Embed Size (px)
Citation preview

Acute Chest Syndrome
Atul Jindal (MD, DM)Assistant Professor
AIIMS, Raipur

OverviewDefinition
Pathophysiology
Clinical features
Challenges in the diagnosis of ACS
Course & Outcome
Monitoring & Investigations
Treatment of ACS
Chronic complications & Prevention

DefinitionAcute Chest Syndrome (ACS) is defined as an acute illness characterised by fever and/or respiratory symptoms, accompanied by a new pulmonary infiltrate on chest X-ray.

Pathophysiology

EtiologyPulmonary infection - identified in 38% who underwent extensive samplingSeasonal variation - 3 times more common in winterMore common in children<10 years - Viral infection (commonest RSV)Mycoplasma pneumonia (14%), Staph, pneumococcus, H.influenzae

EtiologyFat embolism Microvascular pulmonary infarctionHypoventilation/atelectasis - rib pain, opiate narcosis, post-operative periodAsthma

Clinical FeaturesSecond most common reason for hospitalisation Nearly half of patients present initially with a painful VOC ACS will often develop 24-72 hr after the onset of severe pain

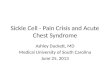
Symptoms & Signs
Data from Vichinsky et al, 1997, 2000
Clinical signs often precede the CXR findings.
Sometimes Chest examination can be normal and hence it is important that the diagnosis is not excluded at this stage.

Challenges in the Diagnosis of ACS
Pulmonary embolism - CT angioFluid overload - Fluid balance chartOpiate narcosis - Monitoring of RR, sedation, and pain scoresAlveolar hypoventilation due to pain

Monitoring and Investigations
High Clinical suspicion + Clinical features = Straight forward diagnosisDiagnosis can be difficult
clinical features may be fewhypoxia is difficult to determine on clinical examination unless severeRadiological signs often lag behind the physical signs

Monitoring and Investigations
Standard monitoring includesAt-least 4 hrly SpO2 (on Air), HR, RR, BPDaily Clinical examinationCBC, CXR, Cr, LFT, Blood C/S, Bld group and cross match, ABG, Sputum C/S and PCR if facilities available

Investigations - CXR

Investigations - CBCAcute fall in Hb conc. or Platelet count are often seen
Decreasing platelet count to <2lac is an independent risk factor for neurological complications and the need for mechanical ventilation
Reticulocyte count - normal count excludes red cell aplasia by parvo B 19.

Investigations - Biochemical tests
RFT & LFT - MODS as a consequence of Systemic fat embolismCRP - monitor progressABG - on room air (if SpO2<94%)
Patients in clear resp. distress or in whom SpO2 falls rapidly to <85% when O2 is removed need escalation of therapy.PaO2 < 82 mm hg (70% of cases)

Investigations - other Investigations
CT - high sensitivity and specificity (84% and 97%)
High radiation dose - not recommendedUse in Pulm. EmbolismSecretory Phospholipase A2 (sPLA2) - levels elevated in ACS

ACS - TreatmentOxygen - titrate to SpO2>95% or within 3% of patient baseline valueIVF - Euvolemic (maintain I/O Chart)Pain relief - Adequate analgesia with frequent review and assessment of pain and sedation scores and cardiorespiratory monitoringIncentive Spirometry & Chest Physiotherapy Antimicrobials - treat for organisms for community acquired pneumonia + atypical organisms

ACS - Treatment
Blood Transfusion -

ACS - TreatmentRespiratory SupportBronchodilators -
Demonstrable reversible airway diseaseHistory s/o asthmaAcute bronchospasm

ACS - Treatment iNO - case reports , No RCT - insufficient evidenceCorticosteroids - Significant variability in their efficacy
Current evidence - mild to moderate ACS - not recommended due to its adverse effectsIf associated with Acute Asthma - Yes

ACS - Chronic complications
Scarring Pulmonary fibrosisChronic Sickle Lung DiseasePoor Lung Function

ACS - PreventionHydroxyurea - Significantly decrease the incidence of ACS in patients with recurrent severe pain and also in unselected children with HbSS.Long term transfusion - has been shown to decrease the incidence of ACS in patients who are being transfused for stroke prevention.Transfusion in preoperative period significantly reduces the incidence of post-operative ACS.Consider HSCT if both fails in preventing ACS episodes.

SCD - Wheeze or Asthma?
Asthma in SCD - 17%-48%
Challenge - Asthma or SCD?
Wheezing: common in SCD and independently associated with morbidity
Cooperative Study - out of 1722 ACS episodes - 11% were wheezing at admission and 26% ultimately had during the course.


SCD - Wheeze or Asthma?
Episode of wheezing producing shortness of breath is associated increased risk of future episode of ACS (IRR 1.7, p=0.04)

SCD - Wheeze or Asthma?
NHLBI guidelines
1) Assess for signs and symptoms of respiratory
problems by history and physical examination;
2) In patients with signs or symptoms of respiratory
problems, further assessment (including pulmonary
function testing) is recommended.

SCD - Wheeze or Asthma?
Knight-Madden and Greenough have termed “Recurrent Wheezing in
Sickle Cell Disease (RWIS)”.
Once we have a better understanding of the mechanisms underlying
airway abnormalities in SCD we can begin to explore the impact of
therapeutic interventions on recurrent wheezing, airway obstruction,
and/or asthma on short and long term SCD outcomes.
This is an important, understudied area that warrants further
investigation in an attempt to reduce morbidity and mortality in these
patients.