 18 % relapsed.
• IPMSSG criteria under evaluation.
• Encephalopathy is the most specific clinical
feature of ADEM.
• Encephalopathy can be seen in fulminant MS.
• Pathophysiology:• Pathological hallmark of ADEM is perivenular
inflammation with limited sleeves of demyelination.
• Acute hemorrhagic leukoencephalitis - additionally
exhibits petechial hemorrhage and venular
necrosis.
• Activation of autoreactive T-cell clones.
Clinical Findings:
• Winter and spring seasonal peaks- suggests viral
etiology.
• Molecular mimicry may produce immune mediated
attack.
• There is a unique immune-mediated CNS process
with a distinct pathophysiology that is
independent of the immune trigger.
• A history of antecedent infection or vaccination may
increase the likelihood of ADEM.
ANTECEDENT INFECTION AND
VACCINATION
• ADEM is more frequent in children.
• Five percent of MS patients present at an age
younger than 16 years.
• Several clinical symptoms of
meningoencephalitis are consistently
associated with ADEM.
• Encephalopathy, seizures, fever, headache,and
meningeal signs.
• More common in pediatric age group and less
common in adults.
• Encephalitis can also cause these symptoms.
• A change in level of consciousness is more
suggestive.
• 23% of 40 patients diagnosed with ADEM
presented with bilateral ON(Dale et al).
• Unilateral ON is associated with MS.
• NMO can present with B/L ON.
• Suspected ADEM patients with B/L ON should
be also evaluated for NMO.
• Typical ADEM is poly symptomatic.
• Restricted forms : ON, Transverse myelitis,
Cerebellitis, Brain stem encephalitis.
Investigations:
• Infection must be excluded by CSF analysis
and culture.
• CSF can be normal or can show lymphocytic
pleocytosis.
• 58% of adult and 29% of pediatric cases with
ADEM have OCBs.
• OCBs resolve in ADEM.
• Persistent OCB points towards MS.
MRI
• Useful in diagnosing ADEM and excluding other conditions.
• MRI will show : multifocal areas of increased T2-weighted (T2W) signal abnormalities in the CNS white matter, with or without gray matter involvement.
• Gadolinium enhancement is less or not seen in ADEM.
• ADEM suggestive: symmetric bilateral disease, relative sparing of the periventricular white matter, or deep gray matter involvement.
• MRI features alone may not be able to
differentiate MS.
• MRI negative ADEM has been reported.
• Single large focal lesion can be compatible with
ADEM..
• Diffusion Tensor imaging and Magnetization
Transfer Imaging can identify abnormalities in
apparently normal appearing white matter.
• ADEM can recurr : 10 to 18%
• Possibility of MS cannot be completely ruled
out.
• Expert opinion: A case is ‘‘recurrent’’ if a
subsequent attack is stereotypical of the first
attack and there is no evidence of involvement
of a different part of the CNS clinically or by
MRI.
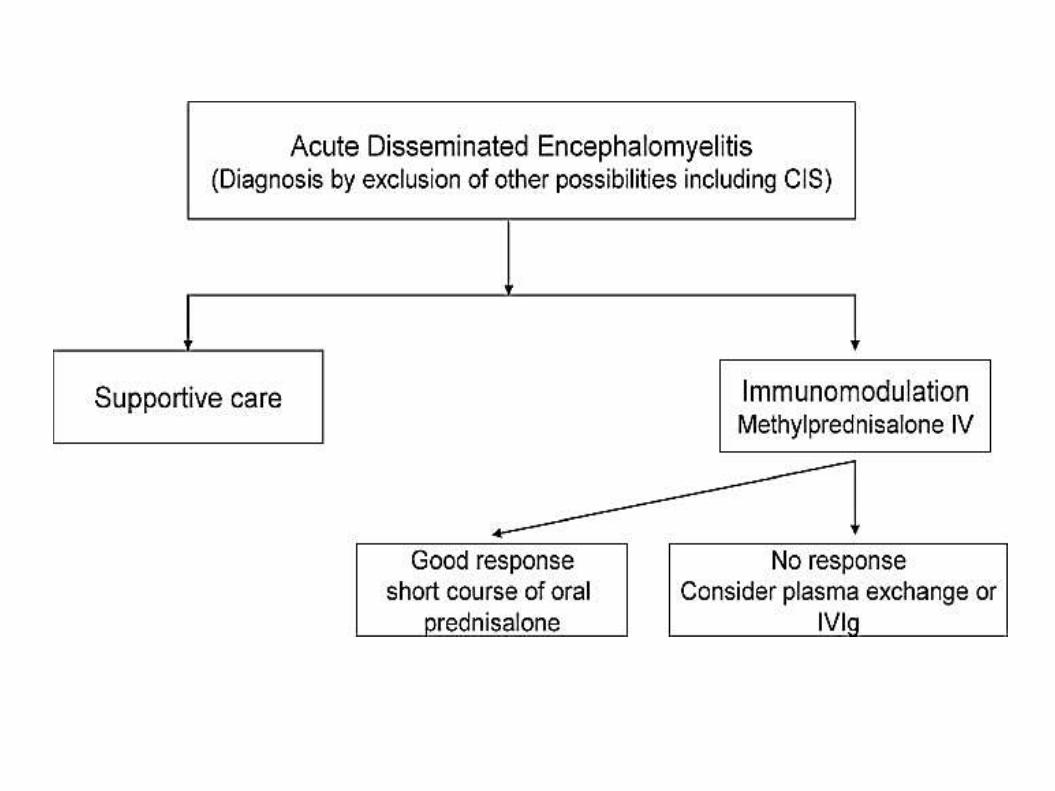
TREATMENT
• Spontaneous recovery can occur.
• Recovery is incomplete in patients who have not
received immunomodulation.
• Use of high-dose steroids, plasma exchange,
and intravenous immunoglobulin are based on
the analogy of pathogenesis of ADEM with that
of MS.
• (1) supportive
• (2) specific—high-dose intravenous methyl
prednisolone, intravenous immunoglobulin
(IVIg), and plasma paresis
• (3) physical and rehabilitation therapy
• Supportive care : management of ventilation,
dyselectrolemias, seizures, maintenance of BP.
Methyl Prednisolone:
• Intravenous methyl prednisolone is the first-line
drug (10–30 mg/kg/day, up to a maximum of 1
g/day) for 3–5 days are being used (Class IV).
• Full recovery has been reported in 50%–80% of
patients.
• Oral corticosteroid treatment is continued with
gradual tapering over 6 weeks to reduce the
risk of relapses.
• Any type of vaccination should be avoided
during the first 6 months following recovery.
PLEx
• Plasma exchange is indicated if corticosteroid
therapy fails.
• There is Class Ib evidence for PE.
• A course of 4–6 PEs have been shown to be
associated with moderate to marked and
sustained improvement.
• Predictors associated with improvement include
male sex, preserved reflexes, and early
initiation of treatment.
IvIg:
• Intravenous immunoglobulin (IVIg) (0.4
gm/kg/day for 5 days) is another option.
• High cost of treatment and the evidence for this
modality of treatment in ADEM is Class IV.
• The improvement is seen within 2–3 days.
• The choice of IvIg vs PLEx depends upon
availability and clinical situation.
• Methyl prednisolone along with IVIg has been
successfully used in patients with atypical
features and could be tried for fulminant,
aggressive, and atypical disease.
Prognosis
• Early studies showed mortality rate of 20% with
a high incidence of neurologic sequelae (
especially postmeasles).
• Prolonged altered mental state was associated
with both mortality and morbidity.
• Multiple or single extensive lesions on MRI
lesions may be associated with disability.
• The prognosis of nonmeasles cases is
favorable and most studies report a full
recovery in 50%–75% of patients.
• Recovery period : 1 to 6 months.