Embed Size (px)
Citation preview

ActiveAgeing
Everybody’sInterest,nobody’sresponsibility(?)
BobLaventureChairHEPAEuropeActiveAgeing
WorkingGroupDirectorLaterLifeTraining

Theplan?
• ActiveAgeingasapolicyfocus• Exemplifythroughphysicalactivitypromotion,(generic)andfallsprevention – (specific)
• WithinEUandEngland• Whathelpsandhinderspolicyimplementation
Researchintopractice

Policyinthehandsofpoliticians
“Investtosave”?• Demographicchangewaspredicted• Advantagetoourpoliticalopponents?• Policychangeswithpoliticians- resultinginshort-termism
• Ageingisnowtopical….But
“wearewoefullyunderprepared”forourlongerlivesandourgrowingolderpopulation”.
LordGeoffreyFilkin,(2014)

Policy– whatcounts?Strategy?Guidelines?Frameworks?

Bitof(horrible)history?
• Internationalconsensusandevidence• WHO 1993 - “exercise and lifestyle modification before
drug treatment for mild hypertension” and……..• WHO 1996 “regular physical activity helps to preserve
independent living” and “postpone the age associated declines in balance and co-ordination that are major risk factors for falls”
• US Surgeon General 1996 - “regular physical activity in older adults with chronic illness can potentially reverse loss of mobility”
• American College of Sports Medicine (1998) “Sedentariness appears a far more dangerous condition than physical activity in the very old.”

Describingolderpopulations- (WHO1996)
PhysicallyFit PhysicallyUnfit
PhysicallyUnfitand
FrailHealthy Group1
Unhealthyindependent
Group2
Unhealthydependent
Group3
(WHO 1996 Heidelberg Guidelines on physical activity (60+)

WHOPolicyFocus– ActiveAgeing
Activeageingistheprocessofoptimizingopportunitiesforhealth,participationandsecurityinordertoenhancequalityoflifeaspeopleage.
(WHO2002)

ButActiveAgeing….allthingstoallpeople?
• ActiveAgeing(WHO)– Health– Participation– Security
• Physicalactivity(PHE)– Activity– Moving– Exercise– Sportandrecreation
• Health– Physical– Psychological– Cognitive
• HealthyAgeing– developingand
maintainingthefunctionalabilitythatenableswell-beinginolderage
• Successfulageing– Participating– Volunteering– Contributingtosociety
• Well-being– SCIE– 5waysto…NEF– ICAA….9Pillars

Commentary– supportingpolicy?Physicalactivityandolder
people(65+)• Multipleneeds,target
populations,outcomes• Multipleservices/players• Multipleactivitymodes• (Little)agreementon
effectiveinterventions• Governmentpolicy
flip/flopping?• Leadershipchallenging
Fallsprevention• Strongevidenceofneed
andtargetpopulations• Clarityofevidencebased
interventions• Authoritativeguidance
(NICE,AGSandBGS)• (Sustained?)service
pathways/models• NHSattheforefront

1.EUActiveAgeingPolicyframeworks• EuropeanCharteronCounteractingObesity(2006)
– TheEuropeanFoodandNutritionActionPlan2015-2020– Stepstohealth:aframeworkforactionintheWHOEuropeanRegion'.
(2007)• ContentAnalysisof27EUNationalPolicyDocuments -
Only5includedreferencetoolderpeople65+Daugbjerg etal( 2009),
• ParmaDeclarationonEnvironmentandHealth adoptedbyWHOEuropeanMemberStates- importanceofprovidingsafeenvironmentstoenablephysicalactivity(2010)
• ActiveAgeing(Europe)nowwithintheWHOGlobalactionplanforthepreventionandcontrolofnon-communicablediseases2013–2020
• WHO/EuropecollaborateswithHEPAEurope(EuropeannetworkforthepromotionofHealth-EnhancingPhysicalActivity?)

Priorityarea4– Promotingphysicalactivityamongolderpeople.
• PhysicalactivitystrategyfortheWHOEuropeanRegion2016–2025HEPAActiveAgeingWorkingGroup
• Guidingprinciplesandobjectives• Objective4.1– Improvethequality
ofadviceonphysicalactivitybyhealthprofessionalstoolderpeople
• Objective4.2– Provideinfrastructureandappropriateenvironmentsforphysicalactivityamongolderpeople
• Objective4.3– Involveolderpeopleinsocialphysicalactivity
© Health Promotion and Disease Prevention Directorate, Malta
Physical activity strategy for the WHO European Region
2016–2025
REGIONAL COMMITTEE FOR EUROPE 65TH SESSION
Vilnius, Lithuania, 14–17 September 2015
Working document

OtherEUActivityonActiveAgeing• Actionresearchthrough3yearmulti-siteprogrammes,multipletopics
• 20+differentplatforms• Significantlackofdisseminationofresultsandlessons
• Permanentfeatures– EGREPA,ECSS,EUGMS• Collaborativeactivity- RomeStatement(2016)submittedtoEU– seekingcoordination

2.Falls- policyandimplementationinEurope
• Evidence-WHOHealthEvidenceNetwork(SkeltonandTodd2004)
• NBNomedicalcharityhome/support
• Evidence- Profaneprogramme –2003– 2007
• Policy - WHOGlobalreport2007

Falls– policyandimplementationinEurope
• Disseminationandimplementationofbestpractice- 17EUCountries
• Communitiesofinterest,resourcesandcascadetraining
• Falls,independenceandtechnology
• Policystatement- “Fallspreventioniseveryone’sbusiness”EuropeanStakeholdersAllianceforActiveAgeingthroughFallsPrevention(ESA)JointDeclaration2015
Thematicnetworks

Physicalactivityandageing– beginnings
• EmergingPhysicalActivityandHealthPolicy• (previouslydomainofvoluntarysector,both
ageingandmovementanddance)• 1996ActiveforLifeOlderPeople(1year
campaignremoderate physicalactivitymessage)
• 1997ActiveforLaterLife(1st NationalConference)
• LaunchofADNFSfollowupdataonphysicalfunctionandolderpeople(HEA1999)

3.Fallspreventionpolicy-beginnings.
• DepartmentofHealth(1999)• ProfessionalGuidance- Physical
activityandthepreventionoffallsandaccidents
• Evidencebasedpractice• Professionalneedsanalysis
• DepartmentofTradeandIndustry• Publiceducationcampaign• SlipsTripsandBrokenHips”

Standard 6 Falls• The NHS, working in partnership with councils,
takes action to prevent falls and reduce resultant fractures/other injuries in their populations of older people.
• Older people who have fallen receive effective treatment
• (1) Prevention. • (2) Diagnosis & management. • (3) Rehabilitation and longer term care.
Standard 8 • the promotion of health and active life for
older people
Startingpoint- NationalServiceFramework
(DH2001)

Home based exercise programme
OTAGO
Chair Based Exercise Class
(Community based)
Exercise Referral Scheme
12 weeks
PSI/Rehab based exercise group
12 weeks
Community based classes for older people
OTAGO exercise classes
(Community based)
Falls AssessmentIdentification of a falls problem and screening to determine risk factors
Cambridgeshire Falls Prevention EXERCISE PATHWAY
Motivation Screening Pathway

Independently mobile older people
Independent with assistance/aids
Independent with assistance/aids/carer
Physically frail housebound/outpatient
Exercise Instructor NVQ2
OTAGO Exercise Leader Chair-based Exercise LeaderNVQ2/3
Dinan, 2004
Advanced Exercise InstructorExercise for the Older PersonNVQ3
Advanced Exercise InstructorExercise ReferralNVQ4
Specialist Exercise InstructorPostural StabilityNVQ4
Specialist Exercise InstructorClinical Exercise MSc
General Populations
Special Populations
Low Risk
Patient
Populations
Medium Risk
HighRisk
The UK Register of Exercise Professionals

Reaching the older public, education and information giving
Falls Awareness Week Action pack for event holders

Authoritativesupportfrom
• RoyalSocietyforthePreventionofAccidents• American/BritishGeriatricsSociety• CharteredSocietyofPhysiotherapy• NICEGuidance(2013/15)• RoyalColleges(incl.GPs,Nursing)• NationalOsteoporosisSociety• AmbulanceServicesandother1st responders• ResearchintoAgeing- AgeConcern,AgeUK

Falls– PHEconsensusstatement
• Movingforward- includes• Keyinterventions• Commissioningservices• Commitment- NationalFallsPreventionCoordinationGroup
• Supportedby16memberorganisations
• Tobereviewed2019
Falls and fracture consensus statement Supporting commissioning for prevention Produced by Public Health England with the National Falls Prevention Coordination
Group member organisations
January 2017 To be reviewed January 2019
(PHEJan2017)

Returnoninvestmentofpublichealthinterventions:asystematicreview
“Interventionsaimedatreducingratesoffallsareabletoshowoneoftheswiftestreturnsoninvestmentofanyofthepublichealth interventionsidentified
withinthisstudy”• CBRof20.6returnedwithin18 months.• Fallspreventioninterventions…….arerelativelylowcost(structuredexerciseprogrammes forthoseatriskoffalls),andyettheirpotentialimpactondemandmanagementforhospitalservicesisclearlydemonstrated.
• Shiftinginvestmentfromsecondarycareforthetreatmentoffallstoprimarypreventionwouldshowsignificantandswiftreturnsoninvestment.
MastersR,etalJournalofEpidemiologyandCommunityHealth(2017)

4.Strengtheningphysicalactivitypolicy
• 2000onwards- successionofpolicydocumentsrelatingtoageing
• Physicalactivityandageinglaggingbehind(determinedby PA/sportpolicypriority)
• Demandsforevidencebasedpractice
• AtLeast5aweek– chapter6,OlderAdults(DH2004)
• Enthusiastsandfrontrunners(AgeUK,FootballFoundation)

Leadership,interestandresponsibility?
Health
Localgovernment
Voluntarysector

Strengtheningthecaseforpolicy- ashift?
6Keyelements……butRecommendationson
StrengthBalance
SedentarybehaviourUKCMOPhysicalActivityGuidelinesforOlderAdults
(65+)(DH2011)

Whatisfunctionalfitness?
“FunctionalFitnessperformanceishavingthephysiologicalcapacitytoperformnormaleverydayactivitiessafelyandindependentlywithoutunduefatigue”.
(Rikli @Jones1999)
Greaterpriorityinlaterlife?

Howimportantisit?
“……itislogicalandpossiblysafertosuggestthatolderadultswhosemobilityiscompromisedstartby
increasingtheirstrengthandimprovingtheirbalancebeforeembarkingonaerobic
training”.
WHOWorldReportonAgeingandHealth(Oct2015)
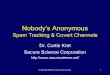
Overall (I-squared = 61.5%, p = 0.000)
Ebrahim, 1997
Barnett, 2003
Woo, Tai Chi, 2007
Luukinen, 2007
Campbell, 2005
Schoenfelder, 2000
Sihvonen, 2004
Lord, 2003
Buchner, 1997
Author,
Nowalk, Tai Chi, 2001
Mulrow, 1994
Day, 2002
Reinsch, 1992
Skelton, 2005
Wolf, Balance, 1996
Woo, Resistance, 2007
Wolf, Tai Chi, 1996
year
McMurdo, 1997
Korpelainen, 2006
Morgan, 2004
Campbell, 1999
Hauer, 2001
Voukelatos, 2007
Faber, Functional walking, 2006
Li, 2005
Lord, 1995
Schnelle, 2003
Steinberg, 2000
Faber, Tai Chi, 2006
Liu-Ambrose, Resistance, 2004
Lin, 2007
Bunout, 2005
Liu-Ambrose, Agility, 2004
Resnick, 2002
Latham, 2003
Madureira, 2007
Carter, 2002
Green, 2002
Toulotte, 2003
Wolf, 2003
Cerny, 1998
Sakamoto, 2006Rubenstein, 2000
Means, 2005
Protas, 2006
Suzuki, 2004
Campbell, 1997
Nowalk, Resist./Endurance, 2001
Robertson, 2001
0.83 (0.75, 0.91)
1.29 (0.90, 1.83)
0.60 (0.36, 0.99)
0.49 (0.24, 0.99)
0.93 (0.80, 1.09)
1.15 (0.82, 1.61)
3.06 (1.61, 5.82)
0.38 (0.17, 0.87)
0.78 (0.62, 0.99)
0.61 (0.40, 0.94)
Effect
0.77 (0.46, 1.28)
1.26 (0.90, 1.76)
0.82 (0.70, 0.97)
1.24 (0.77, 1.98)
0.69 (0.50, 0.96)
0.98 (0.71, 1.34)
0.78 (0.41, 1.48)
0.51 (0.36, 0.72)
size (95% CI)
0.53 (0.28, 0.98)
0.79 (0.59, 1.05)
1.05 (0.66, 1.68)
0.87 (0.36, 2.10)
0.75 (0.46, 1.25)
0.67 (0.46, 0.97)
1.32 (1.03, 1.69)
0.45 (0.33, 0.62)
0.85 (0.57, 1.27)
0.62 (0.38, 1.00)
0.90 (0.79, 1.03)
0.96 (0.76, 1.22)
1.80 (0.67, 4.85)
0.67 (0.32, 1.41)
1.22 (0.70, 2.14)
1.03 (0.36, 2.98)
0.71 (0.04, 11.58)
1.08 (0.87, 1.35)
0.48 (0.25, 0.93)
0.88 (0.32, 2.41)
1.34 (0.87, 2.07)
0.08 (0.00, 1.37)
0.75 (0.52, 1.08)
0.87 (0.17, 4.29)
0.82 (0.64, 1.04)0.90 (0.42, 1.91)
0.41 (0.21, 0.77)
0.62 (0.26, 1.48)
0.35 (0.14, 0.90)
0.68 (0.52, 0.89)
0.96 (0.63, 1.46)
0.54 (0.32, 0.91)
100.00
2.64
1.88
1.22
3.85
2.74
1.40
0.98
3.38
2.21
%
1.88
2.75
3.80
2.04
2.81
2.86
1.41
2.67
Weight
1.48
3.05
2.04
0.88
1.89
2.56
3.31
2.87
2.38
1.98
3.97
3.34
0.72
1.13
1.67
0.65
0.11
3.46
1.34
0.70
2.21
0.10
2.58
0.31
3.341.11
1.40
0.88
0.80
3.13
2.27
1.84
0.83 (0.75, 0.91)
1.29 (0.90, 1.83)
0.60 (0.36, 0.99)
0.49 (0.24, 0.99)
0.93 (0.80, 1.09)
1.15 (0.82, 1.61)
3.06 (1.61, 5.82)
0.38 (0.17, 0.87)
0.78 (0.62, 0.99)
0.61 (0.40, 0.94)
Effect
0.77 (0.46, 1.28)
1.26 (0.90, 1.76)
0.82 (0.70, 0.97)
1.24 (0.77, 1.98)
0.69 (0.50, 0.96)
0.98 (0.71, 1.34)
0.78 (0.41, 1.48)
0.51 (0.36, 0.72)
size (95% CI)
0.53 (0.28, 0.98)
0.79 (0.59, 1.05)
1.05 (0.66, 1.68)
0.87 (0.36, 2.10)
0.75 (0.46, 1.25)
0.67 (0.46, 0.97)
1.32 (1.03, 1.69)
0.45 (0.33, 0.62)
0.85 (0.57, 1.27)
0.62 (0.38, 1.00)
0.90 (0.79, 1.03)
0.96 (0.76, 1.22)
1.80 (0.67, 4.85)
0.67 (0.32, 1.41)
1.22 (0.70, 2.14)
1.03 (0.36, 2.98)
0.71 (0.04, 11.58)
1.08 (0.87, 1.35)
0.48 (0.25, 0.93)
0.88 (0.32, 2.41)
1.34 (0.87, 2.07)
0.08 (0.00, 1.37)
0.75 (0.52, 1.08)
0.87 (0.17, 4.29)
0.82 (0.64, 1.04)0.90 (0.42, 1.91)
0.41 (0.21, 0.77)
0.62 (0.26, 1.48)
0.35 (0.14, 0.90)
0.68 (0.52, 0.89)
0.96 (0.63, 1.46)
0.54 (0.32, 0.91)
100.00
2.64
1.88
1.22
3.85
2.74
1.40
0.98
3.38
2.21
%
1.88
2.75
3.80
2.04
2.81
2.86
1.41
2.67
Weight
1.48
3.05
2.04
0.88
1.89
2.56
3.31
2.87
2.38
1.98
3.97
3.34
0.72
1.13
1.67
0.65
0.11
3.46
1.34
0.70
2.21
0.10
2.58
0.31
3.341.11
1.40
0.88
0.80
3.13
2.27
1.84
Favours exercise Favours control
1.25 .5 1 2 4
(Sherringtonetal2011)

Shiftinpolicy- independence
Independenceiscommonlyunderstoodastheabilitytoperformfunctionsrelatedto
dailyliving– i.e.thecapacityofliving
independentlyinthecommunitywithnoand/orlittlehelpfromothers.
What’simportanttopeopleastheyage?

PolicyfocusacrossthelaterlifecontinuumTargetpopulation Policy focusand
outcomesPotential partners
EnteringoldageActivesGoal– buildandmaintaincapacity
Healthimprovementmaintainingandincreasingphysicalactivitylevels
Primarycare,physicalactivity,sport,recreationproviders andservices
ThoseintransitionGoal- reverse,stoporslowthelossofcapacity
Initiatingandmaintainingphysicalactivitytoimprove/maintainhealth,functionandindependence
Primary careandincontactwithadult,health/social/careservices,voluntarysector,housingandsupportservices
Frailer,olderpeopleGoal – compensateforlossofcapacity
Qualityoflifeandperformanceofactivitiesofdailyliving
Somewithhighlevelsofsupportathome,manyinresidentialcare
(WHO1996/2015,DH2001/11)

Compliance– servicesandinterventions
• Evidencebasedpractice/interventionsinfallsprevention– 50hours,(9months)tailoredandprogressivestrengthandbalance(Sherrington2011)
– SupportandguidancefromNICE,AGS/BGSRCGP• But
– NHSservices10hours=then??????– Behavioural changestrategiesnotreplicated– More“userfriendly”activitiesdesireable?

Externalcircumstancesimposeconstraints
• Realageingpolicypriorities?– Employmentandpensions– Healthandsocialcare– Demographicchanges(eg,older,olderpopulations(85+)
– Lonelinessandisolationwww.cpa.org.uk - www.ilcuk.org.uk -
www.ageuk.org.uk• Evidencebasedpractice• Ecologicalmodelandenvironmentalchange

UpdatingtheEvidencePhysicalActivityandOlderAdults(65+)
BaumannetalGerontologist(2016)

Theevidence– whatworks?
• Systematicreviews• Lacksreferenceto“bestpractice”programs
• Increasingevidencefromtranslationalresearch
• Behavioural change• Youngerolderpeopleandoldest,oldandfrailpeople
(Baumannetal2016)
So?• Scalingupthrough• Replicationofmodelprogrammes (egREAIM)
Or?• Capacitytodesignfrombestpracticeprinciples?
And….• ReturnonInvestment
Tailored,personaladvice,supportedthroughbehaviour changeovertime

Scalingupthroughenvironmentalchange
“Supportedbytheirenvironment, mostpeopleaged80+livinginthecommunity,canexpecttocontinuetogooutdoors
daily,engageinarangeofactivitiesandmaintainqualityoflifeintooldest
age”.(IDGO20120
LivingStreets“StreetAudits- Damagedorunevenpavementsandpavement
parking,lackofbenches/restingplaces,publictoilets,safercrossings’.
www.livingstreets.org.uk

Ageing(still)anegativeagenda?
• MediaprofileofdemandsonNHSandAdultandSocialService(bedblocking/burden/drain)
• Care- repeatedlykickedintothelonggrass• Morepeopleover65thanunder16– physicalactivityremainsschoolsandyouthfocused.
• Stayingyoungorgrowingold(dis)gracefully• Nike(DesigntoMove)– “notgoodforourimage”

Conclusions?Activeageingoffers“onesizefitsall”foradiverse
population• Multiplepolicydimensions,players andactors• FindingclarityforActiveAgeingwithinphysicalactivitypolicy
• FindingclarityforphysicalactivitywithinActiveAgeing• Westilldon’thavetherightsortofevidence• Individualorsocietal(environmental)change• Independenceandconflictwithnon-communicablediseaseaspolicyfocus